Exercise therapy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
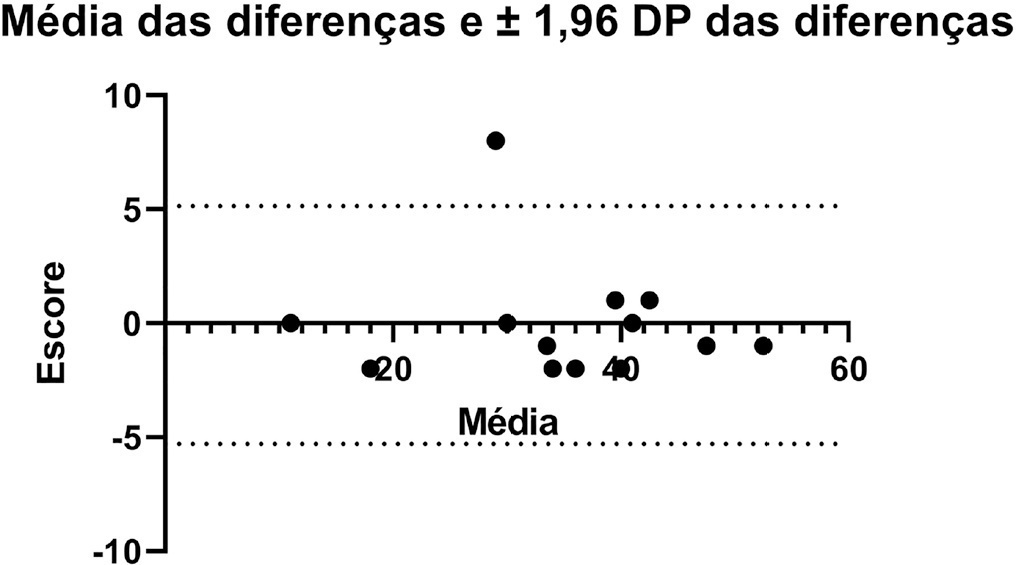
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):188-196
DOI 10.1590/S0103-507X2012000200016
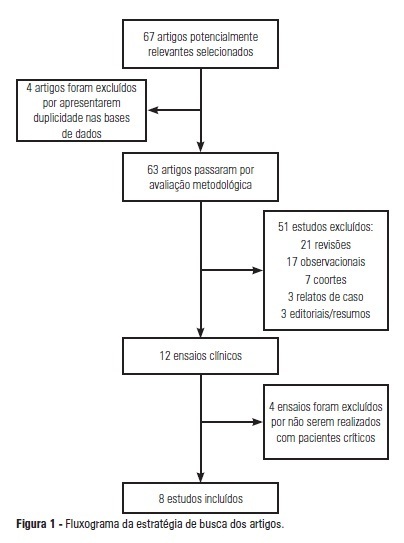
OBJECTIVE: To analyze the outcomes achieved by motor physical therapy in critically ill patients admitted to intensive care units. METHODS: A systematic literature review was performed, and clinical trials published between 2002 and 2011 were included in the study. The search involved the LILACS, SciELO, MedLine, EMBASE and Cochrane databases, using the keywords "intensive care unit", "physiotherapy", "physical therapy", "mobility", "mobilization" and "randomized controlled trials." Two researchers screened the articles independently and included works that addressed the effect of physical therapy on critically ill patients. RESULTS: From an initial analysis of 67 potentially relevant articles, only 8 met the selection criteria and addressed the outcomes of electrostimulation, cycle ergometry and kinesiotherapy techniques. The sample sizes ranged from 8 to 101 subjects, with mean ages between 52 and 79 years. All patients were undergoing invasive mechanical ventilation. Among the analyzed articles, 6 reported significant benefits of motor physical therapy, such as improvement in peripheral muscle strength, respiratory capacity and functionality, in critically ill patients. CONCLUSION: With this systematic review, it is possible to conclude that motor physical therapy is a feasible and safe therapy for critically ill patients and can minimize the deleterious effects of prolonged immobilization. Approaches involving electrostimulation, cycle ergometry and kinesiotherapy showed positive responses in patients under intensive care. Available evidence regarding the impact of motor physical therapy on length of stay in intensive care units and on mortality is still scarce, and further study in this area is warranted.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):188-196
DOI 10.1590/S0103-507X2012000200016
OBJECTIVE: To analyze the outcomes achieved by motor physical therapy in critically ill patients admitted to intensive care units. METHODS: A systematic literature review was performed, and clinical trials published between 2002 and 2011 were included in the study. The search involved the LILACS, SciELO, MedLine, EMBASE and Cochrane databases, using the keywords "intensive care unit", "physiotherapy", "physical therapy", "mobility", "mobilization" and "randomized controlled trials." Two researchers screened the articles independently and included works that addressed the effect of physical therapy on critically ill patients. RESULTS: From an initial analysis of 67 potentially relevant articles, only 8 met the selection criteria and addressed the outcomes of electrostimulation, cycle ergometry and kinesiotherapy techniques. The sample sizes ranged from 8 to 101 subjects, with mean ages between 52 and 79 years. All patients were undergoing invasive mechanical ventilation. Among the analyzed articles, 6 reported significant benefits of motor physical therapy, such as improvement in peripheral muscle strength, respiratory capacity and functionality, in critically ill patients. CONCLUSION: With this systematic review, it is possible to conclude that motor physical therapy is a feasible and safe therapy for critically ill patients and can minimize the deleterious effects of prolonged immobilization. Approaches involving electrostimulation, cycle ergometry and kinesiotherapy showed positive responses in patients under intensive care. Available evidence regarding the impact of motor physical therapy on length of stay in intensive care units and on mortality is still scarce, and further study in this area is warranted.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)