Muscular atrophy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
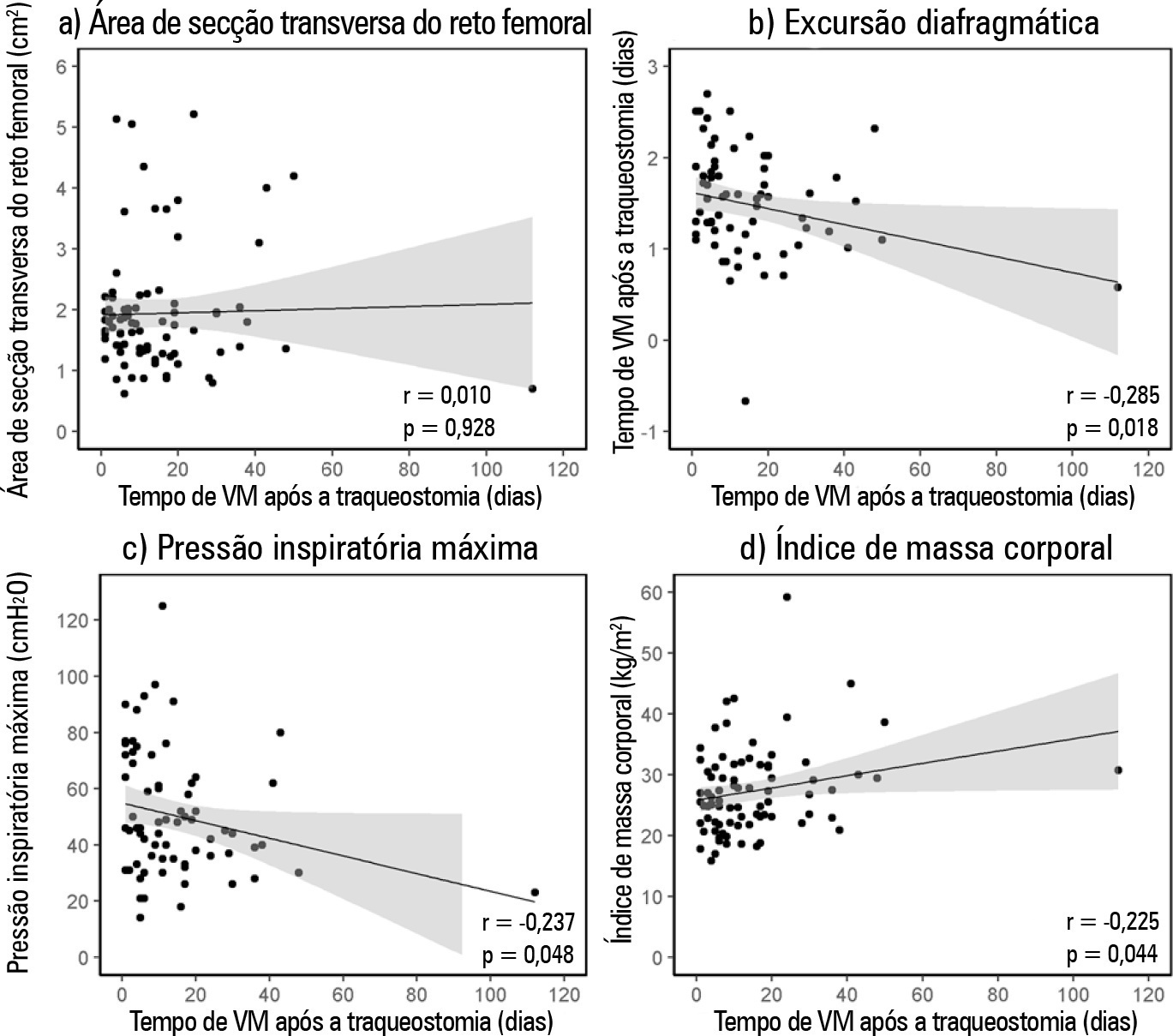
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 - 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 - 1.08; p = 0.061).
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):452-460
DOI 10.5935/0103-507X.20220087-en
To verify the relationship between the rectus femoris cross-sectional area and diaphragmatic excursion with successful weaning from mechanical ventilation in chronic critically tracheostomized patients.
This was a prospective observational cohort study. We included chronic critically ill patients (those who underwent tracheostomy placement after 10 days under mechanical ventilation). The rectus femoris cross-sectional area and diaphragmatic excursion were obtained by ultrasonography performed within the first 48 hours after tracheostomy. We measured rectus femoris cross-sectional area and diaphragmatic excursion to assess their association with weaning from mechanical ventilation, including their potential to predict successful weaning and survival throughout the intensive care unit stay.
Eighty-one patients were included. Forty-five patients (55%) were weaned from mechanical ventilation. The mortality rates were 42% and 61.7% in the intensive care unit and hospital, respectively. The fail group in relation to the success group at weaning presented a lower rectus femoris cross-sectional area (1.4 [0.8] versus 1.84 [0.76]cm2, p = 0.014) and lower diaphragmatic excursion (1.29 ± 0.62 versus 1.62 ± 0.51cm, p = 0.019). When rectus femoris cross-sectional area ≥ 1.80cm2 and diaphragmatic excursion ≥ 1.25cm was a combined condition, it had a strong association with successful weaning (adjusted OR = 20.81, 95%CI 2.38 - 182.28; p = 0.006) but not with intensive care unit survival (adjusted OR = 0.19, 95%CI 0.03 - 1.08; p = 0.061).
Successful weaning from mechanical ventilation in chronic critically ill patients was associated with higher measurements of rectus femoris cross-sectional area and diaphragmatic excursion.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):188-196
DOI 10.1590/S0103-507X2012000200016
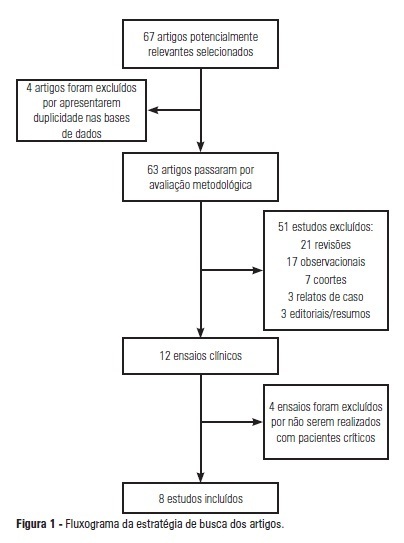
OBJECTIVE: To analyze the outcomes achieved by motor physical therapy in critically ill patients admitted to intensive care units. METHODS: A systematic literature review was performed, and clinical trials published between 2002 and 2011 were included in the study. The search involved the LILACS, SciELO, MedLine, EMBASE and Cochrane databases, using the keywords "intensive care unit", "physiotherapy", "physical therapy", "mobility", "mobilization" and "randomized controlled trials." Two researchers screened the articles independently and included works that addressed the effect of physical therapy on critically ill patients. RESULTS: From an initial analysis of 67 potentially relevant articles, only 8 met the selection criteria and addressed the outcomes of electrostimulation, cycle ergometry and kinesiotherapy techniques. The sample sizes ranged from 8 to 101 subjects, with mean ages between 52 and 79 years. All patients were undergoing invasive mechanical ventilation. Among the analyzed articles, 6 reported significant benefits of motor physical therapy, such as improvement in peripheral muscle strength, respiratory capacity and functionality, in critically ill patients. CONCLUSION: With this systematic review, it is possible to conclude that motor physical therapy is a feasible and safe therapy for critically ill patients and can minimize the deleterious effects of prolonged immobilization. Approaches involving electrostimulation, cycle ergometry and kinesiotherapy showed positive responses in patients under intensive care. Available evidence regarding the impact of motor physical therapy on length of stay in intensive care units and on mortality is still scarce, and further study in this area is warranted.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):188-196
DOI 10.1590/S0103-507X2012000200016
OBJECTIVE: To analyze the outcomes achieved by motor physical therapy in critically ill patients admitted to intensive care units. METHODS: A systematic literature review was performed, and clinical trials published between 2002 and 2011 were included in the study. The search involved the LILACS, SciELO, MedLine, EMBASE and Cochrane databases, using the keywords "intensive care unit", "physiotherapy", "physical therapy", "mobility", "mobilization" and "randomized controlled trials." Two researchers screened the articles independently and included works that addressed the effect of physical therapy on critically ill patients. RESULTS: From an initial analysis of 67 potentially relevant articles, only 8 met the selection criteria and addressed the outcomes of electrostimulation, cycle ergometry and kinesiotherapy techniques. The sample sizes ranged from 8 to 101 subjects, with mean ages between 52 and 79 years. All patients were undergoing invasive mechanical ventilation. Among the analyzed articles, 6 reported significant benefits of motor physical therapy, such as improvement in peripheral muscle strength, respiratory capacity and functionality, in critically ill patients. CONCLUSION: With this systematic review, it is possible to conclude that motor physical therapy is a feasible and safe therapy for critically ill patients and can minimize the deleterious effects of prolonged immobilization. Approaches involving electrostimulation, cycle ergometry and kinesiotherapy showed positive responses in patients under intensive care. Available evidence regarding the impact of motor physical therapy on length of stay in intensive care units and on mortality is still scarce, and further study in this area is warranted.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)