Ultrasonography Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
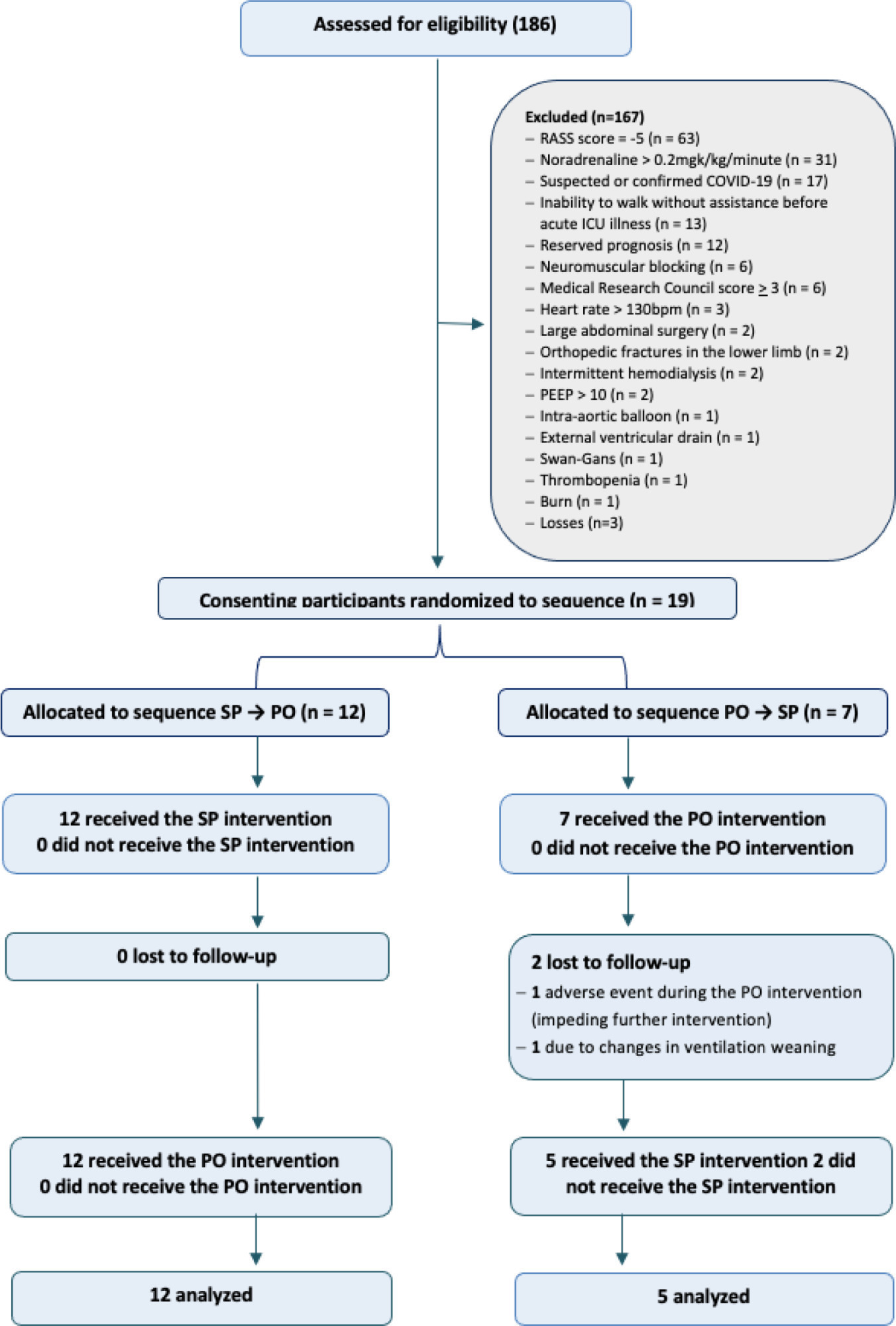
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-pt
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
Abstract
Crit Care Sci. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-pt
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
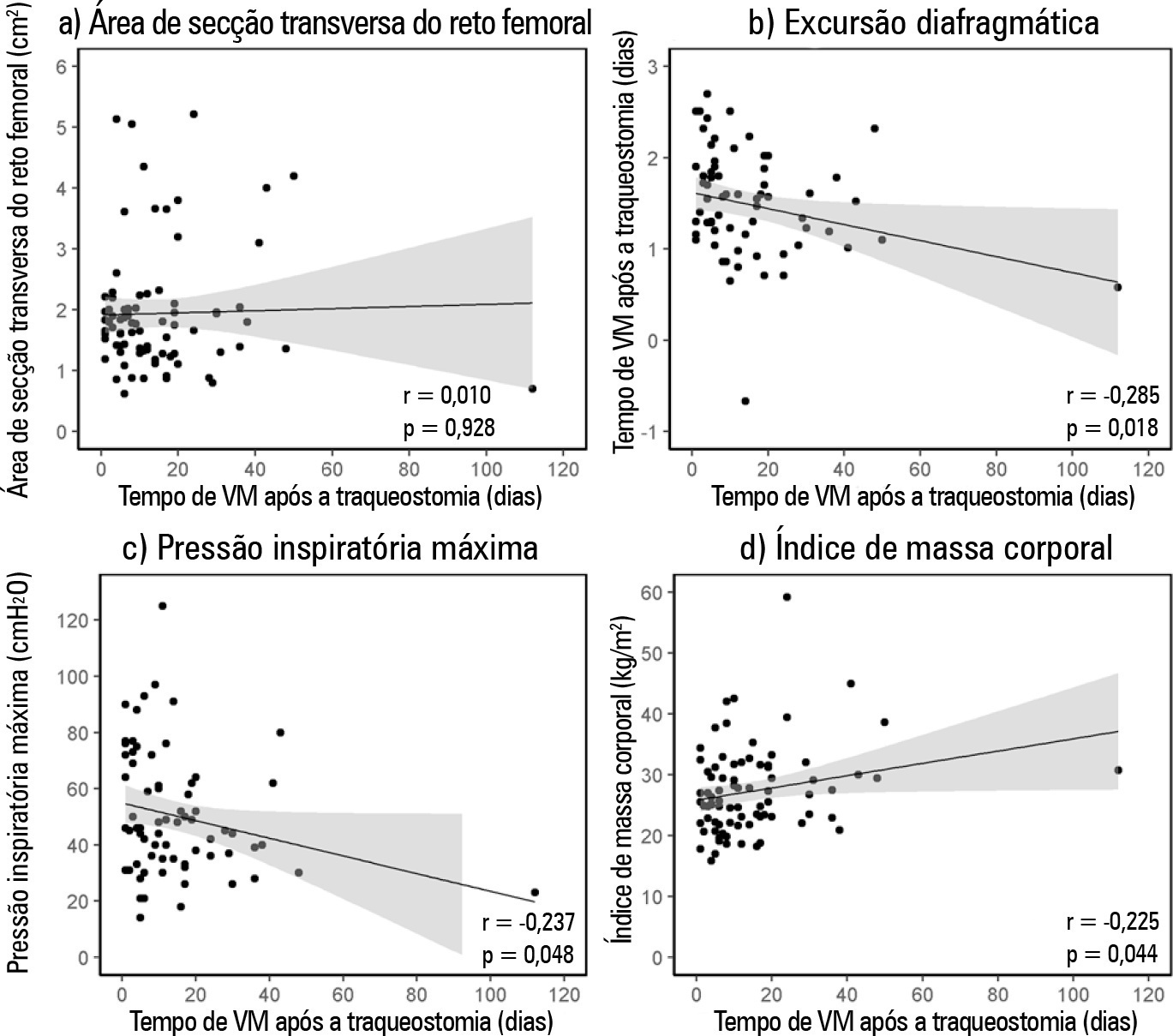
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 - 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 - 1.08; p = 0.061).
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 - 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 - 1.08; p = 0.061).
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor's level of expertise.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor's level of expertise.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):354-360
DOI 10.5935/0103-507X.20190058
To evaluate the agreement between intensive care physicians with similar training in the use of bedside lung ultrasonography in identifying pulmonary B lines, visualized in real time, to verify the reproducibility of the method.
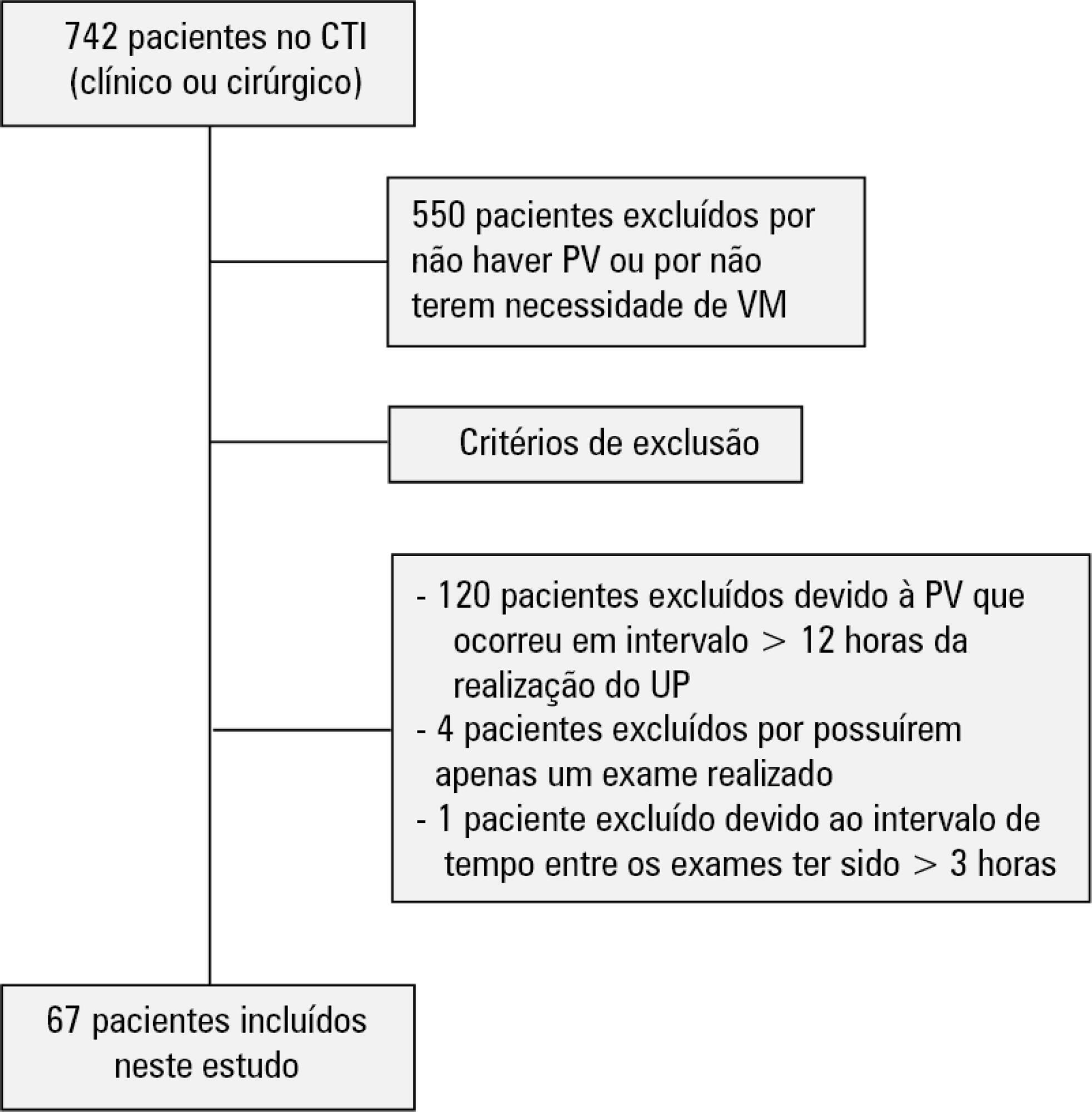
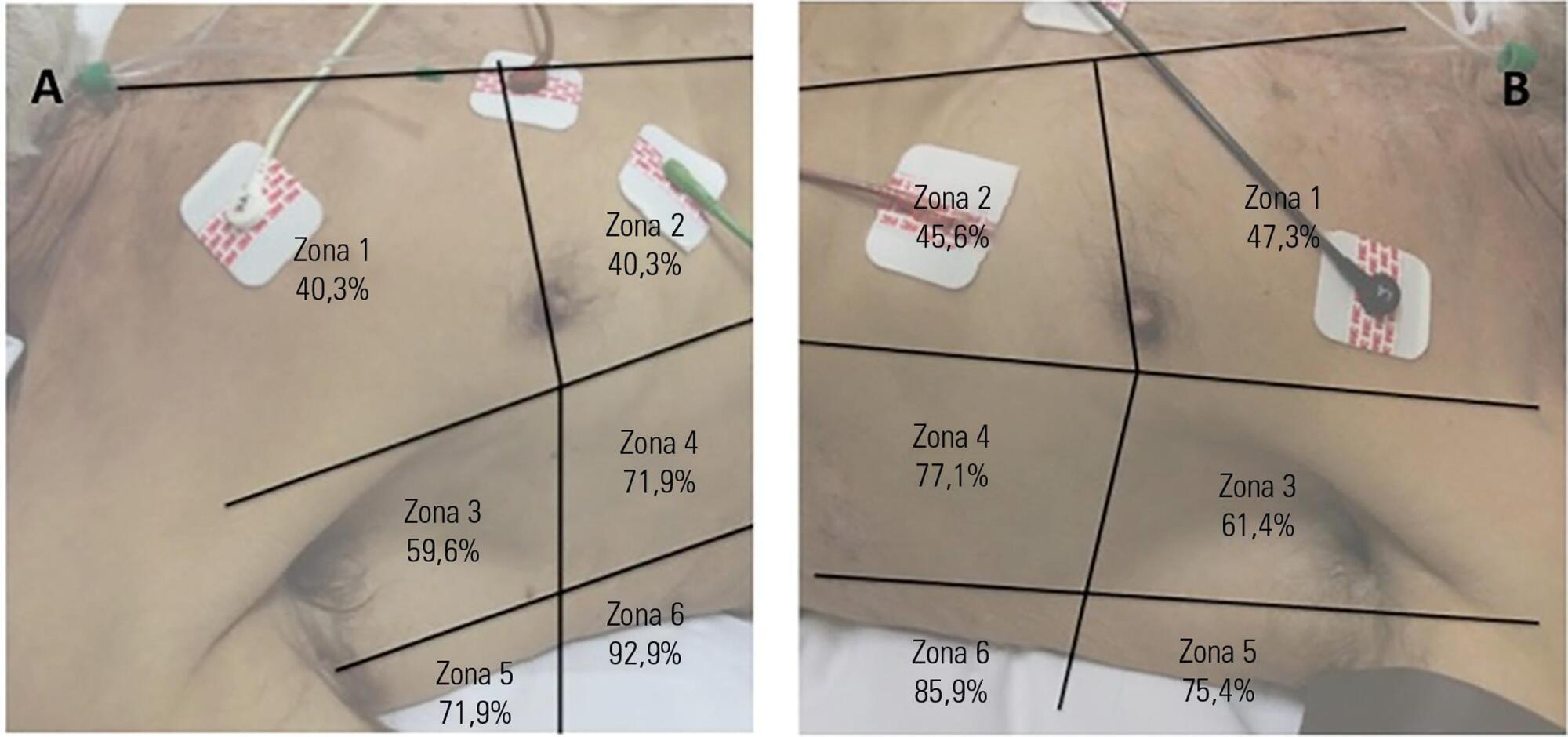
A total of 67 patients with some ventilatory deterioration identified within 12 hours after a pulmonary ultrasonography in the period from November 2016 to March 2017 were analyzed, and all were admitted to an intensive care unit of a private hospital in Belo Horizonte, Minas Gerais. The lung ultrasonographies were performed by three different professionals, termed A, B and C, and the time interval between each lung ultrasonography was less than 3 hours. The only visualized chest zones were the anterior and lateral, defined as right and left anterior (1) zones (Z1R and Z1L, respectively), which were delimited by the clavicle, the sternum and the horizontal line perpendicular to the xiphoid process and anterior axillary line. The right and left lateral (2) zones (Z2R and Z2L, respectively) covered the lateral area between the anterior and posterior axillary lines, with the lower limit being the same horizontal line corresponding to the height of the xiphoid process. A lung zone was considered positive for B lines upon visualization of three or more of these lines, suggesting the presence of alveolar-interstitial syndrome. Using the Kappa value, we evaluated the agreement among the four zones according to the execution of each pair of professionals (AB, AC and BC).
Approximately 80% of the areas that were visualized showed a moderate to substantial agreement, with the Kappa values ranging from 0.41 - 079 (p < 0.05; 95% CI). The highest levels of agreement occurred in the upper zones Z1R and Z1L between subgroups AC and BC, with a Kappa of approximately 0.65 (p < 0.001). In turn, Z2L showed one of the lowest agreements, with a Kappa of 0.36.
The possible limitation of an examiner-dependent effect on lung ultrasounds was not found in this study, suggesting the good reproducibility of this diagnostic modality at the bedside.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):354-360
DOI 10.5935/0103-507X.20190058
To evaluate the agreement between intensive care physicians with similar training in the use of bedside lung ultrasonography in identifying pulmonary B lines, visualized in real time, to verify the reproducibility of the method.
A total of 67 patients with some ventilatory deterioration identified within 12 hours after a pulmonary ultrasonography in the period from November 2016 to March 2017 were analyzed, and all were admitted to an intensive care unit of a private hospital in Belo Horizonte, Minas Gerais. The lung ultrasonographies were performed by three different professionals, termed A, B and C, and the time interval between each lung ultrasonography was less than 3 hours. The only visualized chest zones were the anterior and lateral, defined as right and left anterior (1) zones (Z1R and Z1L, respectively), which were delimited by the clavicle, the sternum and the horizontal line perpendicular to the xiphoid process and anterior axillary line. The right and left lateral (2) zones (Z2R and Z2L, respectively) covered the lateral area between the anterior and posterior axillary lines, with the lower limit being the same horizontal line corresponding to the height of the xiphoid process. A lung zone was considered positive for B lines upon visualization of three or more of these lines, suggesting the presence of alveolar-interstitial syndrome. Using the Kappa value, we evaluated the agreement among the four zones according to the execution of each pair of professionals (AB, AC and BC).
Approximately 80% of the areas that were visualized showed a moderate to substantial agreement, with the Kappa values ranging from 0.41 - 079 (p < 0.05; 95% CI). The highest levels of agreement occurred in the upper zones Z1R and Z1L between subgroups AC and BC, with a Kappa of approximately 0.65 (p < 0.001). In turn, Z2L showed one of the lowest agreements, with a Kappa of 0.36.
The possible limitation of an examiner-dependent effect on lung ultrasounds was not found in this study, suggesting the good reproducibility of this diagnostic modality at the bedside.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
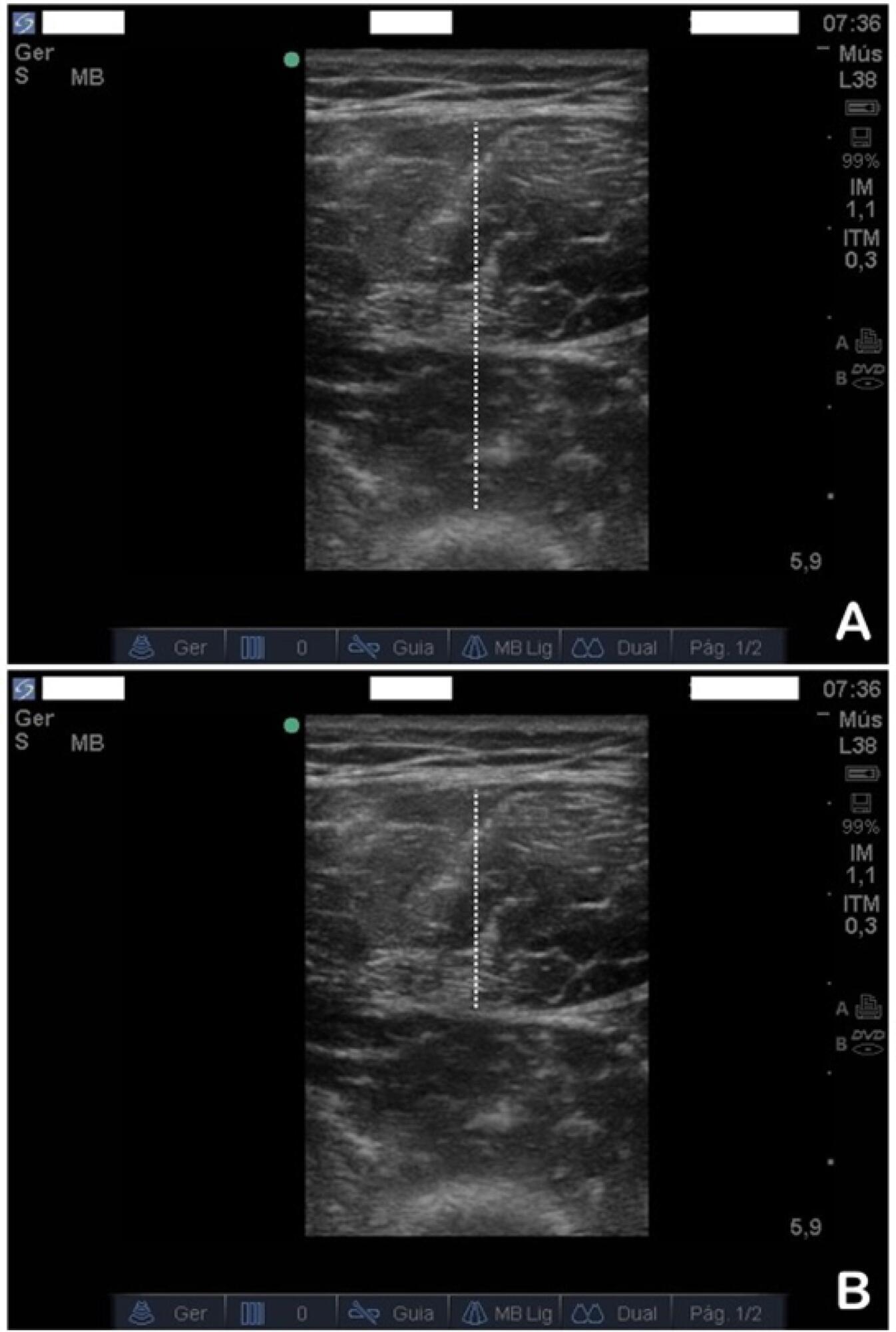
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
A total of 112 images were examined by the coach and compared with the trainees. Pearson's correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
A total of 112 images were examined by the coach and compared with the trainees. Pearson's correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.

Abstract
Rev Bras Ter Intensiva. 2014;26(3):240-252
DOI 10.5935/0103-507X.20140035
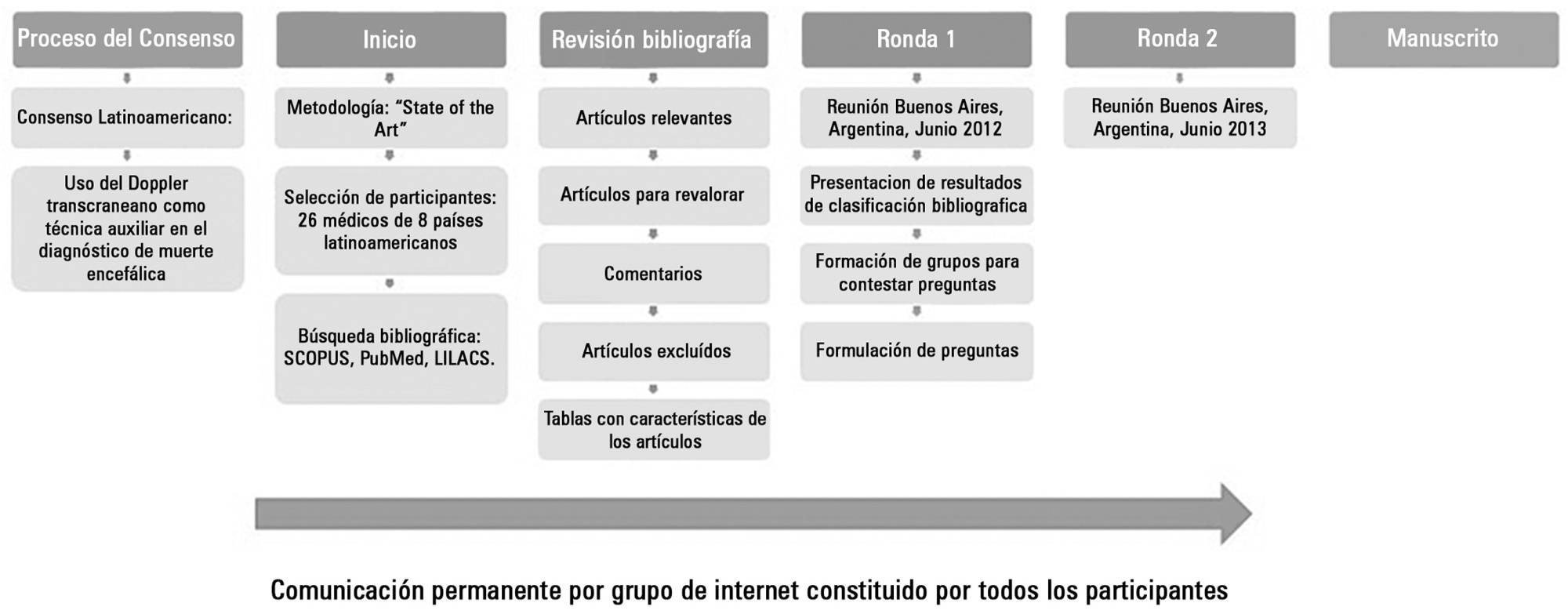
Transcranial Doppler evaluates cerebral hemodynamics in patients with brain injury and is a useful technical tool in diagnosing cerebral circulatory arrest, usually present in the brain-dead patient. This Latin American Consensus was formed by a group of 26 physicians experienced in the use of transcranial Doppler in the context of brain death. The purpose of this agreement was to make recommendations regarding the indications, technique, and interpretation of the study of transcranial ultrasonography in patients with a clinical diagnosis of brain death or in the patient whose clinical diagnosis presents difficulties; a working group was formed to enable further knowledge and to strengthen ties between Latin American physicians working on the same topic.
A review of the literature, concepts, and experiences were exchanged in two meetings and via the Internet. Questions about pathophysiology, equipment, techniques, findings, common problems, and the interpretation of transcranial Doppler in the context of brain death were answered. The basic consensus statements are the following: cerebral circulatory arrest is the final stage in the evolution of progressive intracranial hypertension, which is visualized with transcranial Doppler as a "pattern of cerebral circulatory arrest". The following are accepted as the standard of cerebral circulatory arrest: reverberant pattern, systolic spikes, and absence of previously demonstrated flow. Ultrasonography should be used - in acceptable hemodynamic conditions - in the anterior circulation bilaterally (middle cerebral artery) and in the posterior (basilar artery) territory. If no ultrasonographic images are found in any or all of these vessels, their proximal arteries are acceptable to be studied to look for a a pattern of cerebral circulatory arrest.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):240-252
DOI 10.5935/0103-507X.20140035
Transcranial Doppler evaluates cerebral hemodynamics in patients with brain injury and is a useful technical tool in diagnosing cerebral circulatory arrest, usually present in the brain-dead patient. This Latin American Consensus was formed by a group of 26 physicians experienced in the use of transcranial Doppler in the context of brain death. The purpose of this agreement was to make recommendations regarding the indications, technique, and interpretation of the study of transcranial ultrasonography in patients with a clinical diagnosis of brain death or in the patient whose clinical diagnosis presents difficulties; a working group was formed to enable further knowledge and to strengthen ties between Latin American physicians working on the same topic.
A review of the literature, concepts, and experiences were exchanged in two meetings and via the Internet. Questions about pathophysiology, equipment, techniques, findings, common problems, and the interpretation of transcranial Doppler in the context of brain death were answered. The basic consensus statements are the following: cerebral circulatory arrest is the final stage in the evolution of progressive intracranial hypertension, which is visualized with transcranial Doppler as a "pattern of cerebral circulatory arrest". The following are accepted as the standard of cerebral circulatory arrest: reverberant pattern, systolic spikes, and absence of previously demonstrated flow. Ultrasonography should be used - in acceptable hemodynamic conditions - in the anterior circulation bilaterally (middle cerebral artery) and in the posterior (basilar artery) territory. If no ultrasonographic images are found in any or all of these vessels, their proximal arteries are acceptable to be studied to look for a a pattern of cerebral circulatory arrest.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (33) COVID-19 (45) Critical care (115) Critical illness (54) ICU (25) Infant, newborn (27) Intensive care (72) Intensive care units (254) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (75) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (117) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)