-
Commentary
No one is better than all together: the role of networks in pediatric intensive care
Rev Bras Ter Intensiva. 2019;31(3):277-281
Abstract
CommentaryNo one is better than all together: the role of networks in pediatric intensive care
Rev Bras Ter Intensiva. 2019;31(3):277-281
DOI 10.5935/0103-507X.20190043
Views1INTRODUCTION Pediatric critical illness is a rare event. Crow et al. recently showed how unusual it is for a child to be admitted to a pediatric intensive care unit (PICU).() Although infrequent from a population-based standpoint, common PICU conditions (such as sepsis) represent an international threat, and significant disparities in outcomes still prevail in resource-limited […]See moreViews1

Abstract
CommentaryNo one is better than all together: the role of networks in pediatric intensive care
Rev Bras Ter Intensiva. 2019;31(3):277-281
DOI 10.5935/0103-507X.20190043
Views1INTRODUCTIONPediatric critical illness is a rare event. Crow et al. recently showed how unusual it is for a child to be admitted to a pediatric intensive care unit (PICU).() Although infrequent from a population-based standpoint, common PICU conditions (such as sepsis) represent an international threat, and significant disparities in outcomes still prevail in resource-limited settings.(,)Children […]See more
-
Original Articles
Activation of extracorporeal membrane oxygenation: a therapeutic approach to be considered
- Isabel Araújo
 ,
, - Pedro Raul,
- Francisca Monteiro,
- Mágui Lobo,
- Marta Rodrigues, [ … ],
- Filipe Fernandes
Abstract
Original ArticlesActivation of extracorporeal membrane oxygenation: a therapeutic approach to be considered
Rev Bras Ter Intensiva. 2019;31(3):282-288
DOI 10.5935/0103-507X.20190053
Views0See moreABSTRACT
Objective:
To describe the epidemiological profile of victims of cardiac arrest assisted using a nontransporting emergency medical service vehicle and to determine whether these patients met the criteria for the use of extracorporeal membrane oxygenation.
Methods:
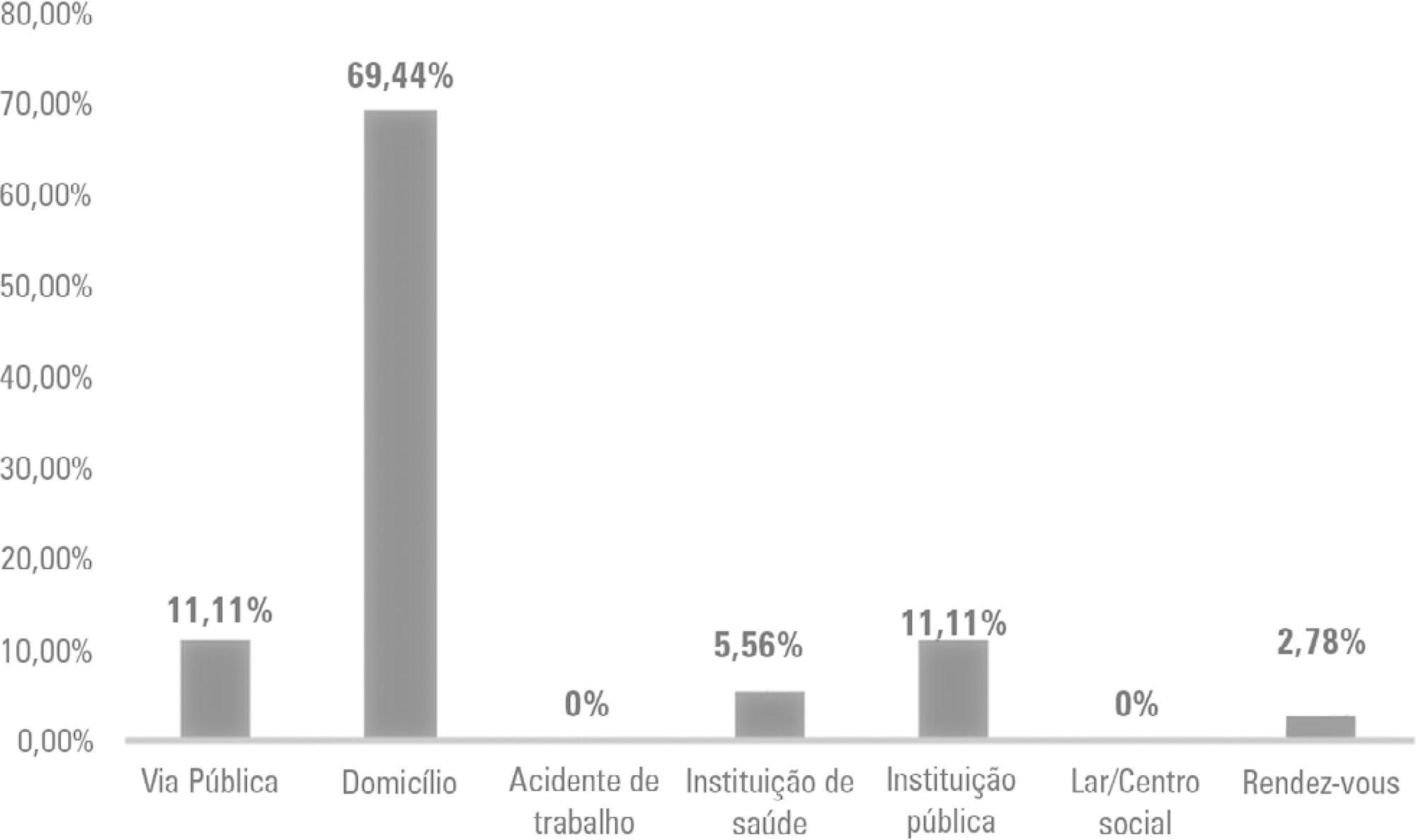
This study employed a retrospective, cohort, descriptive, and exploratory design. Data were collected in January 2018 in northern Portugal by consulting the records of nontransporting emergency medical service vehicles that provided assistance between 2012 and 2016. An observation grid was prepared that was supported by the instrument used for collecting data from the national registry of out-ofhospital cardiac arrests.
Results:
After applying the inclusion criteria, the sample consisted of 36 victims. Extracorporeal membrane oxygenation could have been applied to 24 victims during the period analyzed, which might have increased the odds for transplantation, survival, or both, for either the victim or other individuals.
Conclusion:
Nontransporting emergency medical service vehicles have the potential for inclusion in the extracorporeal membrane oxygenation network of the study area.
Views0Abstract
Original ArticlesActivation of extracorporeal membrane oxygenation: a therapeutic approach to be considered
Rev Bras Ter Intensiva. 2019;31(3):282-288
DOI 10.5935/0103-507X.20190053
Views0See moreABSTRACT
Objective:
To describe the epidemiological profile of victims of cardiac arrest assisted using a nontransporting emergency medical service vehicle and to determine whether these patients met the criteria for the use of extracorporeal membrane oxygenation.
Methods:
This study employed a retrospective, cohort, descriptive, and exploratory design. Data were collected in January 2018 in northern Portugal by consulting the records of nontransporting emergency medical service vehicles that provided assistance between 2012 and 2016. An observation grid was prepared that was supported by the instrument used for collecting data from the national registry of out-ofhospital cardiac arrests.
Results:
After applying the inclusion criteria, the sample consisted of 36 victims. Extracorporeal membrane oxygenation could have been applied to 24 victims during the period analyzed, which might have increased the odds for transplantation, survival, or both, for either the victim or other individuals.
Conclusion:
Nontransporting emergency medical service vehicles have the potential for inclusion in the extracorporeal membrane oxygenation network of the study area.
- Isabel Araújo
-
Original Articles
Acute effects of ventilator hyperinflation with increased inspiratory time on respiratory mechanics: randomized crossover clinical trial
Rev Bras Ter Intensiva. 2019;31(3):289-295
Abstract
Original ArticlesAcute effects of ventilator hyperinflation with increased inspiratory time on respiratory mechanics: randomized crossover clinical trial
Rev Bras Ter Intensiva. 2019;31(3):289-295
DOI 10.5935/0103-507X.20190052
Views1ABSTRACT
Objective:
To evaluate the effects of ventilator hyperinflation on respiratory mechanics.
Methods:
A randomized crossover clinical trial was conducted with 38 mechanically ventilated patients with pulmonary infection. The order of the hyperinflation and control (without changes in the parameters) conditions was randomized. Hyperinflation was performed for 5 minutes in pressure-controlled ventilation mode, with progressive increases of 5cmH2O until a maximum pressure of 35cmH2O was reached, maintaining positive end expiratory pressure. After 35cmH2O was reached, the inspiratory time and respiratory rate were adjusted so that the inspiratory and expiratory flows reached baseline levels. Measurements of static compliance, total resistance and airway resistance, and peak expiratory flow were evaluated before the technique, immediately after the technique and after aspiration. Two-way analysis of variance for repeated measures was used with Tukey’s post hoc test, and p < 0.05 was considered significant.
Results:
Ventilator hyperinflation increased static compliance, which remained at the same level after aspiration (46.2 ± 14.8 versus 52.0 ± 14.9 versus 52.3 ± 16.0mL/cmH2O; p < 0.001). There was a transient increase in airway resistance (6.6 ± 3.6 versus 8.0 ± 5.5 versus 6.6 ± 3.5cmH2O/Ls-1; p < 0.001) and a transient reduction in peak expiratory flow (32.0 ± 16.0 versus 29.8 ± 14.8 versus 32.1 ± 15.3Lpm; p <0.05) immediately after the technique; these values returned to pretechnique levels after tracheal aspiration. There were no changes in the control condition, nor were hemodynamic alterations observed.
Conclusion:
Ventilator hyperinflation promoted increased compliance associated with a transient increase in airway resistance and peak expiratory flow, with reduction after aspiration.
Keywords:Physical therapy modalitiesPositive pressure respirationRespiration, artificialRespiratory care unitsRespiratory mechanicsRespiratory therapy/methodsSee moreViews1Abstract
Original ArticlesAcute effects of ventilator hyperinflation with increased inspiratory time on respiratory mechanics: randomized crossover clinical trial
Rev Bras Ter Intensiva. 2019;31(3):289-295
DOI 10.5935/0103-507X.20190052
Views1ABSTRACT
Objective:
To evaluate the effects of ventilator hyperinflation on respiratory mechanics.
Methods:
A randomized crossover clinical trial was conducted with 38 mechanically ventilated patients with pulmonary infection. The order of the hyperinflation and control (without changes in the parameters) conditions was randomized. Hyperinflation was performed for 5 minutes in pressure-controlled ventilation mode, with progressive increases of 5cmH2O until a maximum pressure of 35cmH2O was reached, maintaining positive end expiratory pressure. After 35cmH2O was reached, the inspiratory time and respiratory rate were adjusted so that the inspiratory and expiratory flows reached baseline levels. Measurements of static compliance, total resistance and airway resistance, and peak expiratory flow were evaluated before the technique, immediately after the technique and after aspiration. Two-way analysis of variance for repeated measures was used with Tukey’s post hoc test, and p < 0.05 was considered significant.
Results:
Ventilator hyperinflation increased static compliance, which remained at the same level after aspiration (46.2 ± 14.8 versus 52.0 ± 14.9 versus 52.3 ± 16.0mL/cmH2O; p < 0.001). There was a transient increase in airway resistance (6.6 ± 3.6 versus 8.0 ± 5.5 versus 6.6 ± 3.5cmH2O/Ls-1; p < 0.001) and a transient reduction in peak expiratory flow (32.0 ± 16.0 versus 29.8 ± 14.8 versus 32.1 ± 15.3Lpm; p <0.05) immediately after the technique; these values returned to pretechnique levels after tracheal aspiration. There were no changes in the control condition, nor were hemodynamic alterations observed.
Conclusion:
Ventilator hyperinflation promoted increased compliance associated with a transient increase in airway resistance and peak expiratory flow, with reduction after aspiration.
Keywords:Physical therapy modalitiesPositive pressure respirationRespiration, artificialRespiratory care unitsRespiratory mechanicsRespiratory therapy/methodsSee more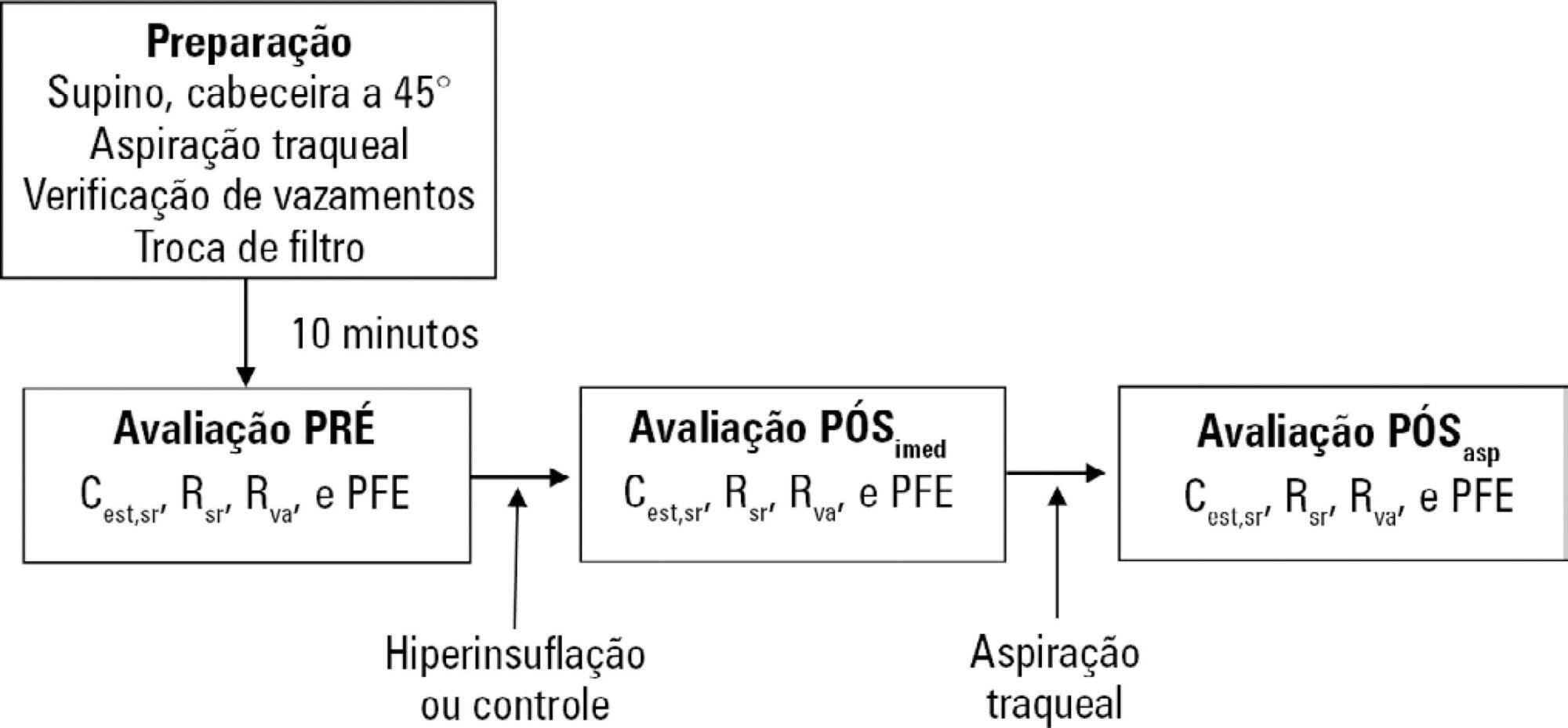
-
Original Articles
Autonomic responses of premature newborns to body position and environmental noise in the neonatal intensive care unit
- Evelim Leal de Freitas Dantas Gomes ,
- Camilla Malta dos Santos,
- Anelise da Costa Souza Santos,
- Aline Gomes da Silva,
- Mariza Aparecida Malaquias França, [ … ],
- Dirceu Costa
Abstract
Original ArticlesAutonomic responses of premature newborns to body position and environmental noise in the neonatal intensive care unit
Rev Bras Ter Intensiva. 2019;31(3):296-302
DOI 10.5935/0103-507X.20190054
- Evelim Leal de Freitas Dantas Gomes ,
- Camilla Malta dos Santos,
- Anelise da Costa Souza Santos,
- Aline Gomes da Silva,
- Mariza Aparecida Malaquias França,
- Dyele Souza Romanini,
- Manoela Cristina Veiga de Mattos,
- Andrea Fernanda Leal,
- Dirceu Costa
Views0See moreABSTRACT
Objective:
Evaluate the physiological and autonomic nervous system responses of premature newborns to body position and noise in the neonatal intensive care unit.
Methods:
A quasi-experimental study. The autonomic nervous system of newborns was evaluated based on heart rate variability when the newborns were exposed to environmental noise and placed in different positions: supine without support, supine with manual restraint and prone.
Results:
Fifty premature newborns were evaluated (gestational age: 32.6 ± 2.3 weeks; weight: 1816 ± 493g; and Brazelton sleep/awake level: 3 to 4). A positive correlation was found between environmental noise and sympathetic activity (R = 0.27, p = 0.04). The mean environmental noise was 53 ± 14dB. The heart rate was higher in the supine position than in the manual restraint and prone positions (148.7 ± 21.6, 141.9 ± 16 and 144 ± 13, respectively) (p = 0.001). Sympathetic activity, represented by a low frequency index, was higher in the supine position (p < 0.05) than in the other positions, and parasympathetic activity (high frequency, root mean square of the sum of differences between normal adjacent mean R-R interval and percentage of adjacent iRR that differed by more than 50ms) was higher in the prone position (p < 0.05) than in the other positions. The complexity of the autonomic adjustments (approximate entropy and sample entropy) was lower in the supine position than in the other positions.
Conclusion:
The prone position and manual restraint position increased both parasympathetic activity and the complexity of autonomic adjustments in comparison to the supine position, even in the presence of higher environmental noise than the recommended level, which tends to increase sympathetic activity.
Views0Abstract
Original ArticlesAutonomic responses of premature newborns to body position and environmental noise in the neonatal intensive care unit
Rev Bras Ter Intensiva. 2019;31(3):296-302
DOI 10.5935/0103-507X.20190054
- Evelim Leal de Freitas Dantas Gomes ,
- Camilla Malta dos Santos,
- Anelise da Costa Souza Santos,
- Aline Gomes da Silva,
- Mariza Aparecida Malaquias França,
- Dyele Souza Romanini,
- Manoela Cristina Veiga de Mattos,
- Andrea Fernanda Leal,
- Dirceu Costa
Views0See moreABSTRACT
Objective:
Evaluate the physiological and autonomic nervous system responses of premature newborns to body position and noise in the neonatal intensive care unit.
Methods:
A quasi-experimental study. The autonomic nervous system of newborns was evaluated based on heart rate variability when the newborns were exposed to environmental noise and placed in different positions: supine without support, supine with manual restraint and prone.
Results:
Fifty premature newborns were evaluated (gestational age: 32.6 ± 2.3 weeks; weight: 1816 ± 493g; and Brazelton sleep/awake level: 3 to 4). A positive correlation was found between environmental noise and sympathetic activity (R = 0.27, p = 0.04). The mean environmental noise was 53 ± 14dB. The heart rate was higher in the supine position than in the manual restraint and prone positions (148.7 ± 21.6, 141.9 ± 16 and 144 ± 13, respectively) (p = 0.001). Sympathetic activity, represented by a low frequency index, was higher in the supine position (p < 0.05) than in the other positions, and parasympathetic activity (high frequency, root mean square of the sum of differences between normal adjacent mean R-R interval and percentage of adjacent iRR that differed by more than 50ms) was higher in the prone position (p < 0.05) than in the other positions. The complexity of the autonomic adjustments (approximate entropy and sample entropy) was lower in the supine position than in the other positions.
Conclusion:
The prone position and manual restraint position increased both parasympathetic activity and the complexity of autonomic adjustments in comparison to the supine position, even in the presence of higher environmental noise than the recommended level, which tends to increase sympathetic activity.

- Evelim Leal de Freitas Dantas Gomes
-
Original Articles
Update of the diagnostic criteria of brain death: application and training of physicians
- José Antonio Chehuen Neto,
- Renato Erothildes Ferreira,
- Igor Malheiros Assad ,
- Ivy Alves Santos,
- João Luís Carvalho Tricote dos Santos, [ … ],
- Sávio Dornelas Breder
Abstract
Original ArticlesUpdate of the diagnostic criteria of brain death: application and training of physicians
Rev Bras Ter Intensiva. 2019;31(3):303-311
DOI 10.5935/0103-507X.20190055
- José Antonio Chehuen Neto,
- Renato Erothildes Ferreira,
- Igor Malheiros Assad ,
- Ivy Alves Santos,
- João Luís Carvalho Tricote dos Santos,
- Luíza Campos de Paula,
- Sávio Dornelas Breder
Views6ABSTRACT
Objective:
To evaluate the medical knowledge regarding the application of the diagnostic criteria for brain death and to correlate it with training parameters for this diagnosis according to Federal Council of Medicine resolution 2,173 of 2017.
Method:
We interviewed 174 physicians with experience with comatose patients. A structured questionnaire adapted from previous studies was used. The associations of the variables were tested using the chi-square test for independence. A multivariate logistic model was fitted for associations with p values ≤ 0.20.
Results:
Among the interviewees, 40% had been working for more than 1 year in intensive care, and 23% had initiated ten or more brain death protocols complying with the new resolution. Forty-five percent of the interviewees reported having difficulty following the criteria, 94% acknowledged the need for complementary tests for diagnosis, and 8% of them reported the existence of incorrect tests. The difficulty with these criteria decreased with an increase in the number of years of medical training (OR = 0.487; p = 0.045; 95%CI 0.241 – 0.983) and with a higher number of initiated brain death protocols (OR = 0.223; p = 0.0001; 95%CI 0.117 – 0.424).
Conclusions:
Difficulties in the application of brain death criteria were identified by a significant portion of the sample. However, among other factors, more years of training and a greater number of initiated brain death protocols were associated with greater ease in the application of brain death criteria according to the guidelines provided in Resolution 2,173 of the Federal Council of Medicine.
Keywords:Brain death/diagnosisBrain death/legislation & jurisprudenceEthics, medicalPhysician's roleTissue and organ procurementSee moreViews6Abstract
Original ArticlesUpdate of the diagnostic criteria of brain death: application and training of physicians
Rev Bras Ter Intensiva. 2019;31(3):303-311
DOI 10.5935/0103-507X.20190055
- José Antonio Chehuen Neto,
- Renato Erothildes Ferreira,
- Igor Malheiros Assad ,
- Ivy Alves Santos,
- João Luís Carvalho Tricote dos Santos,
- Luíza Campos de Paula,
- Sávio Dornelas Breder
Views6ABSTRACT
Objective:
To evaluate the medical knowledge regarding the application of the diagnostic criteria for brain death and to correlate it with training parameters for this diagnosis according to Federal Council of Medicine resolution 2,173 of 2017.
Method:
We interviewed 174 physicians with experience with comatose patients. A structured questionnaire adapted from previous studies was used. The associations of the variables were tested using the chi-square test for independence. A multivariate logistic model was fitted for associations with p values ≤ 0.20.
Results:
Among the interviewees, 40% had been working for more than 1 year in intensive care, and 23% had initiated ten or more brain death protocols complying with the new resolution. Forty-five percent of the interviewees reported having difficulty following the criteria, 94% acknowledged the need for complementary tests for diagnosis, and 8% of them reported the existence of incorrect tests. The difficulty with these criteria decreased with an increase in the number of years of medical training (OR = 0.487; p = 0.045; 95%CI 0.241 – 0.983) and with a higher number of initiated brain death protocols (OR = 0.223; p = 0.0001; 95%CI 0.117 – 0.424).
Conclusions:
Difficulties in the application of brain death criteria were identified by a significant portion of the sample. However, among other factors, more years of training and a greater number of initiated brain death protocols were associated with greater ease in the application of brain death criteria according to the guidelines provided in Resolution 2,173 of the Federal Council of Medicine.
Keywords:Brain death/diagnosisBrain death/legislation & jurisprudenceEthics, medicalPhysician's roleTissue and organ procurementSee more -
Original Articles
Respiratory distress syndrome: influence of management on the hemodynamic status of ≤ 32-week preterm infants in the first 24 hours of life
- Daniela Matos Fiorenzano ,
- Gabriela Nunes Leal,
- Karen Saori Shiraishi Sawamura,
- Alessandro Cavalcanti Lianza,
- Werther Brunow de Carvalho, [ … ],
- Vera Lúcia Jornada Krebs
Abstract
Original ArticlesRespiratory distress syndrome: influence of management on the hemodynamic status of ≤ 32-week preterm infants in the first 24 hours of life
Rev Bras Ter Intensiva. 2019;31(3):312-317
DOI 10.5935/0103-507X.20190056
- Daniela Matos Fiorenzano ,
- Gabriela Nunes Leal,
- Karen Saori Shiraishi Sawamura,
- Alessandro Cavalcanti Lianza,
- Werther Brunow de Carvalho,
- Vera Lúcia Jornada Krebs
Views0ABSTRACT
Objective:
To investigate the influence of respiratory distress syndrome management on clinical and echocardiographic parameters used for hemodynamic evaluation in ≤ 32- week newborns.
Methods:
Thirty-three ≤ 32-week newborns were prospectively evaluated and subjected to invasive mechanical ventilation. The need for exogenous surfactant and clinical and echocardiographic parameters in the first 24 hours of life was detailed in this group of patients.
Results:
The mean airway pressure was significantly higher in newborn infants who required inotropes [10.8 (8.8 – 23) cmH2O versus 9 (6.2 – 12) cmH2O; p = 0.04]. A negative correlation was found between the mean airway pressure and velocity-time integral of the pulmonary artery (r = -0.39; p = 0.026), right ventricular output (r = -0.43; p = 0.017) and measurements of the tricuspid annular plane excursion (r = -0.37; p = 0.036). A negative correlation was found between the number of doses of exogenous surfactant and the right ventricular output (r = -0.39; p = 0.028) and pulmonary artery velocity-time integral (r = -0.35; p = 0.043).
Conclusion:
In ≤ 32-week newborns under invasive mechanical ventilation, increases in the mean airway pressure and number of surfactant doses are correlated with the worsening of early cardiac function. Therefore, more aggressive management of respiratory distress syndrome may contribute to the hemodynamic instability of these patients.
Keywords:EchocardiographyHemodynamicsInfant, prematurePulmonary surfactantsRespiratory distress syndrome, newbornSee moreViews0Abstract
Original ArticlesRespiratory distress syndrome: influence of management on the hemodynamic status of ≤ 32-week preterm infants in the first 24 hours of life
Rev Bras Ter Intensiva. 2019;31(3):312-317
DOI 10.5935/0103-507X.20190056
- Daniela Matos Fiorenzano ,
- Gabriela Nunes Leal,
- Karen Saori Shiraishi Sawamura,
- Alessandro Cavalcanti Lianza,
- Werther Brunow de Carvalho,
- Vera Lúcia Jornada Krebs
Views0ABSTRACT
Objective:
To investigate the influence of respiratory distress syndrome management on clinical and echocardiographic parameters used for hemodynamic evaluation in ≤ 32- week newborns.
Methods:
Thirty-three ≤ 32-week newborns were prospectively evaluated and subjected to invasive mechanical ventilation. The need for exogenous surfactant and clinical and echocardiographic parameters in the first 24 hours of life was detailed in this group of patients.
Results:
The mean airway pressure was significantly higher in newborn infants who required inotropes [10.8 (8.8 – 23) cmH2O versus 9 (6.2 – 12) cmH2O; p = 0.04]. A negative correlation was found between the mean airway pressure and velocity-time integral of the pulmonary artery (r = -0.39; p = 0.026), right ventricular output (r = -0.43; p = 0.017) and measurements of the tricuspid annular plane excursion (r = -0.37; p = 0.036). A negative correlation was found between the number of doses of exogenous surfactant and the right ventricular output (r = -0.39; p = 0.028) and pulmonary artery velocity-time integral (r = -0.35; p = 0.043).
Conclusion:
In ≤ 32-week newborns under invasive mechanical ventilation, increases in the mean airway pressure and number of surfactant doses are correlated with the worsening of early cardiac function. Therefore, more aggressive management of respiratory distress syndrome may contribute to the hemodynamic instability of these patients.
Keywords:EchocardiographyHemodynamicsInfant, prematurePulmonary surfactantsRespiratory distress syndrome, newbornSee more - Daniela Matos Fiorenzano
-
Original Articles
Checklist for managing critical patients’ daily awakening
Rev Bras Ter Intensiva. 2019;31(3):318-325
Abstract
Original ArticlesChecklist for managing critical patients’ daily awakening
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
Views0See moreABSTRACT
Objective:
To validate the “Checklist for Managing Critical Patients’ Daily Awakening” instrument.
Methods:
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Results:
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
Conclusion:
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
Views0Abstract
Original ArticlesChecklist for managing critical patients’ daily awakening
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
Views0See moreABSTRACT
Objective:
To validate the “Checklist for Managing Critical Patients’ Daily Awakening” instrument.
Methods:
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Results:
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
Conclusion:
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
-
Original Articles
High nutritional risk is associated with unfavorable outcomes in patients admitted to an intensive care unit
- Julia Marchetti,
- Audrey Machado dos Reis,
- Amanda Forte dos Santos,
- Oellen Stuani Franzosi,
- Vivian Cristine Luft, [ … ],
- Thais Steemburgo
Abstract
Original ArticlesHigh nutritional risk is associated with unfavorable outcomes in patients admitted to an intensive care unit
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
- Julia Marchetti,
- Audrey Machado dos Reis,
- Amanda Forte dos Santos,
- Oellen Stuani Franzosi,
- Vivian Cristine Luft,
- Thais Steemburgo
Views1See moreABSTRACT
Objective:
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
Methods:
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients’ medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
Results:
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 – 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 – 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 – 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 – 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 – 6.44; p < 0.001).
Conclusion:
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.
Views1Abstract
Original ArticlesHigh nutritional risk is associated with unfavorable outcomes in patients admitted to an intensive care unit
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
- Julia Marchetti,
- Audrey Machado dos Reis,
- Amanda Forte dos Santos,
- Oellen Stuani Franzosi,
- Vivian Cristine Luft,
- Thais Steemburgo
Views1See moreABSTRACT
Objective:
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
Methods:
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients’ medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
Results:
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 – 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 – 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 – 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 – 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 – 6.44; p < 0.001).
Conclusion:
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.
-
Original Articles
Noninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
Abstract
Original ArticlesNoninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
DOI 10.5935/0103-507X.20190045
Views0ABSTRACT
Objective:
To describe the use of noninvasive ventilation to prevent tracheal intubation in children in a pediatric intensive care unit and to analyze the factors related to respiratory failure.
Methods:
A retrospective cohort study was performed from January 2016 to May 2018. The study population included children aged 1 to 14 years who were subjected to noninvasive ventilation as the first therapeutic choice for acute respiratory failure. Biological, clinical and managerial data were analyzed by applying a model with the variables that obtained significance ≤ 0.20 in a bivariate analysis. Logistic regression was performed using the ENTER method. The level of significance was set at 5%.
Results:
The children had a mean age of 68.7 ± 42.3 months, 96.6% had respiratory disease as a primary diagnosis, and 15.8% had comorbidities. Of the 209 patients, noninvasive ventilation was the first option for ventilatory support in 86.6% of the patients, and the fraction of inspired oxygen was ≥ 0.40 in 47% of the cases. The lethality rate was 1.4%. The data for the use of noninvasive ventilation showed a high success rate of 95.3% (84.32 – 106). The Pediatric Risk of Mortality (PRISM) score and the length of stay in the intensive care unit were the significant clinical variables for the success or failure of noninvasive ventilation.
Conclusion:
A high rate of effectiveness was found for the use of noninvasive ventilation for acute episodes of respiratory failure. A higher PRISM score on admission, comorbidities associated with respiratory symptoms and oxygen use ≥ 40% were independent factors related to noninvasive ventilation failure.
Keywords:ChildComorbidityIntensive care units, pediatricNoninvasive ventilationRespiratory insufficiencyVentilatory supportSee moreViews0Abstract
Original ArticlesNoninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
DOI 10.5935/0103-507X.20190045
Views0ABSTRACT
Objective:
To describe the use of noninvasive ventilation to prevent tracheal intubation in children in a pediatric intensive care unit and to analyze the factors related to respiratory failure.
Methods:
A retrospective cohort study was performed from January 2016 to May 2018. The study population included children aged 1 to 14 years who were subjected to noninvasive ventilation as the first therapeutic choice for acute respiratory failure. Biological, clinical and managerial data were analyzed by applying a model with the variables that obtained significance ≤ 0.20 in a bivariate analysis. Logistic regression was performed using the ENTER method. The level of significance was set at 5%.
Results:
The children had a mean age of 68.7 ± 42.3 months, 96.6% had respiratory disease as a primary diagnosis, and 15.8% had comorbidities. Of the 209 patients, noninvasive ventilation was the first option for ventilatory support in 86.6% of the patients, and the fraction of inspired oxygen was ≥ 0.40 in 47% of the cases. The lethality rate was 1.4%. The data for the use of noninvasive ventilation showed a high success rate of 95.3% (84.32 – 106). The Pediatric Risk of Mortality (PRISM) score and the length of stay in the intensive care unit were the significant clinical variables for the success or failure of noninvasive ventilation.
Conclusion:
A high rate of effectiveness was found for the use of noninvasive ventilation for acute episodes of respiratory failure. A higher PRISM score on admission, comorbidities associated with respiratory symptoms and oxygen use ≥ 40% were independent factors related to noninvasive ventilation failure.
Keywords:ChildComorbidityIntensive care units, pediatricNoninvasive ventilationRespiratory insufficiencyVentilatory supportSee more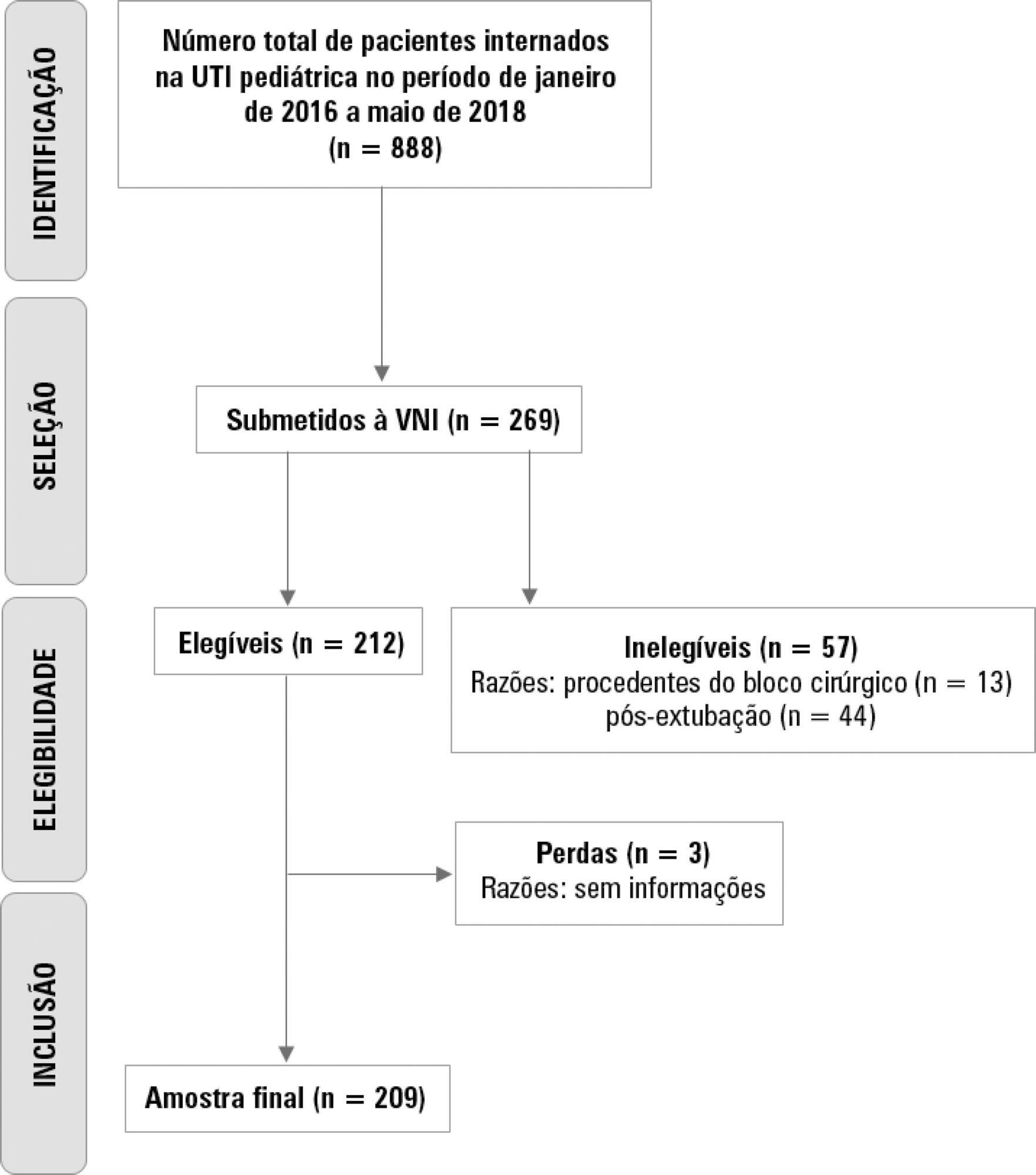
-
Original Articles
A past medical history of heart failure is associated with less fluid therapy in septic patients
Rev Bras Ter Intensiva. 2019;31(3):340-346
Abstract
Original ArticlesA past medical history of heart failure is associated with less fluid therapy in septic patients
Rev Bras Ter Intensiva. 2019;31(3):340-346
DOI 10.5935/0103-507X.20190049
Views1See moreABSTRACT
Objective:
To identify the underlying factors that affect fluid resuscitation in septic patients.
Methods:
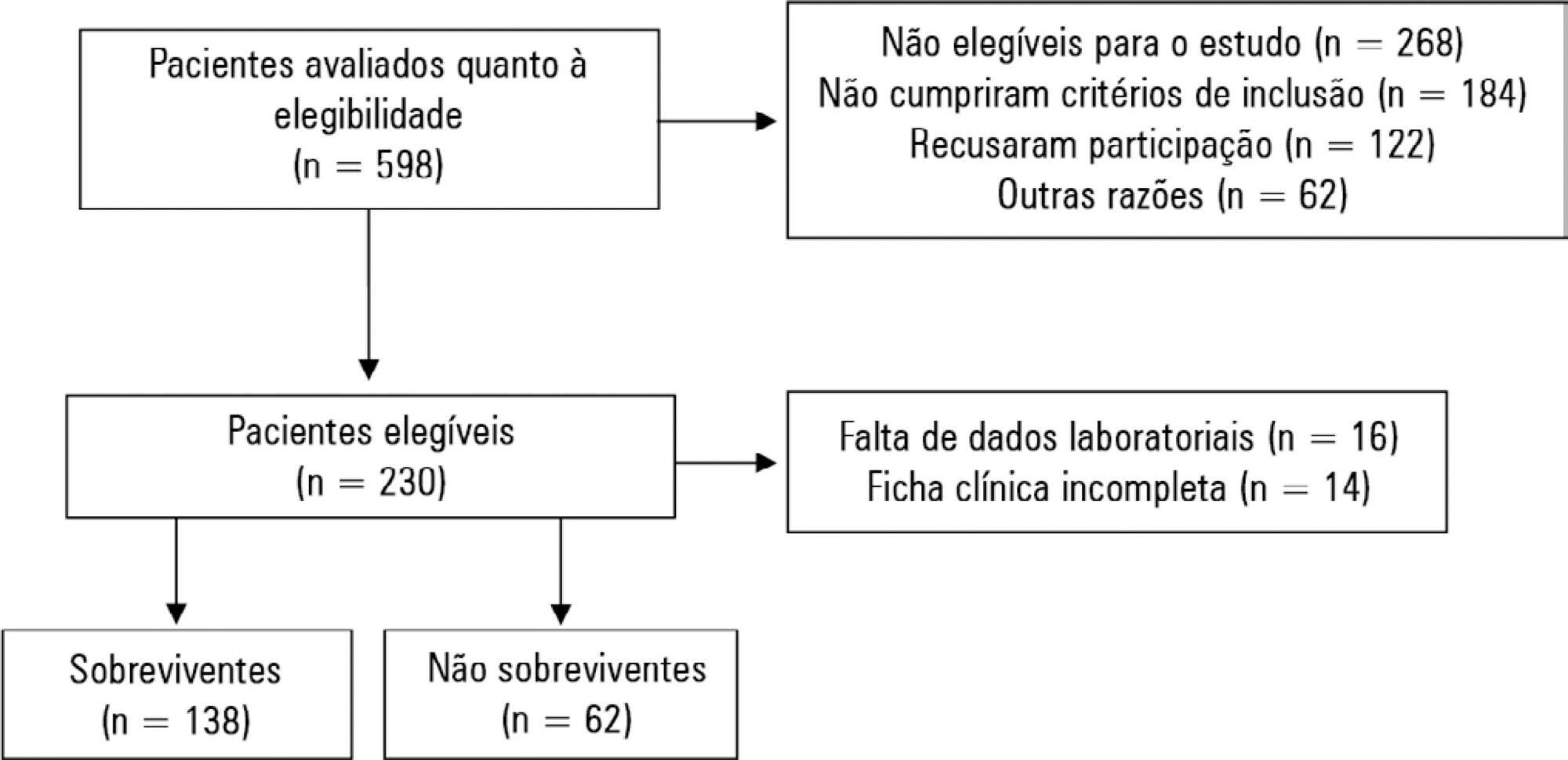
The present study was a case-control study of 181 consecutive patients admitted to a Medical Intensive Care Unit between 2012 and 2016 with a diagnosis of sepsis. Demographic, clinical, radiological and laboratory data were analyzed.
Results:
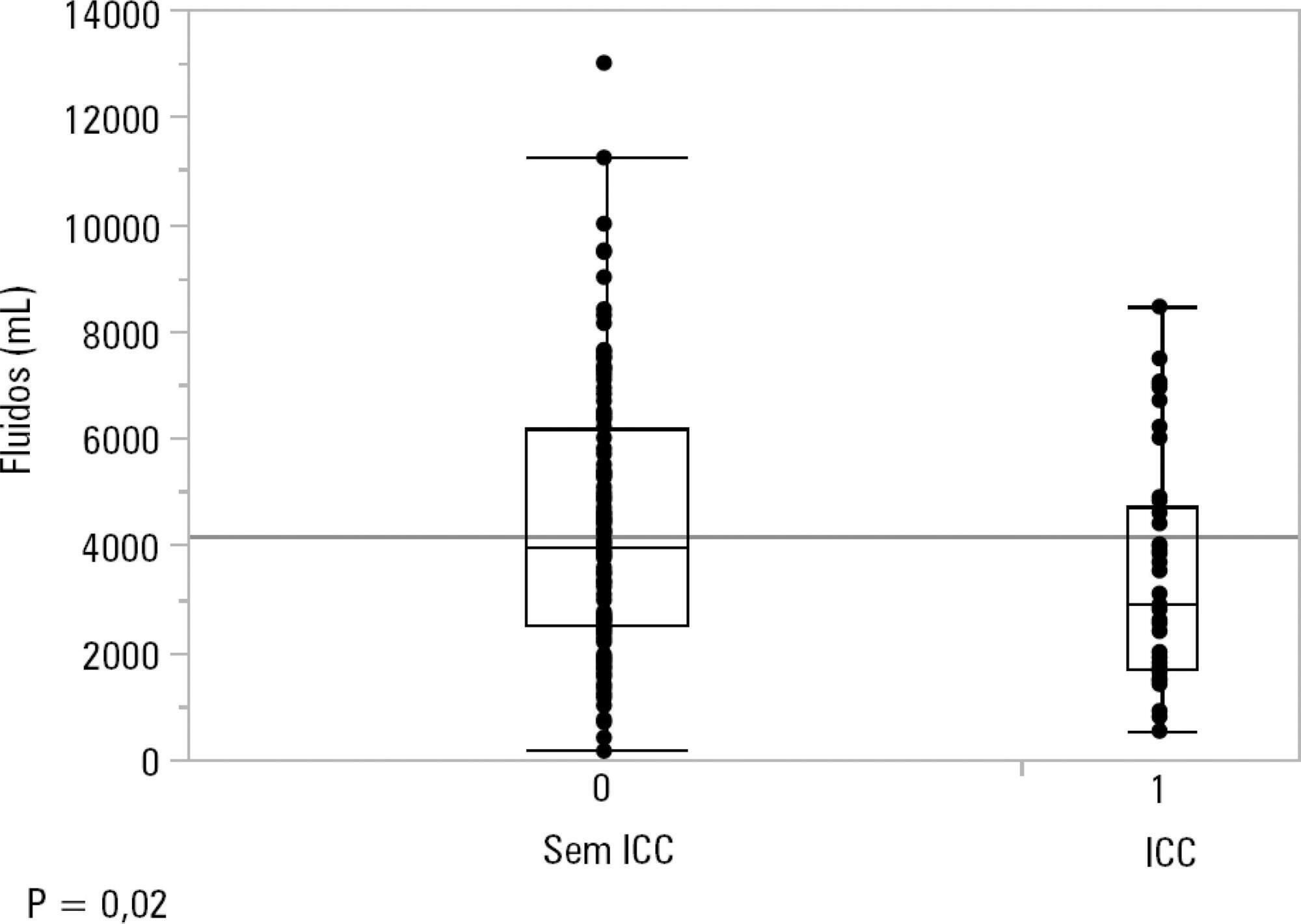
One hundred-thirty patients (72%) received ≥ 30mL/kg of IV fluids on admission. On univariate analyses, a past history of coronary artery disease and heart failure was associated with less fluid therapy. On multivariate analyses, a history of heart failure (OR = 2.31; 95%CI 1.04 – 5.14) remained significantly associated with receiving less IV fluids. Left ventricular ejection fraction, systolic/diastolic function, left ventricular hypertrophy and pulmonary hypertension were not associated with IV fluids. The amount of IV fluids was not associated with differences in mortality. During the first 24 hours, patients with a past history of heart failure received 2,900mLof IV fluids [1,688 – 4,714mL] versus 3,977mL [2,500 – 6,200mL] received by those without a history of heart failure, p = 0.02.
Conclusion:
Septic patients with a past history of heart failure received 1L less IV fluids in the first 24 hours with no difference in mortality.
Views1Abstract
Original ArticlesA past medical history of heart failure is associated with less fluid therapy in septic patients
Rev Bras Ter Intensiva. 2019;31(3):340-346
DOI 10.5935/0103-507X.20190049
Views1See moreABSTRACT
Objective:
To identify the underlying factors that affect fluid resuscitation in septic patients.
Methods:
The present study was a case-control study of 181 consecutive patients admitted to a Medical Intensive Care Unit between 2012 and 2016 with a diagnosis of sepsis. Demographic, clinical, radiological and laboratory data were analyzed.
Results:
One hundred-thirty patients (72%) received ≥ 30mL/kg of IV fluids on admission. On univariate analyses, a past history of coronary artery disease and heart failure was associated with less fluid therapy. On multivariate analyses, a history of heart failure (OR = 2.31; 95%CI 1.04 – 5.14) remained significantly associated with receiving less IV fluids. Left ventricular ejection fraction, systolic/diastolic function, left ventricular hypertrophy and pulmonary hypertension were not associated with IV fluids. The amount of IV fluids was not associated with differences in mortality. During the first 24 hours, patients with a past history of heart failure received 2,900mLof IV fluids [1,688 – 4,714mL] versus 3,977mL [2,500 – 6,200mL] received by those without a history of heart failure, p = 0.02.
Conclusion:
Septic patients with a past history of heart failure received 1L less IV fluids in the first 24 hours with no difference in mortality.
-
Original Articles
Atelectasis and lung changes in preterm neonates in the neonatal period: a blind radiological report and clinical findings
- Anne Karoline Santos ,
- Jaqueline Silveira,
- Valéria Cabral Neves,
- Talita Gianello Gnoato Zotz,
- Arlete Ana Motter, [ … ],
- Marimar Goretti Andreazza
Abstract
Original ArticlesAtelectasis and lung changes in preterm neonates in the neonatal period: a blind radiological report and clinical findings
Rev Bras Ter Intensiva. 2019;31(3):347-353
DOI 10.5935/0103-507X.20190047
- Anne Karoline Santos ,
- Jaqueline Silveira,
- Valéria Cabral Neves,
- Talita Gianello Gnoato Zotz,
- Arlete Ana Motter,
- Marimar Goretti Andreazza
Views0ABSTRACT
Objective:
To determine the occurrence and characteristics of atelectasis, opacities, hypolucency and pulmonary infiltrates observed on chest X-rays of preterm infants in a neonatal intensive care unit.
Methods:
This was a cross-sectional observational study. From August to December 2017, all chest radiographs of newborn infants were analyzed. The study included the chest radiographs of preterm neonates with gestational ages up to 36 weeks in the neonatal period that showed clear changes or suspected changes, which were confirmed after a radiologist’s report. Radiological changes were associated with possible predisposing factors.
Results:
During the study period, 450 radiographs were performed on preterm neonates, and 37 lung changes were identified and classified into 4 types: 12 (2.66%) changes were described as opacities, 11 (2.44%) were described as atelectasis, 10 (2.22%) were described as pulmonary infiltrate, and 4 (0.88%) were described as hypolucency. A higher occurrence of atelectasis was noted in the right lung (81.8%). Among the abnormal radiographs, 25 (67.6%) newborn infants were receiving invasive mechanical ventilation.
Conclusion:
Considering the radiological report, no significance was found for the observed changes. Atelectasis was not the most frequently observed change. The predisposing factors for these changes were extreme prematurity, low weight, male sex, a poorly positioned endotracheal tube and the use of invasive mechanical ventilation.
Keywords:Diagnostic imagingInfant, prematureIntensive care units, neonatalPremature birthPulmonary atelectasisThorax/diagnostic imagingSee moreViews0Abstract
Original ArticlesAtelectasis and lung changes in preterm neonates in the neonatal period: a blind radiological report and clinical findings
Rev Bras Ter Intensiva. 2019;31(3):347-353
DOI 10.5935/0103-507X.20190047
- Anne Karoline Santos ,
- Jaqueline Silveira,
- Valéria Cabral Neves,
- Talita Gianello Gnoato Zotz,
- Arlete Ana Motter,
- Marimar Goretti Andreazza
Views0ABSTRACT
Objective:
To determine the occurrence and characteristics of atelectasis, opacities, hypolucency and pulmonary infiltrates observed on chest X-rays of preterm infants in a neonatal intensive care unit.
Methods:
This was a cross-sectional observational study. From August to December 2017, all chest radiographs of newborn infants were analyzed. The study included the chest radiographs of preterm neonates with gestational ages up to 36 weeks in the neonatal period that showed clear changes or suspected changes, which were confirmed after a radiologist’s report. Radiological changes were associated with possible predisposing factors.
Results:
During the study period, 450 radiographs were performed on preterm neonates, and 37 lung changes were identified and classified into 4 types: 12 (2.66%) changes were described as opacities, 11 (2.44%) were described as atelectasis, 10 (2.22%) were described as pulmonary infiltrate, and 4 (0.88%) were described as hypolucency. A higher occurrence of atelectasis was noted in the right lung (81.8%). Among the abnormal radiographs, 25 (67.6%) newborn infants were receiving invasive mechanical ventilation.
Conclusion:
Considering the radiological report, no significance was found for the observed changes. Atelectasis was not the most frequently observed change. The predisposing factors for these changes were extreme prematurity, low weight, male sex, a poorly positioned endotracheal tube and the use of invasive mechanical ventilation.
Keywords:Diagnostic imagingInfant, prematureIntensive care units, neonatalPremature birthPulmonary atelectasisThorax/diagnostic imagingSee more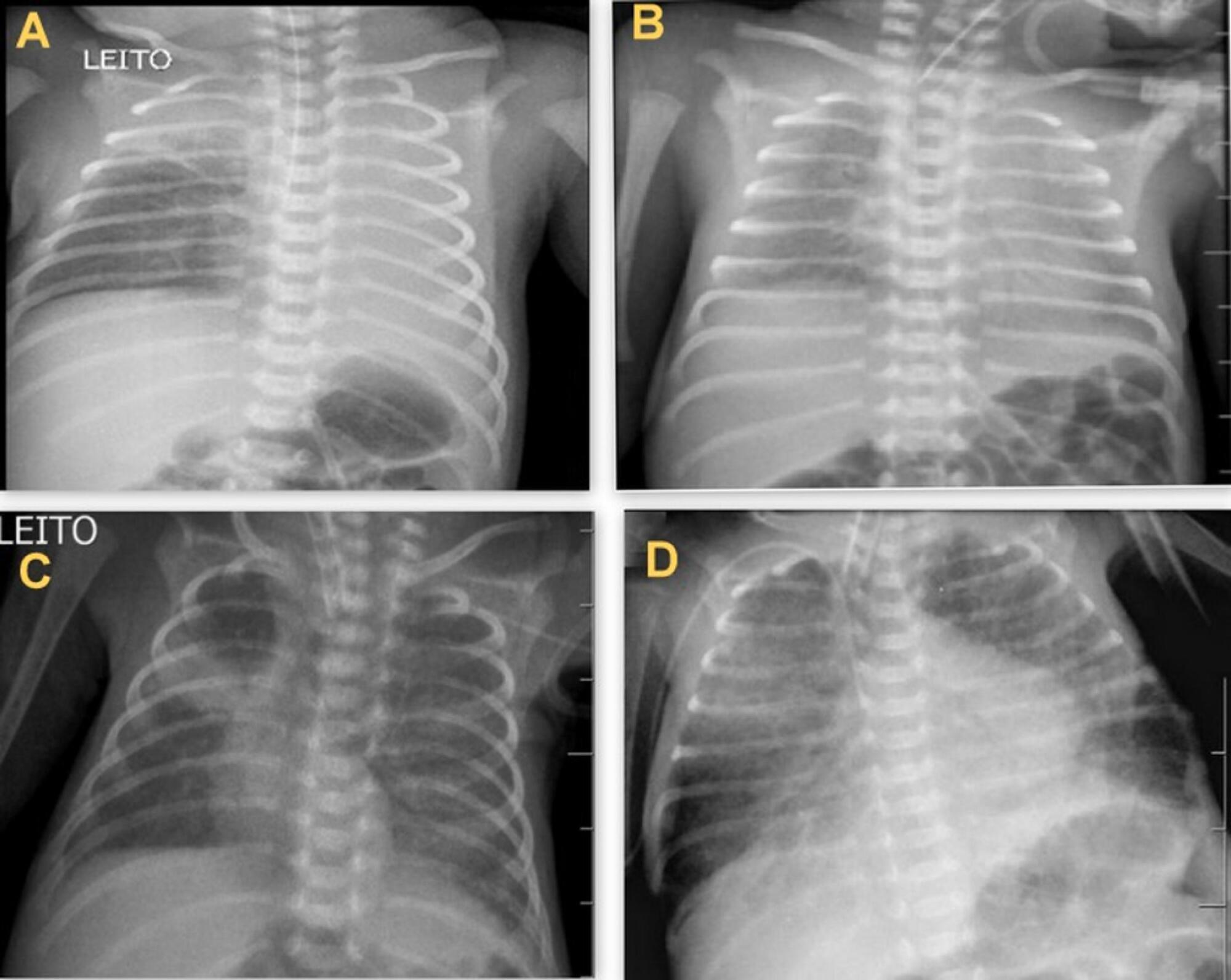
- Anne Karoline Santos
-
Original Articles
Evaluation of pulmonary B lines by different intensive care physicians using bedside ultrasonography: a reliability study
- Juliana Rodrigues Vieira ,
- Marcela Rangel de Castro,
- Thaís de Paula Guimarães,
- Aldo José Tavarez Pinheiro,
- Ana Clara Tiso Costa Figueiredo, [ … ],
- Wesley Academes Oliveira
Abstract
Original ArticlesEvaluation of pulmonary B lines by different intensive care physicians using bedside ultrasonography: a reliability study
Rev Bras Ter Intensiva. 2019;31(3):354-360
DOI 10.5935/0103-507X.20190058
- Juliana Rodrigues Vieira ,
- Marcela Rangel de Castro,
- Thaís de Paula Guimarães,
- Aldo José Tavarez Pinheiro,
- Ana Clara Tiso Costa Figueiredo,
- Bruna Jacomini Martins,
- Daniel Reis do Carmo,
- Wesley Academes Oliveira
Views0ABSTRACT
Objective:
To evaluate the agreement between intensive care physicians with similar training in the use of bedside lung ultrasonography in identifying pulmonary B lines, visualized in real time, to verify the reproducibility of the method.
Methods:
A total of 67 patients with some ventilatory deterioration identified within 12 hours after a pulmonary ultrasonography in the period from November 2016 to March 2017 were analyzed, and all were admitted to an intensive care unit of a private hospital in Belo Horizonte, Minas Gerais. The lung ultrasonographies were performed by three different professionals, termed A, B and C, and the time interval between each lung ultrasonography was less than 3 hours. The only visualized chest zones were the anterior and lateral, defined as right and left anterior (1) zones (Z1R and Z1L, respectively), which were delimited by the clavicle, the sternum and the horizontal line perpendicular to the xiphoid process and anterior axillary line. The right and left lateral (2) zones (Z2R and Z2L, respectively) covered the lateral area between the anterior and posterior axillary lines, with the lower limit being the same horizontal line corresponding to the height of the xiphoid process. A lung zone was considered positive for B lines upon visualization of three or more of these lines, suggesting the presence of alveolar-interstitial syndrome. Using the Kappa value, we evaluated the agreement among the four zones according to the execution of each pair of professionals (AB, AC and BC).
Results:
Approximately 80% of the areas that were visualized showed a moderate to substantial agreement, with the Kappa values ranging from 0.41 – 079 (p < 0.05; 95% CI). The highest levels of agreement occurred in the upper zones Z1R and Z1L between subgroups AC and BC, with a Kappa of approximately 0.65 (p < 0.001). In turn, Z2L showed one of the lowest agreements, with a Kappa of 0.36.
Conclusion:
The possible limitation of an examiner-dependent effect on lung ultrasounds was not found in this study, suggesting the good reproducibility of this diagnostic modality at the bedside.
Keywords:Critical careLung/diagnostic imagingReproducibility of resultsRespiratory insuficience/diagnostic imagingUltrasonographySee moreViews0Abstract
Original ArticlesEvaluation of pulmonary B lines by different intensive care physicians using bedside ultrasonography: a reliability study
Rev Bras Ter Intensiva. 2019;31(3):354-360
DOI 10.5935/0103-507X.20190058
- Juliana Rodrigues Vieira ,
- Marcela Rangel de Castro,
- Thaís de Paula Guimarães,
- Aldo José Tavarez Pinheiro,
- Ana Clara Tiso Costa Figueiredo,
- Bruna Jacomini Martins,
- Daniel Reis do Carmo,
- Wesley Academes Oliveira
Views0ABSTRACT
Objective:
To evaluate the agreement between intensive care physicians with similar training in the use of bedside lung ultrasonography in identifying pulmonary B lines, visualized in real time, to verify the reproducibility of the method.
Methods:
A total of 67 patients with some ventilatory deterioration identified within 12 hours after a pulmonary ultrasonography in the period from November 2016 to March 2017 were analyzed, and all were admitted to an intensive care unit of a private hospital in Belo Horizonte, Minas Gerais. The lung ultrasonographies were performed by three different professionals, termed A, B and C, and the time interval between each lung ultrasonography was less than 3 hours. The only visualized chest zones were the anterior and lateral, defined as right and left anterior (1) zones (Z1R and Z1L, respectively), which were delimited by the clavicle, the sternum and the horizontal line perpendicular to the xiphoid process and anterior axillary line. The right and left lateral (2) zones (Z2R and Z2L, respectively) covered the lateral area between the anterior and posterior axillary lines, with the lower limit being the same horizontal line corresponding to the height of the xiphoid process. A lung zone was considered positive for B lines upon visualization of three or more of these lines, suggesting the presence of alveolar-interstitial syndrome. Using the Kappa value, we evaluated the agreement among the four zones according to the execution of each pair of professionals (AB, AC and BC).
Results:
Approximately 80% of the areas that were visualized showed a moderate to substantial agreement, with the Kappa values ranging from 0.41 – 079 (p < 0.05; 95% CI). The highest levels of agreement occurred in the upper zones Z1R and Z1L between subgroups AC and BC, with a Kappa of approximately 0.65 (p < 0.001). In turn, Z2L showed one of the lowest agreements, with a Kappa of 0.36.
Conclusion:
The possible limitation of an examiner-dependent effect on lung ultrasounds was not found in this study, suggesting the good reproducibility of this diagnostic modality at the bedside.
Keywords:Critical careLung/diagnostic imagingReproducibility of resultsRespiratory insuficience/diagnostic imagingUltrasonographySee more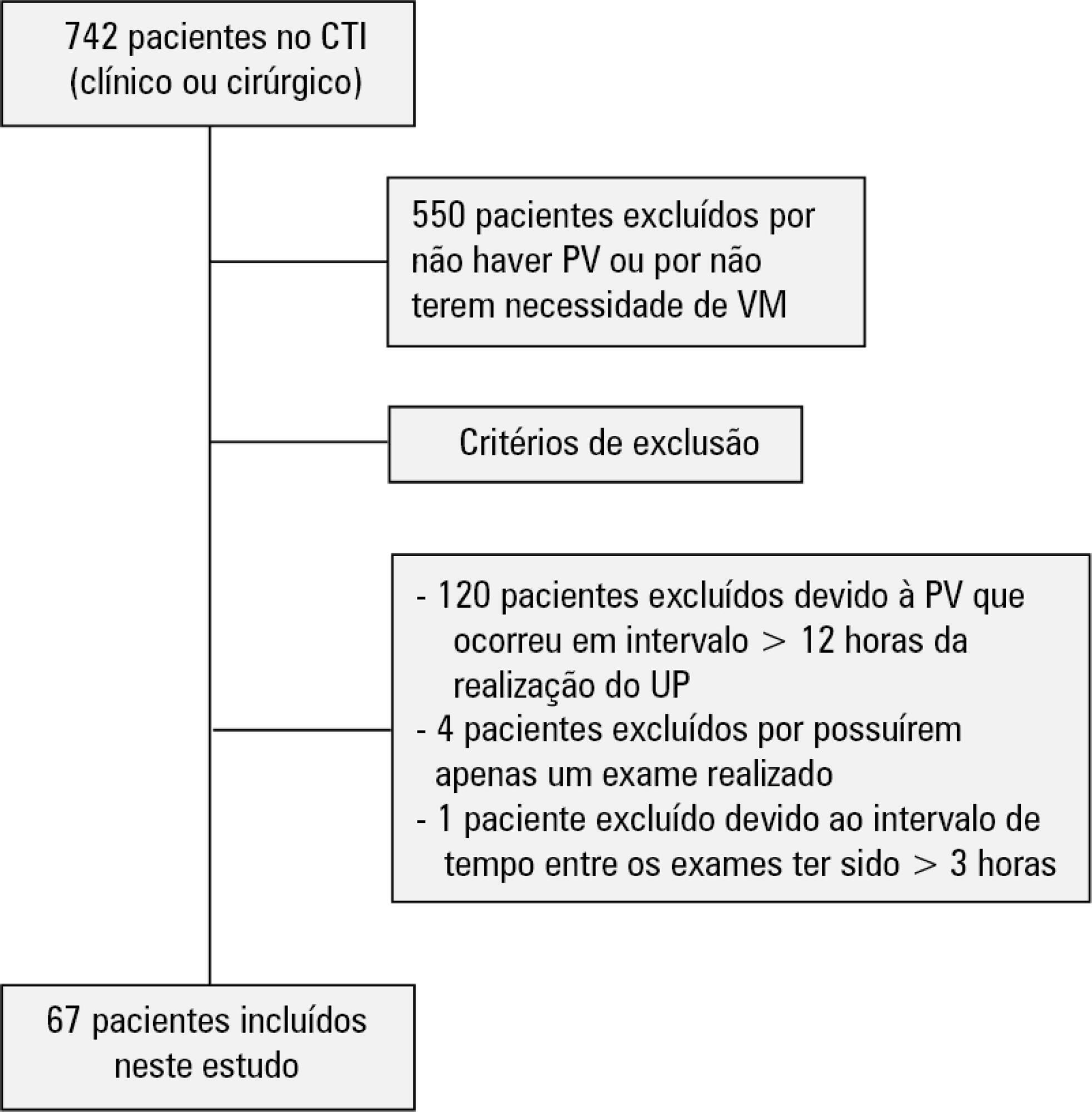
- Juliana Rodrigues Vieira
-
Original Articles
Impact of fast-track management on adult cardiac surgery: clinical and hospital outcomes
- Cibelle Andrade Lima ,
- Maria Karoline Richtrmoc,
- Wagner Souza Leite,
- Diogo André Rodrigues Galdino Silva,
- Wildberg Alencar Lima, [ … ],
- Armele Dornelas de Andrade
Abstract
Original ArticlesImpact of fast-track management on adult cardiac surgery: clinical and hospital outcomes
Rev Bras Ter Intensiva. 2019;31(3):361-367
DOI 10.5935/0103-507X.20190059
- Cibelle Andrade Lima ,
- Maria Karoline Richtrmoc,
- Wagner Souza Leite,
- Diogo André Rodrigues Galdino Silva,
- Wildberg Alencar Lima,
- Shirley Lima Campos,
- Armele Dornelas de Andrade
Views0ABSTRACT
Objective:
To compare the impact of two fast-track strategies regarding the extubation time and removal of invasive mechanical ventilation in adults after cardiac surgery on clinical and hospital outcomes.
Methods:
This was a retrospective cohort study with patients undergoing cardiac surgery. Patients were classified according to the extubation time as the Control Group (extubated 6 hours after admission to the intensive care unit, with a maximum mechanical ventilation time of 18 hours), Group 1 (extubated in the operating room after surgery) and Group 2 (extubated within 6 hours after admission to the intensive care unit). The primary outcomes analyzed were vital capacity on the first postoperative day, length of hospital stay, and length of stay in the intensive care unit. The secondary outcomes were reintubation, hospital-acquired pneumonia, sepsis, and death.
Results:
For the 223 patients evaluated, the vital capacity was lower in Groups 1 and 2 compared to the Control (p = 0.000 and p = 0.046, respectively). The length of stay in the intensive care unit was significantly lower in Groups 1 and 2 compared to the Control (p = 0.009 and p = 0.000, respectively), whereas the length of hospital stay was lower in Group 1 compared to the Control (p = 0.014). There was an association between extubation in the operating room (Group 1) with reintubation (p = 0.025) and postoperative complications (p = 0.038).
Conclusion:
Patients undergoing fast-track management with extubation within 6 hours had shorter stays in the intensive care unit without increasing postoperative complications and death. Patients extubated in the operating room had a shorter hospital stay and a shorter stay in the intensive care unit but showed an increase in the frequency of reintubation and postoperative complications.
Keywords:Airway extubationCardiac surgical proceduresIntensive care unitsLength of stayRespiration, artificialVital capacitySee moreViews0Abstract
Original ArticlesImpact of fast-track management on adult cardiac surgery: clinical and hospital outcomes
Rev Bras Ter Intensiva. 2019;31(3):361-367
DOI 10.5935/0103-507X.20190059
- Cibelle Andrade Lima ,
- Maria Karoline Richtrmoc,
- Wagner Souza Leite,
- Diogo André Rodrigues Galdino Silva,
- Wildberg Alencar Lima,
- Shirley Lima Campos,
- Armele Dornelas de Andrade
Views0ABSTRACT
Objective:
To compare the impact of two fast-track strategies regarding the extubation time and removal of invasive mechanical ventilation in adults after cardiac surgery on clinical and hospital outcomes.
Methods:
This was a retrospective cohort study with patients undergoing cardiac surgery. Patients were classified according to the extubation time as the Control Group (extubated 6 hours after admission to the intensive care unit, with a maximum mechanical ventilation time of 18 hours), Group 1 (extubated in the operating room after surgery) and Group 2 (extubated within 6 hours after admission to the intensive care unit). The primary outcomes analyzed were vital capacity on the first postoperative day, length of hospital stay, and length of stay in the intensive care unit. The secondary outcomes were reintubation, hospital-acquired pneumonia, sepsis, and death.
Results:
For the 223 patients evaluated, the vital capacity was lower in Groups 1 and 2 compared to the Control (p = 0.000 and p = 0.046, respectively). The length of stay in the intensive care unit was significantly lower in Groups 1 and 2 compared to the Control (p = 0.009 and p = 0.000, respectively), whereas the length of hospital stay was lower in Group 1 compared to the Control (p = 0.014). There was an association between extubation in the operating room (Group 1) with reintubation (p = 0.025) and postoperative complications (p = 0.038).
Conclusion:
Patients undergoing fast-track management with extubation within 6 hours had shorter stays in the intensive care unit without increasing postoperative complications and death. Patients extubated in the operating room had a shorter hospital stay and a shorter stay in the intensive care unit but showed an increase in the frequency of reintubation and postoperative complications.
Keywords:Airway extubationCardiac surgical proceduresIntensive care unitsLength of stayRespiration, artificialVital capacitySee more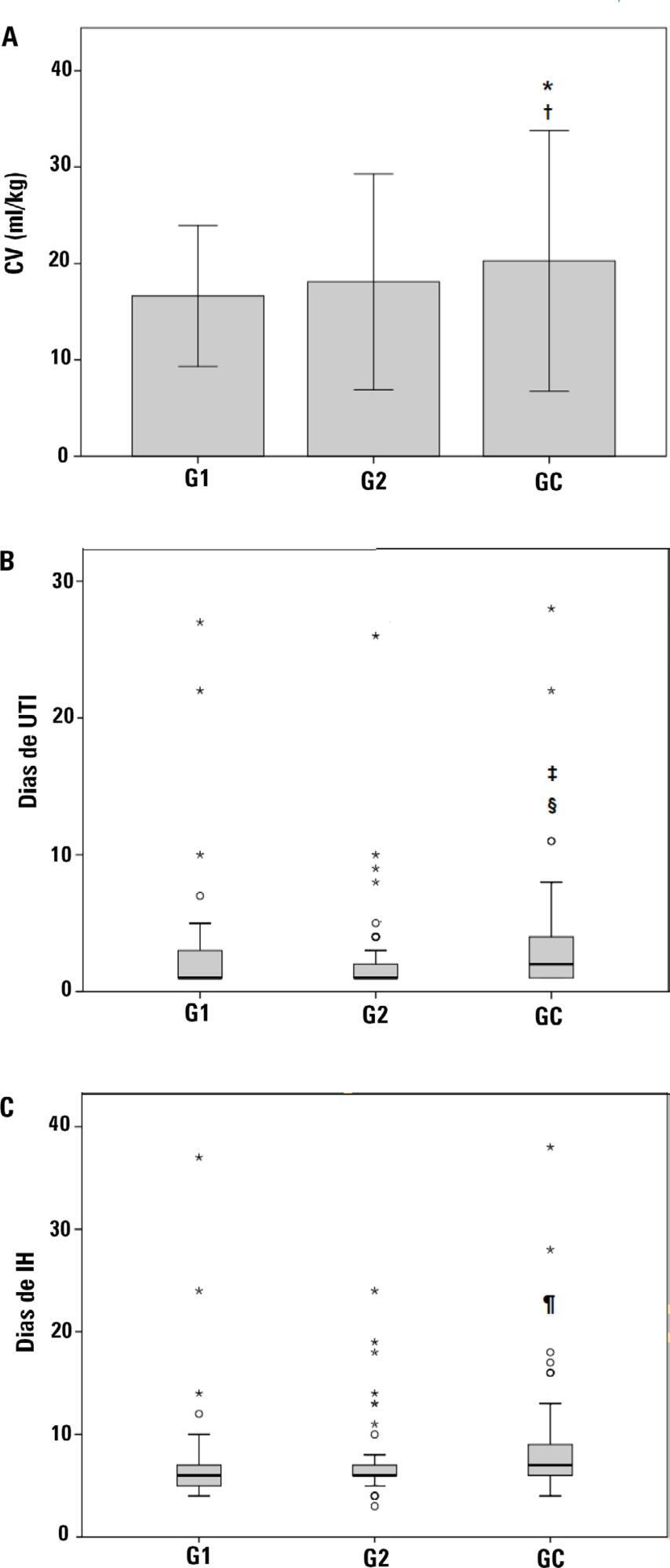
- Cibelle Andrade Lima
-
Review Articles
The role of natriuretic peptides in the management, outcomes and prognosis of sepsis and septic shock
Rev Bras Ter Intensiva. 2019;31(3):368-378
Abstract
Review ArticlesThe role of natriuretic peptides in the management, outcomes and prognosis of sepsis and septic shock
Rev Bras Ter Intensiva. 2019;31(3):368-378
DOI 10.5935/0103-507X.20190060
Views0See moreABSTRACT
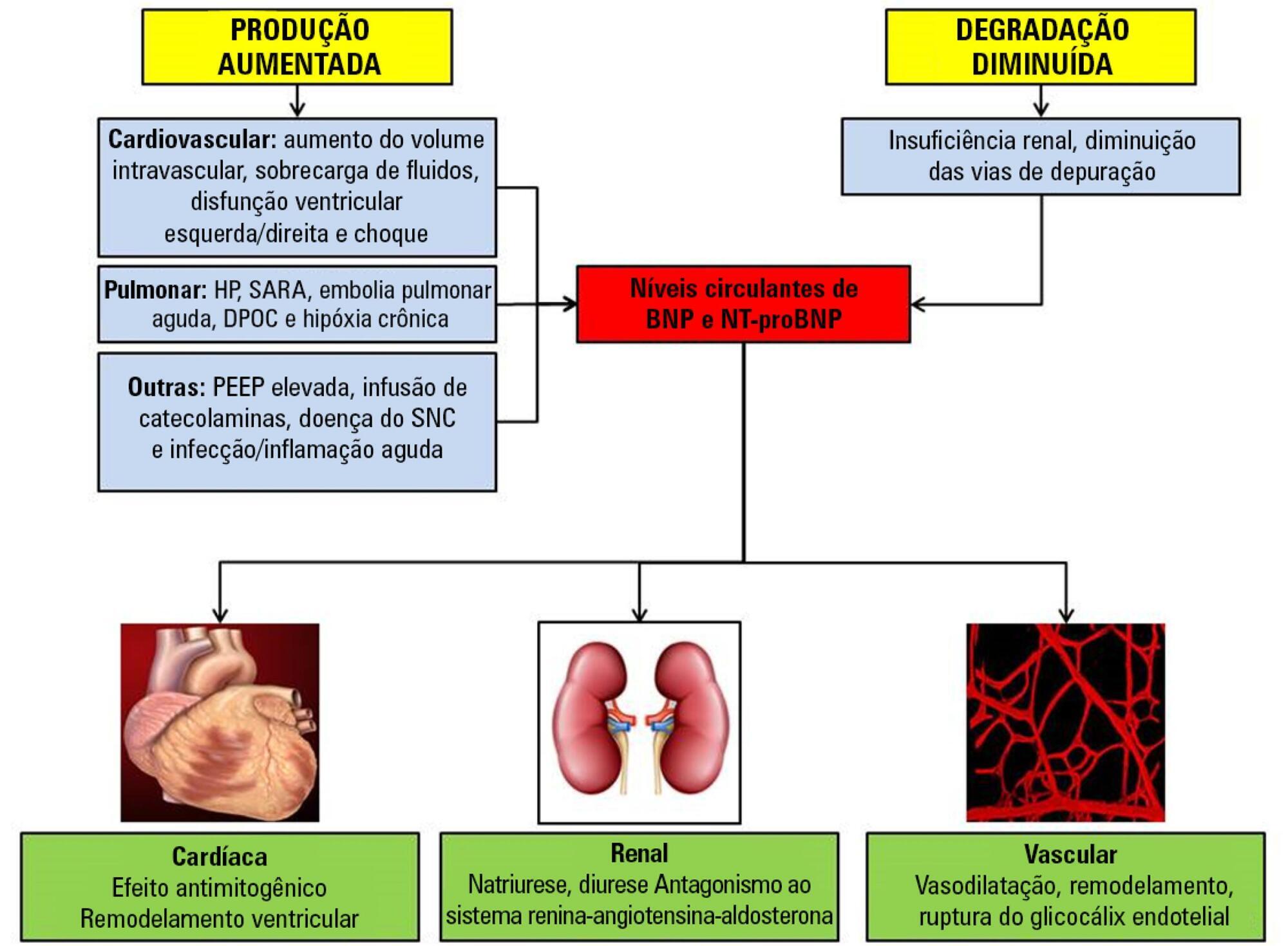
Sepsis continues to be a leading public health burden in the United States and worldwide. With the increasing use of advanced laboratory technology, there is a renewed interest in the use of biomarkers in sepsis to aid in more precise and targeted decision-making. Natriuretic peptides have been increasingly recognized to play a role outside of heart failure. They are commonly elevated among critically ill patients in the setting of cardiopulmonary dysfunction and may play a role in identifying patients with sepsis and septic shock. There are limited data on the role of these biomarkers in the diagnosis, management, outcomes and prognosis of septic patients. This review seeks to describe the role of natriuretic peptides in fluid resuscitation, diagnosis of ventricular dysfunction and outcomes and the prognosis of patients with sepsis. B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP) have been noted to be associated with left ventricular systolic and diastolic and right ventricular dysfunction in patients with septic cardiomyopathy. BNP/NT-proBNP may predict fluid responsiveness, and trends of these peptides may play a role in fluid resuscitation. Despite suggestions of a correlation with mortality, the role of BNP in mortality outcomes and prognosis during sepsis needs further evaluation.
Views0Abstract
Review ArticlesThe role of natriuretic peptides in the management, outcomes and prognosis of sepsis and septic shock
Rev Bras Ter Intensiva. 2019;31(3):368-378
DOI 10.5935/0103-507X.20190060
Views0See moreABSTRACT
Sepsis continues to be a leading public health burden in the United States and worldwide. With the increasing use of advanced laboratory technology, there is a renewed interest in the use of biomarkers in sepsis to aid in more precise and targeted decision-making. Natriuretic peptides have been increasingly recognized to play a role outside of heart failure. They are commonly elevated among critically ill patients in the setting of cardiopulmonary dysfunction and may play a role in identifying patients with sepsis and septic shock. There are limited data on the role of these biomarkers in the diagnosis, management, outcomes and prognosis of septic patients. This review seeks to describe the role of natriuretic peptides in fluid resuscitation, diagnosis of ventricular dysfunction and outcomes and the prognosis of patients with sepsis. B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP) have been noted to be associated with left ventricular systolic and diastolic and right ventricular dysfunction in patients with septic cardiomyopathy. BNP/NT-proBNP may predict fluid responsiveness, and trends of these peptides may play a role in fluid resuscitation. Despite suggestions of a correlation with mortality, the role of BNP in mortality outcomes and prognosis during sepsis needs further evaluation.
-
Review Articles
NUTRIC score use around the world: a systematic review
Rev Bras Ter Intensiva. 2019;31(3):379-385
Abstract
Review ArticlesNUTRIC score use around the world: a systematic review
Rev Bras Ter Intensiva. 2019;31(3):379-385
DOI 10.5935/0103-507X.20190061
Views0See moreABSTRACT
Objective:
To collect data on the use of The Nutrition Risk in Critically Ill (NUTRIC) score.
Methods:
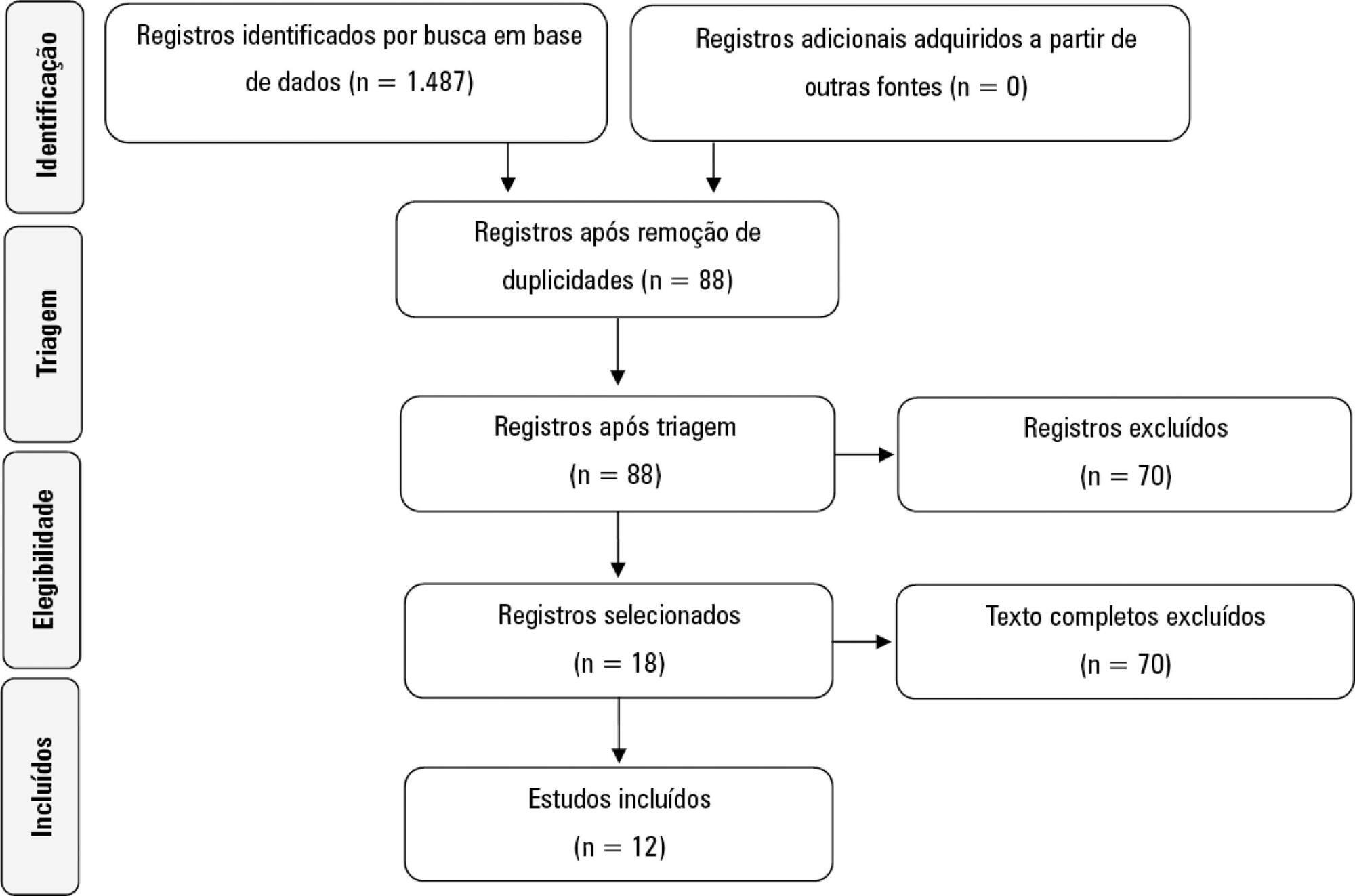
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Reviews, abstracts, dissertations, protocols and case reports were excluded from this review; to be included in the review, studies needed to specifically evaluate the NUTRIC score and to have been published in English, Spanish or Portuguese.
Results:
We included 12 (0.8%) studies from our search in this review. Ten studies (83.3%) were observational, 1 was a pilot study (8.3%) and 1 was a randomized control trial (8.3%). All of the included studies (100%) chose not to use IL-6 and considered a high nutritional risk cutoff point ≥ 5. There were 11 (91.7%) English language studies versus 1 (8.3%) Spanish language study. Mechanical ventilation and a high NUTRIC score were significantly correlated in four studies. The association between intensive care unit or hospital length of stay and nutritional high risk was significant in three studies. Seven studies found a statistically significant association between the NUTRIC score and mortality.
Conclusion:
The NUTRIC score is related to clinical outcomes, such as length of hospital stay, and is appropriate for use in critically ill patients in intensive care units.
Views0Abstract
Review ArticlesNUTRIC score use around the world: a systematic review
Rev Bras Ter Intensiva. 2019;31(3):379-385
DOI 10.5935/0103-507X.20190061
Views0See moreABSTRACT
Objective:
To collect data on the use of The Nutrition Risk in Critically Ill (NUTRIC) score.
Methods:
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Reviews, abstracts, dissertations, protocols and case reports were excluded from this review; to be included in the review, studies needed to specifically evaluate the NUTRIC score and to have been published in English, Spanish or Portuguese.
Results:
We included 12 (0.8%) studies from our search in this review. Ten studies (83.3%) were observational, 1 was a pilot study (8.3%) and 1 was a randomized control trial (8.3%). All of the included studies (100%) chose not to use IL-6 and considered a high nutritional risk cutoff point ≥ 5. There were 11 (91.7%) English language studies versus 1 (8.3%) Spanish language study. Mechanical ventilation and a high NUTRIC score were significantly correlated in four studies. The association between intensive care unit or hospital length of stay and nutritional high risk was significant in three studies. Seven studies found a statistically significant association between the NUTRIC score and mortality.
Conclusion:
The NUTRIC score is related to clinical outcomes, such as length of hospital stay, and is appropriate for use in critically ill patients in intensive care units.
-
Review Articles
How to discuss about do-not-resuscitate in the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(3):386-392
Abstract
Review ArticlesHow to discuss about do-not-resuscitate in the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
Views0See moreAbstract
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Views0Abstract
Review ArticlesHow to discuss about do-not-resuscitate in the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
Views0See moreAbstract
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
-
Review Articles
Pediatric enteral nutrition therapy for burn victims: when should it be initiated?
Rev Bras Ter Intensiva. 2019;31(3):393-402
Abstract
Review ArticlesPediatric enteral nutrition therapy for burn victims: when should it be initiated?
Rev Bras Ter Intensiva. 2019;31(3):393-402
DOI 10.5935/0103-507X.20190062
Views0See moreABSTRACT
Objective:
To review the scientific evidence regarding the initiation of enteral nutrition in the pediatric burn population.
Methods:
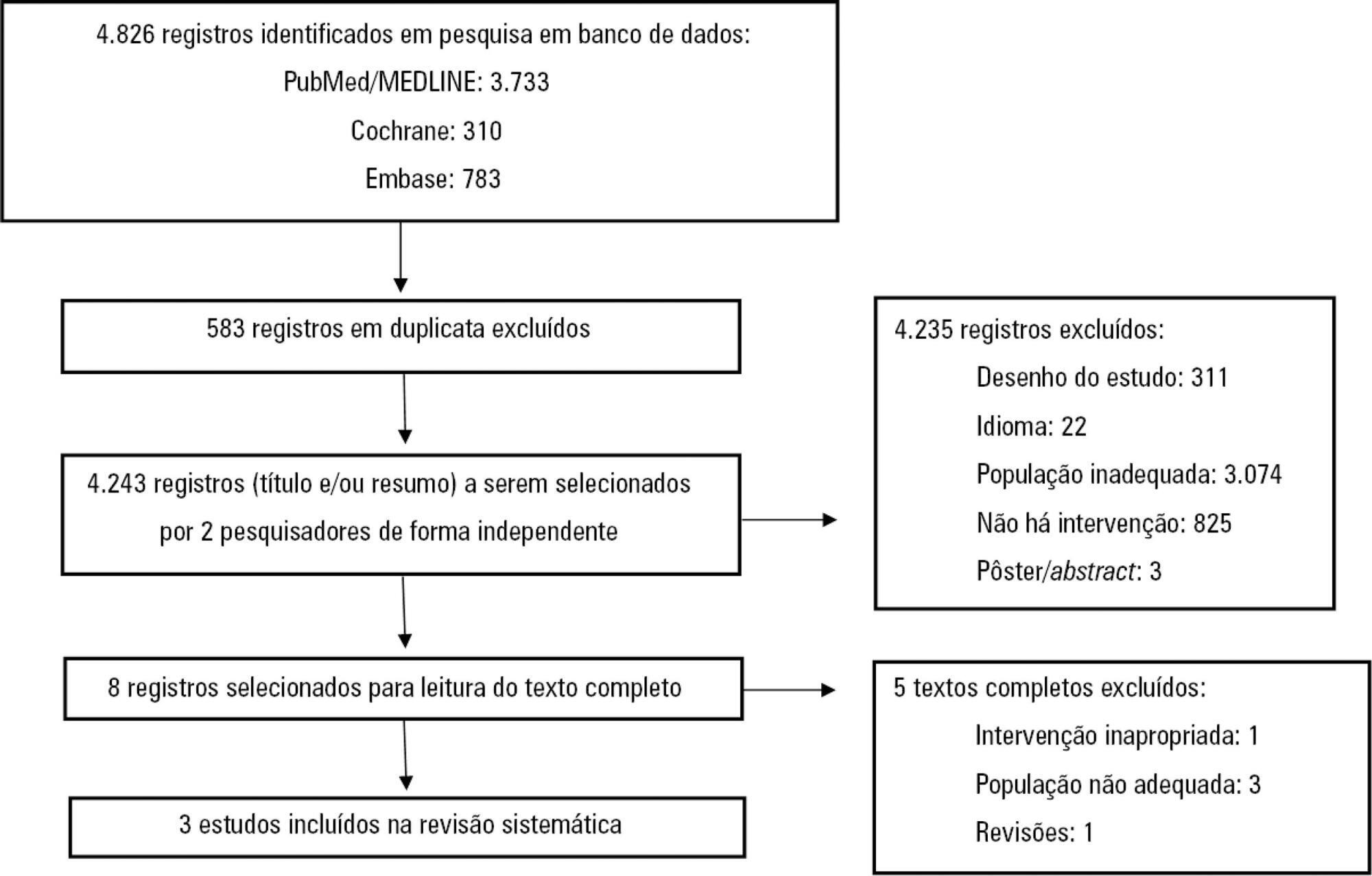
This study was a systematic review and meta-analysis of randomized clinical trials comparing early enteral nutrition and late enteral nutrition in individuals aged 1 month to 18 years with burns. The MEDLINE/PubMed, Embase and Cochrane Library databases were searched using the terms “burns”, “fires”, “child nutrition disorders”, “nutritional support” and related terms.
Results:
Three articles that included a total of 781 patients were identified. There was no significant difference in the mortality rate between the early and late groups (OR = 0.72, 95%CI = 0.46 – 1.15, p = 0.17). Patients who received early enteral nutrition had a 3.69-day reduction in the length of hospital stay (mean difference = -3.69, 95%CI = -4.11 – -3.27, p < 0.00001). There was a higher incidence of diarrhea and vomiting and decreased intestinal permeability in the early group. This group also presented higher a serum insulin concentration and insulin/glucagon ratio as well as lower caloric deficit and weight loss when compared to the control group.
Conclusion:
Analysis of the different intragroup variables suggests the importance of starting nutritional support early. Considering the number of pediatric burn patients, there is a need for robust studies with greater scientific impact.
Views0Abstract
Review ArticlesPediatric enteral nutrition therapy for burn victims: when should it be initiated?
Rev Bras Ter Intensiva. 2019;31(3):393-402
DOI 10.5935/0103-507X.20190062
Views0See moreABSTRACT
Objective:
To review the scientific evidence regarding the initiation of enteral nutrition in the pediatric burn population.
Methods:
This study was a systematic review and meta-analysis of randomized clinical trials comparing early enteral nutrition and late enteral nutrition in individuals aged 1 month to 18 years with burns. The MEDLINE/PubMed, Embase and Cochrane Library databases were searched using the terms “burns”, “fires”, “child nutrition disorders”, “nutritional support” and related terms.
Results:
Three articles that included a total of 781 patients were identified. There was no significant difference in the mortality rate between the early and late groups (OR = 0.72, 95%CI = 0.46 – 1.15, p = 0.17). Patients who received early enteral nutrition had a 3.69-day reduction in the length of hospital stay (mean difference = -3.69, 95%CI = -4.11 – -3.27, p < 0.00001). There was a higher incidence of diarrhea and vomiting and decreased intestinal permeability in the early group. This group also presented higher a serum insulin concentration and insulin/glucagon ratio as well as lower caloric deficit and weight loss when compared to the control group.
Conclusion:
Analysis of the different intragroup variables suggests the importance of starting nutritional support early. Considering the number of pediatric burn patients, there is a need for robust studies with greater scientific impact.
-
Review Articles
Diagnosis of brain death in Brazil
Rev Bras Ter Intensiva. 2019;31(3):403-409
Abstract
Review ArticlesDiagnosis of brain death in Brazil
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Views7ABSTRACT
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Keywords:Brain death/diagnosisBrazilSee moreViews7Abstract
Review ArticlesDiagnosis of brain death in Brazil
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Views7ABSTRACT
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Keywords:Brain death/diagnosisBrazilSee more -
Review Articles
Extracorporeal membrane oxygenation: a literature review
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova, [ … ],
- Thiago Domingos Corrêa
Abstract
Review ArticlesExtracorporeal membrane oxygenation: a literature review
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova,
- Bruno de Arruda Bravim,
- Ary Serpa Neto,
- Thiago Domingos Corrêa
Views1ABSTRACT
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Keywords:Critical careExtracorporeal membrane oxygenationheart failureRespiration, artificialRespiratory insufficiencySee moreViews1Abstract
Review ArticlesExtracorporeal membrane oxygenation: a literature review
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova,
- Bruno de Arruda Bravim,
- Ary Serpa Neto,
- Thiago Domingos Corrêa
Views1ABSTRACT
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Keywords:Critical careExtracorporeal membrane oxygenationheart failureRespiration, artificialRespiratory insufficiencySee more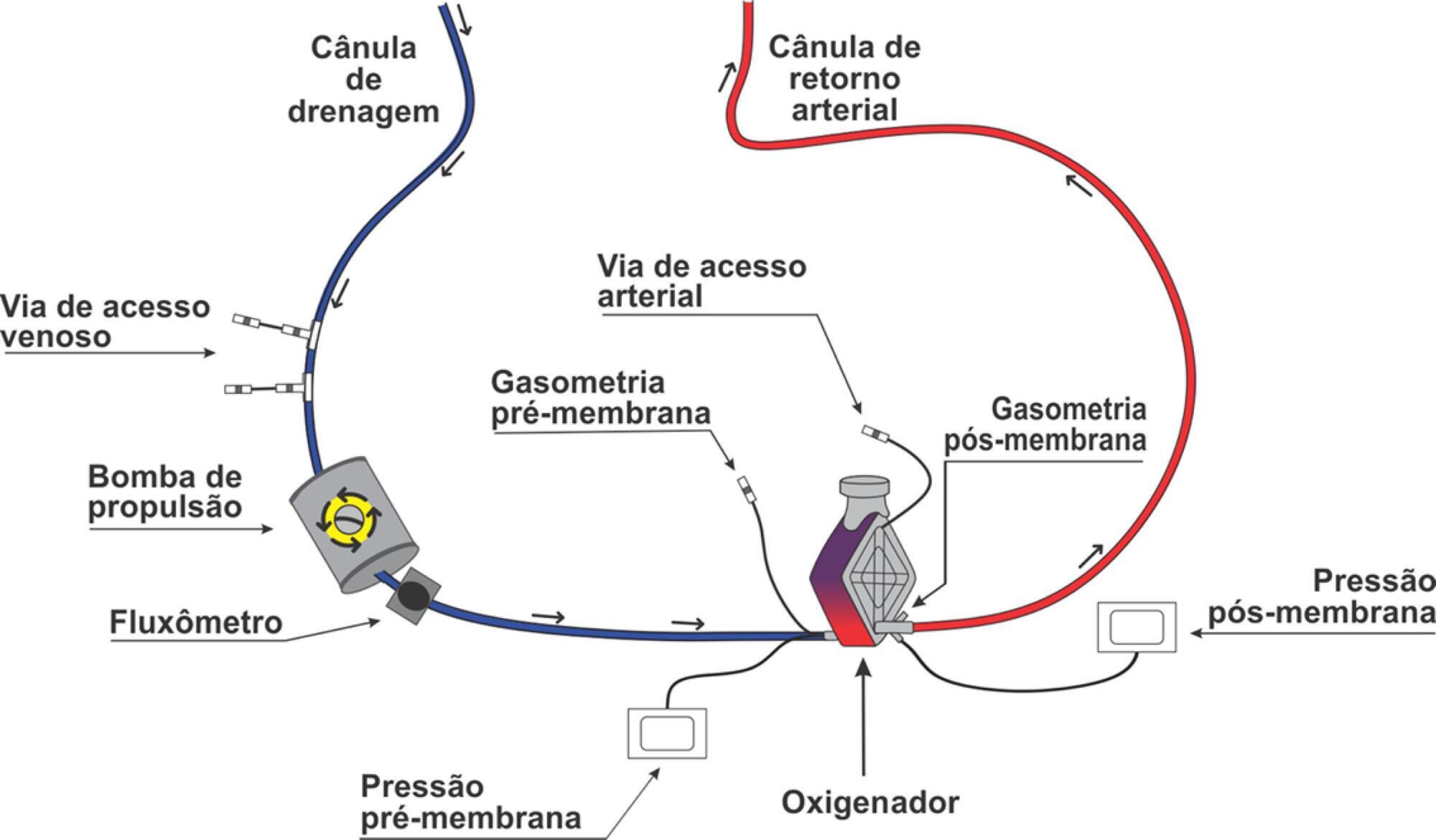
- Renato Carneiro de Freitas Chaves
-
Letters to the Editor
Mortality, morbidity, and quality-of-life outcomes of patients requiring ≥ 14 days of mechanical ventilation: a 12-month post-intensive-care-unit cohort study
- Cláudia da Rocha Cabral ,
- Cassiano Teixeira,
- Régis Goulart Rosa,
- Caroline Robinson,
- Daniel Sganzerla, [ … ],
- Vania Dezoti Micheletti
Abstract
Letters to the EditorMortality, morbidity, and quality-of-life outcomes of patients requiring ≥ 14 days of mechanical ventilation: a 12-month post-intensive-care-unit cohort study
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
- Cláudia da Rocha Cabral ,
- Cassiano Teixeira,
- Régis Goulart Rosa,
- Caroline Robinson,
- Daniel Sganzerla,
- Sérgio Henrique Loss,
- Priscila Lora,
- Vania Dezoti Micheletti
Views0Dear Editor, Intensive care unit (ICU) survivors suffer significant morbidity,(,) and longer mechanical ventilation (MV)-dependency increases the probability that these subjects will suffer a “persistent inflammation-immunosuppression and catabolism syndrome”.(–) These patients have ongoing inflammation, manageable organ failure, ongoing protein catabolism, and poor nutrition, leading to cachexia; poor wound healing and immunosuppression with increased susceptibility to […]See moreViews0Abstract
Letters to the EditorMortality, morbidity, and quality-of-life outcomes of patients requiring ≥ 14 days of mechanical ventilation: a 12-month post-intensive-care-unit cohort study
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
- Cláudia da Rocha Cabral ,
- Cassiano Teixeira,
- Régis Goulart Rosa,
- Caroline Robinson,
- Daniel Sganzerla,
- Sérgio Henrique Loss,
- Priscila Lora,
- Vania Dezoti Micheletti
Views0Dear Editor, Intensive care unit (ICU) survivors suffer significant morbidity,(,) and longer mechanical ventilation (MV)-dependency increases the probability that these subjects will suffer a “persistent inflammation-immunosuppression and catabolism syndrome”.(–) These patients have ongoing inflammation, manageable organ failure, ongoing protein catabolism, and poor nutrition, leading to cachexia; poor wound healing and immunosuppression with increased susceptibility to […]See more - Cláudia da Rocha Cabral
-
Letters to the Editor
Mandibular fracture due to rare manifestation of Langerhans cell histiocytosis
- Fábio Vieira de Miranda,
- William Phillip Pereira da Silva ,
- Renato Victor de Oliveira,
- Gustavo Antônio Correia Momesso,
- Tárik Ocon Braga Polo, [ … ],
- Leonardo Pérez Faverani
Abstract
Letters to the EditorMandibular fracture due to rare manifestation of Langerhans cell histiocytosis
Rev Bras Ter Intensiva. 2019;31(3):428-429
DOI 10.5935/0103-507X.20190048
- Fábio Vieira de Miranda,
- William Phillip Pereira da Silva ,
- Renato Victor de Oliveira,
- Gustavo Antônio Correia Momesso,
- Tárik Ocon Braga Polo,
- Leonardo Pérez Faverani
Views0Dear Editor, Langerhans cell histiocytosis (LCH) is reported as being rare in the literature, with an incidence of 5 cases per 1 million per year and a prevalence of 3.7:1 in men:women. LCH is generally limited to an organ, most commonly lesions of the bone, whether solitary or multiple, that tend to appear in the […]See moreViews0Abstract
Letters to the EditorMandibular fracture due to rare manifestation of Langerhans cell histiocytosis
Rev Bras Ter Intensiva. 2019;31(3):428-429
DOI 10.5935/0103-507X.20190048
- Fábio Vieira de Miranda,
- William Phillip Pereira da Silva ,
- Renato Victor de Oliveira,
- Gustavo Antônio Correia Momesso,
- Tárik Ocon Braga Polo,
- Leonardo Pérez Faverani
Views0Dear Editor, Langerhans cell histiocytosis (LCH) is reported as being rare in the literature, with an incidence of 5 cases per 1 million per year and a prevalence of 3.7:1 in men:women. LCH is generally limited to an organ, most commonly lesions of the bone, whether solitary or multiple, that tend to appear in the […]See more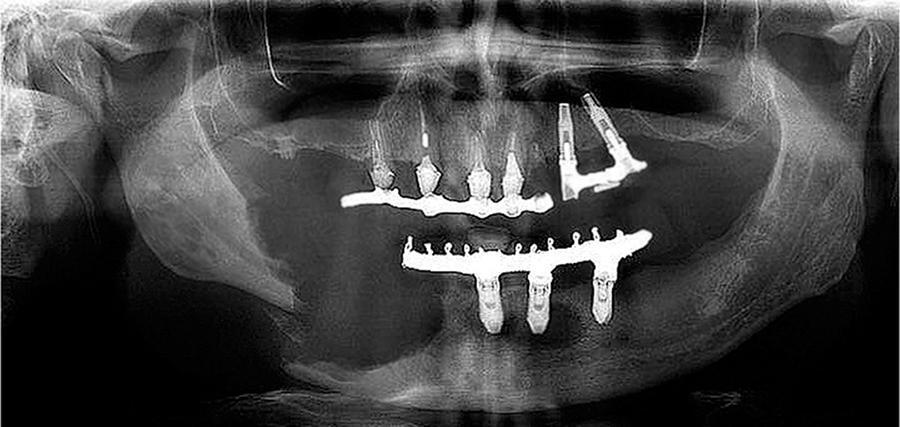
Volume Articles - Critical Care Science (CCS)
