Infant, newborn Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children's Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.
Abstract
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children's Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
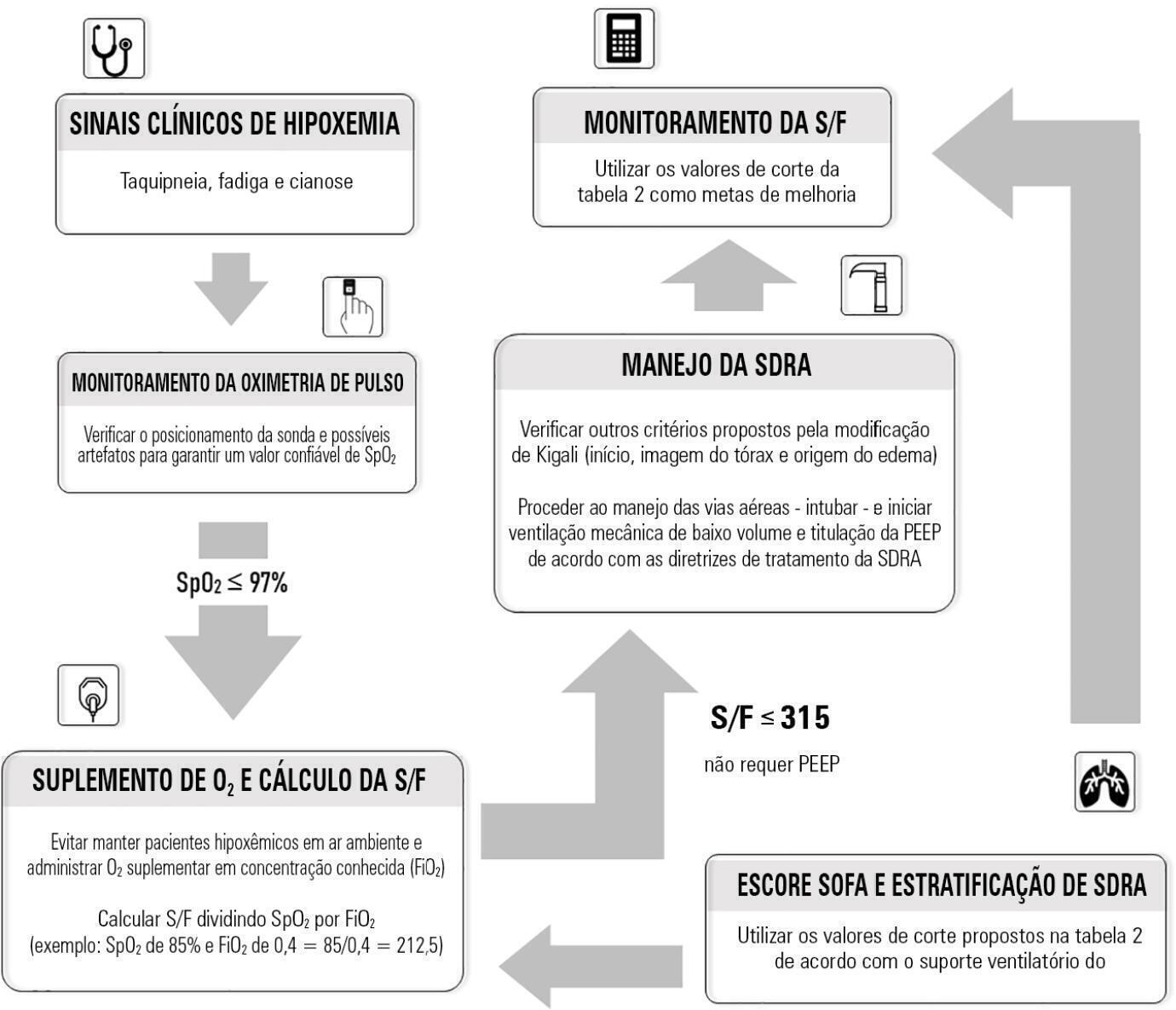
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 - 6), 24.2% (n = 15) had mild to moderate pain (7 - 11) and 45.2% (28) had severe pain (12 - 21). It was found that health professionals identified pain during the procedure.
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 - 6), 24.2% (n = 15) had mild to moderate pain (7 - 11) and 45.2% (28) had severe pain (12 - 21). It was found that health professionals identified pain during the procedure.
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):266-275
DOI 10.5935/0103-507X.20210034
To evaluate the use of off-label and unlicensed medications in preterm infants hospitalized in a neonatal intensive care unit.
This nonconcurrent cohort study included preterm infants admitted to 3 neonatal intensive care units in 2016 and 2017 who were followed up during the neonatal period. The type and number of medications used were recorded for the entire period and classified based on the Anatomical Therapeutic Chemical. Descriptive and bivariate data analyses were performed to assess associations between the number of drugs used (total, off-label and unlicensed) and the explanatory variables of interest.
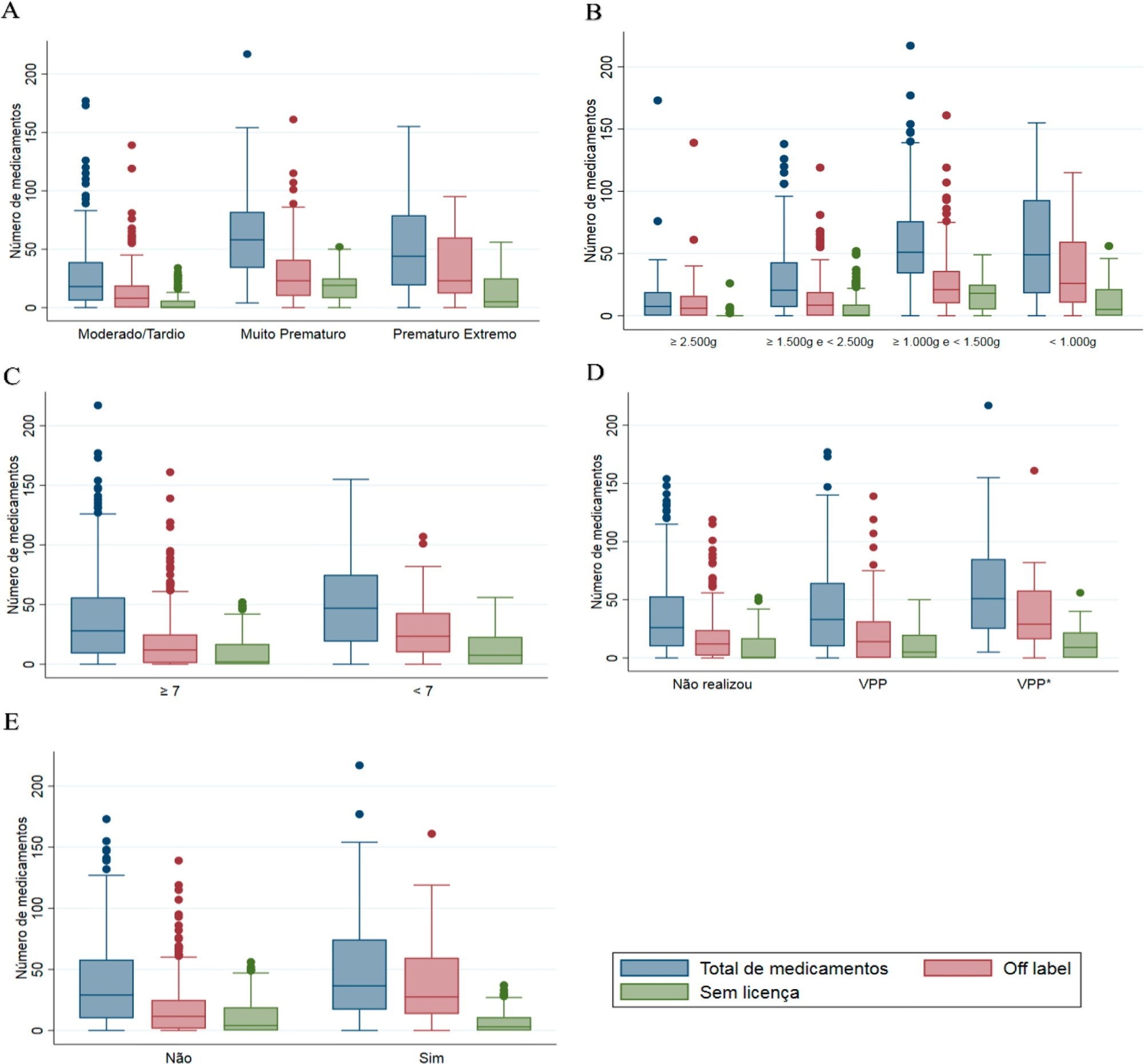
Four hundred preterm infants received 16,143 prescriptions for 86 different pharmaceuticals; 51.9% of these medications were classified as off-label and 23.5% as unlicensed. The most prescribed drugs were gentamicin and ampicillin (17.5% and 15.5% among off-label, respectively) and caffeine (75.5% among unlicensed). The results indicated significant associations between the use of off-label drugs and lower gestational age, low birth weight, lower 5-minute Apgar score, advanced resuscitation maneuver in the delivery room and death. The prescription of unlicensed drugs was associated with lower gestational age, low birth weight and 5-minute Apgar score below 7.
Neonates admitted to neonatal intensive care units are highly exposed to off-label and unlicensed medications. Further studies are needed to achieve greater safety and quality of drug therapy used in neonatology.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):266-275
DOI 10.5935/0103-507X.20210034
To evaluate the use of off-label and unlicensed medications in preterm infants hospitalized in a neonatal intensive care unit.
This nonconcurrent cohort study included preterm infants admitted to 3 neonatal intensive care units in 2016 and 2017 who were followed up during the neonatal period. The type and number of medications used were recorded for the entire period and classified based on the Anatomical Therapeutic Chemical. Descriptive and bivariate data analyses were performed to assess associations between the number of drugs used (total, off-label and unlicensed) and the explanatory variables of interest.
Four hundred preterm infants received 16,143 prescriptions for 86 different pharmaceuticals; 51.9% of these medications were classified as off-label and 23.5% as unlicensed. The most prescribed drugs were gentamicin and ampicillin (17.5% and 15.5% among off-label, respectively) and caffeine (75.5% among unlicensed). The results indicated significant associations between the use of off-label drugs and lower gestational age, low birth weight, lower 5-minute Apgar score, advanced resuscitation maneuver in the delivery room and death. The prescription of unlicensed drugs was associated with lower gestational age, low birth weight and 5-minute Apgar score below 7.
Neonates admitted to neonatal intensive care units are highly exposed to off-label and unlicensed medications. Further studies are needed to achieve greater safety and quality of drug therapy used in neonatology.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):12-30
DOI 10.5935/0103-507X.20210002
To present guidelines on sensory motor stimulation for newborns and infants in the intensive care unit.
We employed a mixed methods design with a systematic review of the literature and recommendations based on scientific evidence and the opinions of physiotherapists with neonatal expertise. The research included studies published between 2010 and 2018 in the MEDLINE® and Cochrane databases that included newborns (preterm and term) and infants (between 28 days and 6 months of age) hospitalized in the intensive care unit and submitted to sensory motor stimulation methods. The studies found were classified according to the GRADE score by five physiotherapists in different regions of Brazil and presented at eight Scientific Congresses held to discuss the clinical practice guidelines.
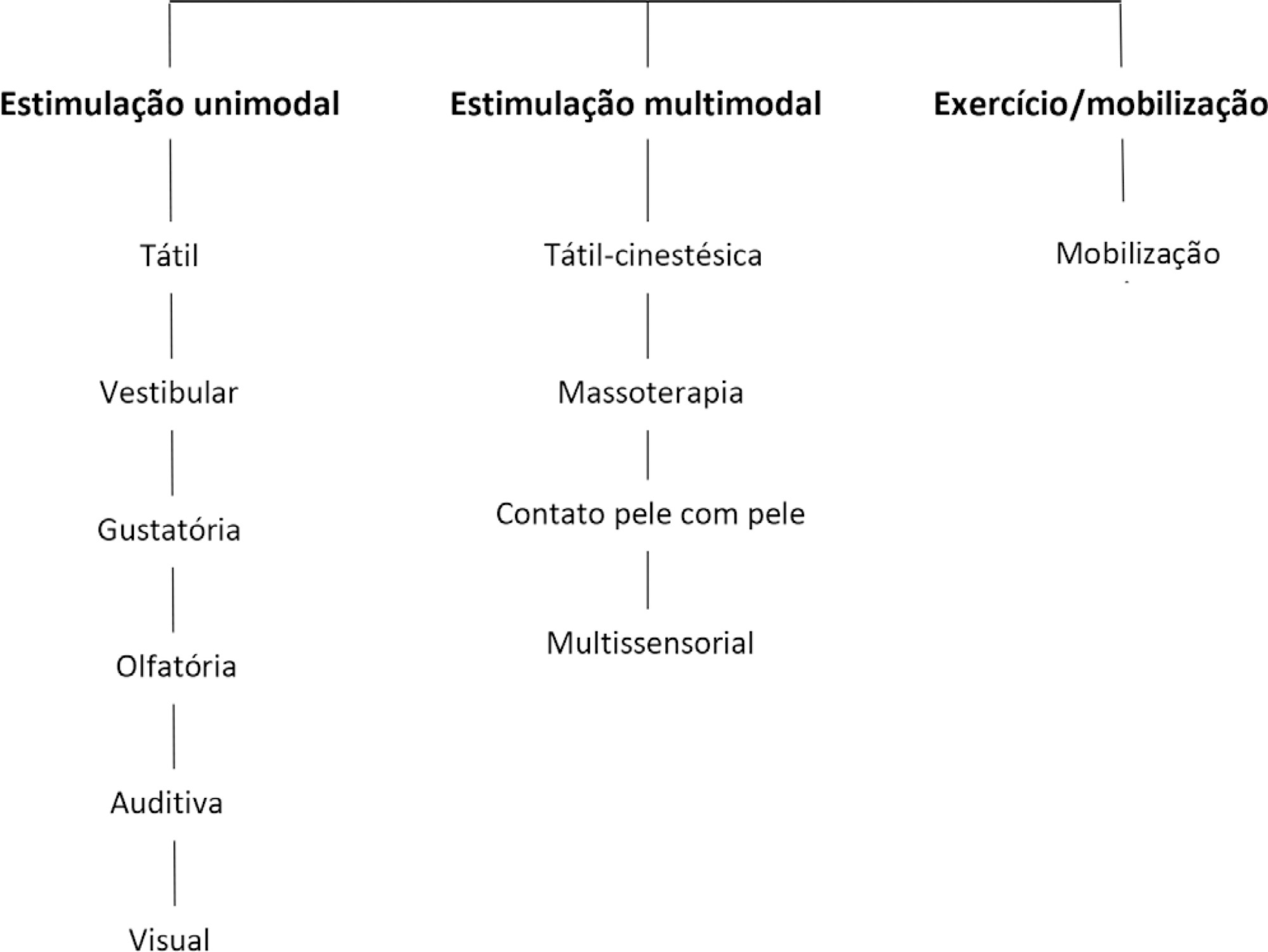
We included 89 articles to construct the clinical practice guidelines. Auditory, gustatory and skin-to-skin stimulation stand out for enhancing vital signs, and tactile-kinesthetic massage and multisensory stimulation stand out for improving weight or sucking.
Although all modalities have good ratings for pain or stress control, it is recommended that sensory motor stimulation procedures be tailored to the infant’s specific needs and that interventions and be carried out by expert professionals.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):12-30
DOI 10.5935/0103-507X.20210002
To present guidelines on sensory motor stimulation for newborns and infants in the intensive care unit.
We employed a mixed methods design with a systematic review of the literature and recommendations based on scientific evidence and the opinions of physiotherapists with neonatal expertise. The research included studies published between 2010 and 2018 in the MEDLINE® and Cochrane databases that included newborns (preterm and term) and infants (between 28 days and 6 months of age) hospitalized in the intensive care unit and submitted to sensory motor stimulation methods. The studies found were classified according to the GRADE score by five physiotherapists in different regions of Brazil and presented at eight Scientific Congresses held to discuss the clinical practice guidelines.
We included 89 articles to construct the clinical practice guidelines. Auditory, gustatory and skin-to-skin stimulation stand out for enhancing vital signs, and tactile-kinesthetic massage and multisensory stimulation stand out for improving weight or sucking.
Although all modalities have good ratings for pain or stress control, it is recommended that sensory motor stimulation procedures be tailored to the infant’s specific needs and that interventions and be carried out by expert professionals.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):578-584
DOI 10.5935/0103-507X.20200096
To determine the concordance of mortality risk classification through the use of the Pediatric Index of Mortality (PIM) 2 and 3.
Through a retrospective cohort, we evaluated patients admitted to the pediatric intensive care unit between April 2016 and December 2018. We calculated the mortality risk with the PIM 2 and 3. Analyses were carried out to determine the concordance between the risk classification obtained with both scales using unweighted and linearly weighted kappa.
A total of 722 subjects were included, and 66.6% had a chronic condition. The overall mortality was 3.7%. The global kappa concordance coefficient for classifying patients according to risk with the PIM 2 and 3 was moderate at 0.48 (95%CI 0.43 - 0.53). After linear weighting, concordance was substantial at 0.64 (95%CI 0.59 - 0.69). For cardiac surgery patients, concordance for risk classification was fair at 0.30 (95%CI 0.21 - 0.39), and after linear weighting, concordance was only moderate at 0.49 (95%CI 0.39 - 0.59). The PIM 3 assigned a lower risk than the PIM 2 in 44.8% of patients in this subgroup.
Our study proves that the PIM 2 and 3 are not clinically equivalent and should not be used interchangeably for quality evaluation across pediatric intensive care units. Validation studies must be performed before using the PIM 2 or PIM 3 in specific settings.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):578-584
DOI 10.5935/0103-507X.20200096
To determine the concordance of mortality risk classification through the use of the Pediatric Index of Mortality (PIM) 2 and 3.
Through a retrospective cohort, we evaluated patients admitted to the pediatric intensive care unit between April 2016 and December 2018. We calculated the mortality risk with the PIM 2 and 3. Analyses were carried out to determine the concordance between the risk classification obtained with both scales using unweighted and linearly weighted kappa.
A total of 722 subjects were included, and 66.6% had a chronic condition. The overall mortality was 3.7%. The global kappa concordance coefficient for classifying patients according to risk with the PIM 2 and 3 was moderate at 0.48 (95%CI 0.43 - 0.53). After linear weighting, concordance was substantial at 0.64 (95%CI 0.59 - 0.69). For cardiac surgery patients, concordance for risk classification was fair at 0.30 (95%CI 0.21 - 0.39), and after linear weighting, concordance was only moderate at 0.49 (95%CI 0.39 - 0.59). The PIM 3 assigned a lower risk than the PIM 2 in 44.8% of patients in this subgroup.
Our study proves that the PIM 2 and 3 are not clinically equivalent and should not be used interchangeably for quality evaluation across pediatric intensive care units. Validation studies must be performed before using the PIM 2 or PIM 3 in specific settings.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):296-302
DOI 10.5935/0103-507X.20190054
Evaluate the physiological and autonomic nervous system responses of premature newborns to body position and noise in the neonatal intensive care unit.
A quasi-experimental study. The autonomic nervous system of newborns was evaluated based on heart rate variability when the newborns were exposed to environmental noise and placed in different positions: supine without support, supine with manual restraint and prone.
Fifty premature newborns were evaluated (gestational age: 32.6 ± 2.3 weeks; weight: 1816 ± 493g; and Brazelton sleep/awake level: 3 to 4). A positive correlation was found between environmental noise and sympathetic activity (R = 0.27, p = 0.04). The mean environmental noise was 53 ± 14dB. The heart rate was higher in the supine position than in the manual restraint and prone positions (148.7 ± 21.6, 141.9 ± 16 and 144 ± 13, respectively) (p = 0.001). Sympathetic activity, represented by a low frequency index, was higher in the supine position (p < 0.05) than in the other positions, and parasympathetic activity (high frequency, root mean square of the sum of differences between normal adjacent mean R-R interval and percentage of adjacent iRR that differed by more than 50ms) was higher in the prone position (p < 0.05) than in the other positions. The complexity of the autonomic adjustments (approximate entropy and sample entropy) was lower in the supine position than in the other positions.
The prone position and manual restraint position increased both parasympathetic activity and the complexity of autonomic adjustments in comparison to the supine position, even in the presence of higher environmental noise than the recommended level, which tends to increase sympathetic activity.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):296-302
DOI 10.5935/0103-507X.20190054
Evaluate the physiological and autonomic nervous system responses of premature newborns to body position and noise in the neonatal intensive care unit.
A quasi-experimental study. The autonomic nervous system of newborns was evaluated based on heart rate variability when the newborns were exposed to environmental noise and placed in different positions: supine without support, supine with manual restraint and prone.
Fifty premature newborns were evaluated (gestational age: 32.6 ± 2.3 weeks; weight: 1816 ± 493g; and Brazelton sleep/awake level: 3 to 4). A positive correlation was found between environmental noise and sympathetic activity (R = 0.27, p = 0.04). The mean environmental noise was 53 ± 14dB. The heart rate was higher in the supine position than in the manual restraint and prone positions (148.7 ± 21.6, 141.9 ± 16 and 144 ± 13, respectively) (p = 0.001). Sympathetic activity, represented by a low frequency index, was higher in the supine position (p < 0.05) than in the other positions, and parasympathetic activity (high frequency, root mean square of the sum of differences between normal adjacent mean R-R interval and percentage of adjacent iRR that differed by more than 50ms) was higher in the prone position (p < 0.05) than in the other positions. The complexity of the autonomic adjustments (approximate entropy and sample entropy) was lower in the supine position than in the other positions.
The prone position and manual restraint position increased both parasympathetic activity and the complexity of autonomic adjustments in comparison to the supine position, even in the presence of higher environmental noise than the recommended level, which tends to increase sympathetic activity.

Abstract
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (33) COVID-19 (45) Critical care (115) Critical illness (54) Infant, newborn (27) Intensive care (72) Intensive care units (254) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (75) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (117) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98) Septic shock (25)