Pain Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 - 6), 24.2% (n = 15) had mild to moderate pain (7 - 11) and 45.2% (28) had severe pain (12 - 21). It was found that health professionals identified pain during the procedure.
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):434-439
DOI 10.5935/0103-507X.20210058
To evaluate pain intensity during arterial puncture performed in newborns admitted to a neonatal progressive care unit and to evaluate the perception of health professionals regarding neonatal pain.
This was an observational analytical study in which 62 arterial punctures were performed in 35 neonates. Pain was assessed during collection using the Premature Infant Pain Profile scale. The health professionals responsible for collection evaluated pain using a verbal numerical scale ranging from zero to ten. The data were subjected to descriptive statistical analysis using the Statistical Package for the Social Science software.
Among the newborns, 30.6% (n = 19) had no pain or mild pain (0 - 6), 24.2% (n = 15) had mild to moderate pain (7 - 11) and 45.2% (28) had severe pain (12 - 21). It was found that health professionals identified pain during the procedure.
Arterial puncture is considered a painful procedure that can result in mild to severe pain. The adoption of systematic evaluation strategies is necessary to enable appropriate therapeutic intervention.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):48-67
DOI 10.5935/0103-507X.20210005
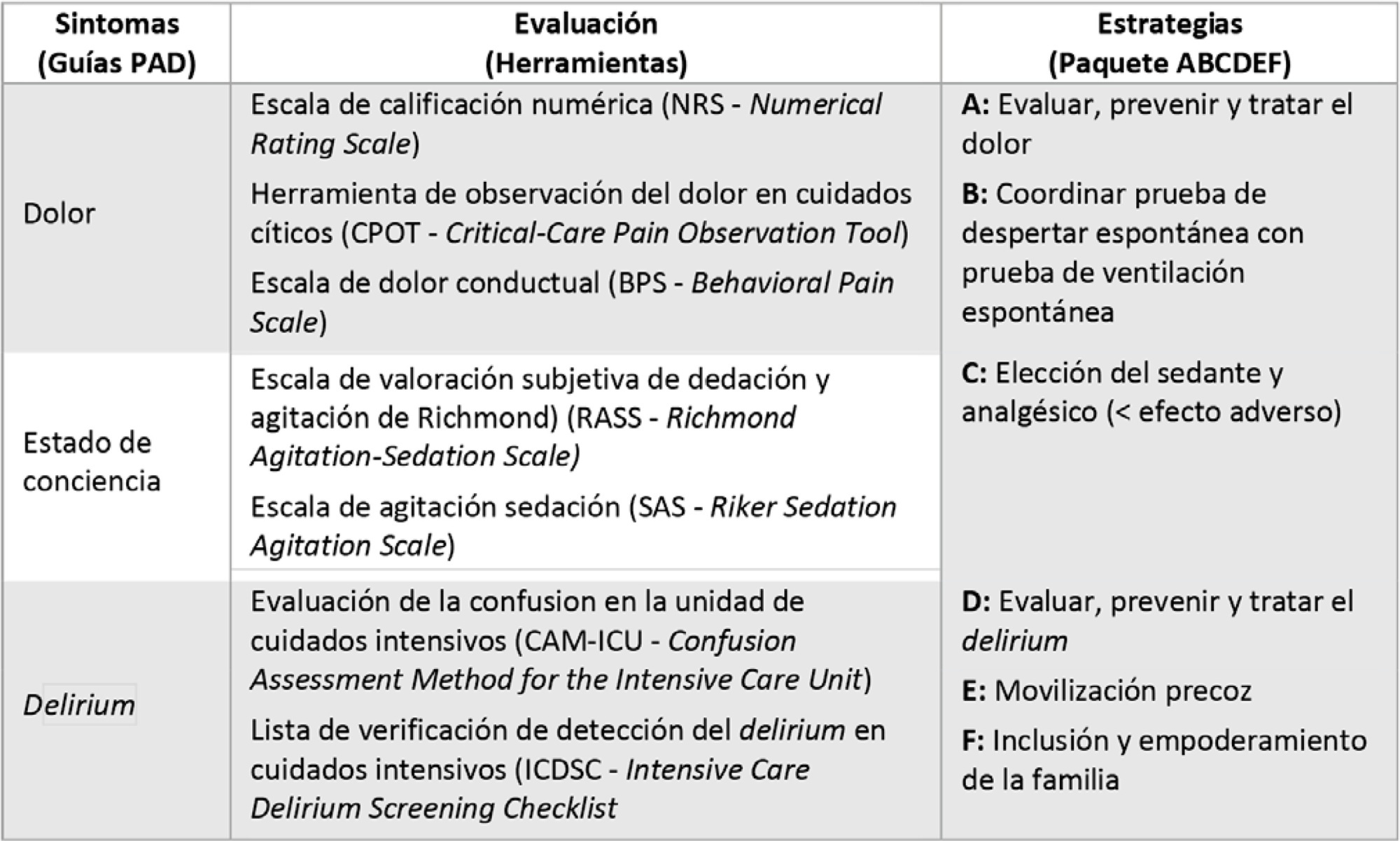
To propose agile strategies for a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for patients with COVID-19-associated acute respiratory distress syndrome, considering the high risk of infection among health workers, the humanitarian treatment that we must provide to patients and the inclusion of patients’ families, in a context lacking specific therapeutic strategies against the virus globally available to date and a potential lack of health resources.
A nonsystematic review of the scientific evidence in the main bibliographic databases was carried out, together with national and international clinical experience and judgment. Finally, a consensus of recommendations was made among the members of the Committee for Analgesia, Sedation and Delirium of the Sociedad Argentina de Terapia Intensiva.
Recommendations were agreed upon, and tools were developed to ensure a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for adult patients with acute respiratory distress syndrome due to COVID-19.
Given the new order generated in intensive therapies due to the advancing COVID-19 pandemic, we propose to not leave aside the usual good practices but to adapt them to the particular context generated. Our consensus is supported by scientific evidence and national and international experience and will be an attractive consultation tool in intensive therapies.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):48-67
DOI 10.5935/0103-507X.20210005
To propose agile strategies for a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for patients with COVID-19-associated acute respiratory distress syndrome, considering the high risk of infection among health workers, the humanitarian treatment that we must provide to patients and the inclusion of patients’ families, in a context lacking specific therapeutic strategies against the virus globally available to date and a potential lack of health resources.
A nonsystematic review of the scientific evidence in the main bibliographic databases was carried out, together with national and international clinical experience and judgment. Finally, a consensus of recommendations was made among the members of the Committee for Analgesia, Sedation and Delirium of the Sociedad Argentina de Terapia Intensiva.
Recommendations were agreed upon, and tools were developed to ensure a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for adult patients with acute respiratory distress syndrome due to COVID-19.
Given the new order generated in intensive therapies due to the advancing COVID-19 pandemic, we propose to not leave aside the usual good practices but to adapt them to the particular context generated. Our consensus is supported by scientific evidence and national and international experience and will be an attractive consultation tool in intensive therapies.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):66-71
DOI 10.5935/0103-507X.20200011
To temporally assess a painful stimulus in premature infants using 3 neonatal pain scales.
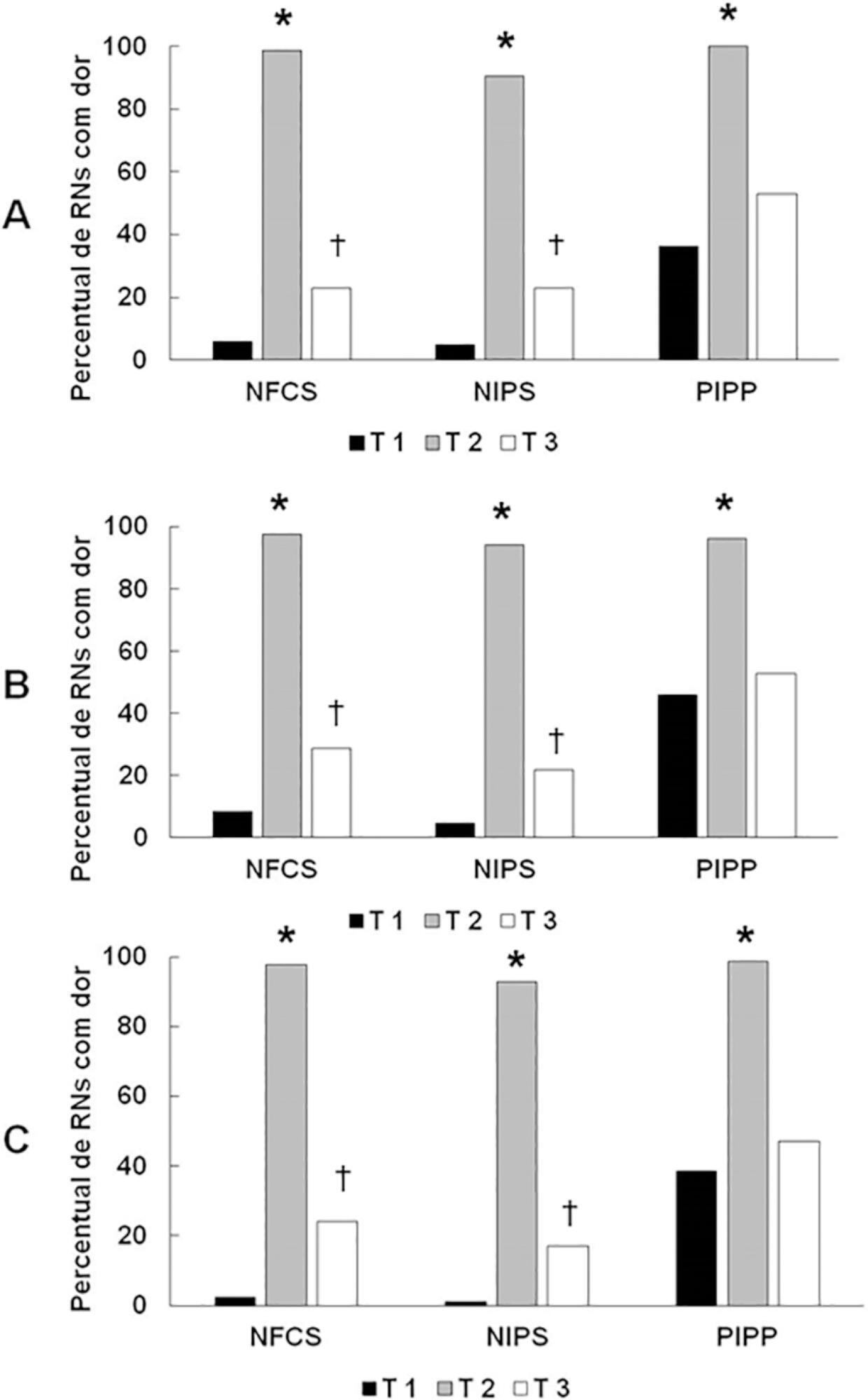
A total of 83 premature infants were observed during airway aspiration by 3 evaluators (E1, E2 and E3) using 3 pain assessment scales (Neonatal Facial Coding System - NFCS; Neonatal Infant Pain Scale - NIPS; and Premature Infant Pain Profile - PIPP) at 5 time points: T1 (before airway aspiration), T2 (during airway aspiration), T3 (1 minute after airway aspiration), T4 (3 minutes after airway aspiration), and T5 (5 minutes after airway aspiration). Light’s Kappa (agreement among examiners and among scales at each time point) and the McNemar test (comparison among time points) were used considering p < 0.05.
There was a significant difference between the 3 examiners for T1 and T2 using the 3 scales. In T3, pain was observed in 22.9%/E1, 28.9%/E2, and 24.1%/E3 according to the NFCS; 22.9%/E1, 21.7%/E2, and 16.9%/E3 according to the NIPS; and 49.4%/E1, 53.9%/E2, and 47%/E3 according to the PIPP. There was a difference between T1 and T3 using the 3 scales, except for 2 examiners for the PIPP (E2: p = 0.15/E3: p = 0.17). Comparing T4 and T5 to T1, there was no difference in the 3 scales.
Premature infants required at least 3 minutes to return to their initial state of rest (no pain).
Abstract
Rev Bras Ter Intensiva. 2020;32(1):66-71
DOI 10.5935/0103-507X.20200011
To temporally assess a painful stimulus in premature infants using 3 neonatal pain scales.
A total of 83 premature infants were observed during airway aspiration by 3 evaluators (E1, E2 and E3) using 3 pain assessment scales (Neonatal Facial Coding System - NFCS; Neonatal Infant Pain Scale - NIPS; and Premature Infant Pain Profile - PIPP) at 5 time points: T1 (before airway aspiration), T2 (during airway aspiration), T3 (1 minute after airway aspiration), T4 (3 minutes after airway aspiration), and T5 (5 minutes after airway aspiration). Light’s Kappa (agreement among examiners and among scales at each time point) and the McNemar test (comparison among time points) were used considering p < 0.05.
There was a significant difference between the 3 examiners for T1 and T2 using the 3 scales. In T3, pain was observed in 22.9%/E1, 28.9%/E2, and 24.1%/E3 according to the NFCS; 22.9%/E1, 21.7%/E2, and 16.9%/E3 according to the NIPS; and 49.4%/E1, 53.9%/E2, and 47%/E3 according to the PIPP. There was a difference between T1 and T3 using the 3 scales, except for 2 examiners for the PIPP (E2: p = 0.15/E3: p = 0.17). Comparing T4 and T5 to T1, there was no difference in the 3 scales.
Premature infants required at least 3 minutes to return to their initial state of rest (no pain).
Abstract
Rev Bras Ter Intensiva. 2019;31(4):571-581
DOI 10.5935/0103-507X.20190070
Descrever a adequação de duas escalas comportamentais, a Behavioral Pain Scale e a Critical Care Pain Observation Tool, para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidades de terapia intensiva.
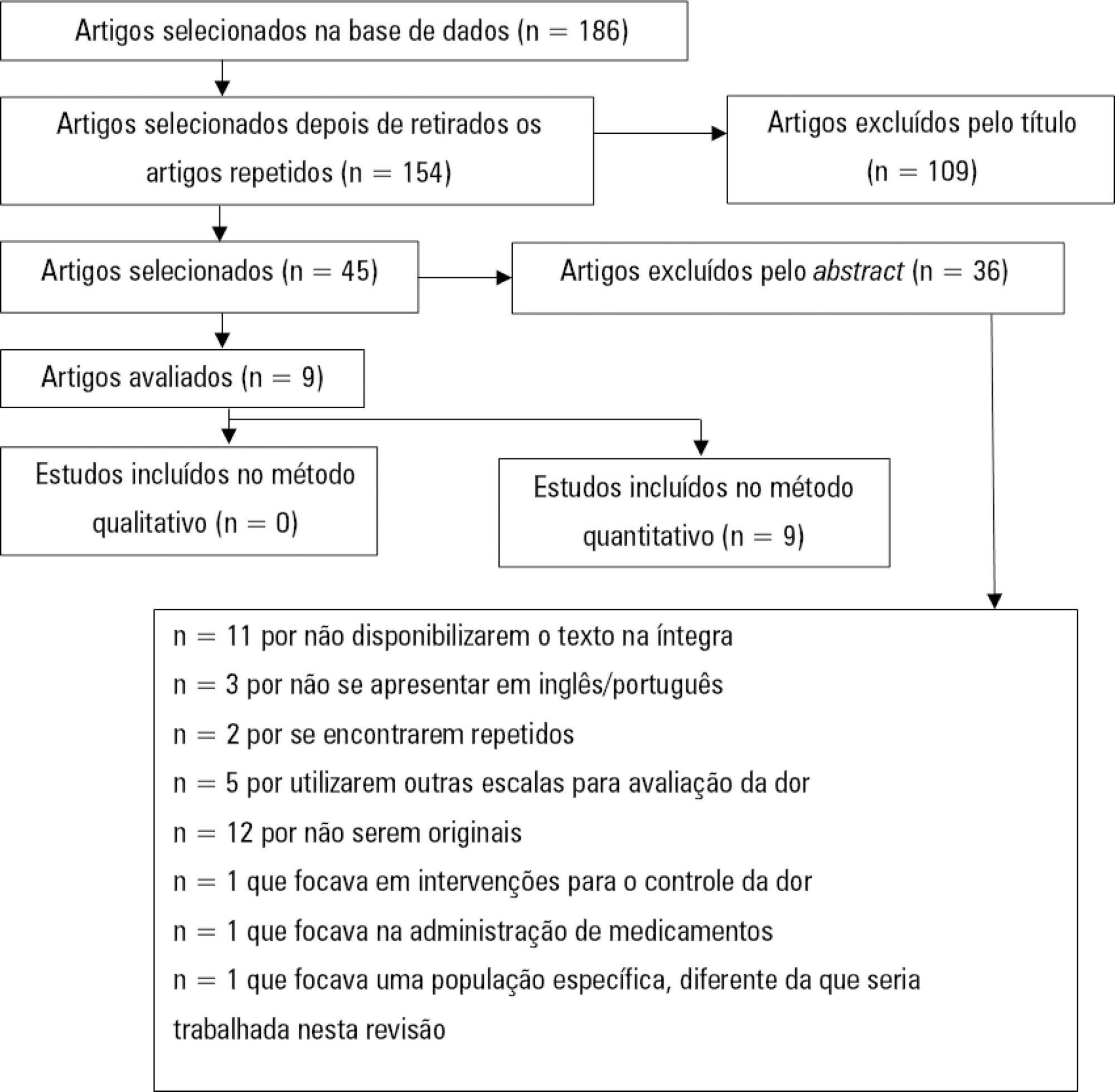
Utilizando a metodologia recomendada pelo Centro Cochrane, foi realizada revisão sistemática da literatura, na base de dados eletrônica EBSCO host (CINAHL Complete, MEDLINE®Complete, Nursing & Allied Health Collection: Comprehensive, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Library, Information Science & Technology Abstracts, MedicLatina). Foram realizadas duas pesquisas com os seguintes termos em inglês no campo de pesquisa: "behavioral pain scale" AND "critical care pain observation tool" AND "behavioral pain scale" OR "critical care pain observation tool". Dois revisores independentes realizaram a avaliação crítica, a extração e a síntese dos dados.
Foram incluídos 15 estudos que evidenciaram que a Behavioral Pain Scale e a Critical Care Pain Observation Tool eram duas escalas válidas e confiáveis para a avaliação da dor em pacientes intubados orotraquealmente e internados em unidade de terapia intensiva. As escalas apresentaram propriedades psicométricas semelhantes, bem como boa confiabilidade.
Ambas as escalas são adequadas para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidade de terapia intensiva, contudo, apresentam limitações em populações específicas como doentes vítimas de trauma, queimados e do foro neurocirurgico. É sugerida a realização de mais estudos sobre o tema e em populações específicas.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):571-581
DOI 10.5935/0103-507X.20190070
Descrever a adequação de duas escalas comportamentais, a Behavioral Pain Scale e a Critical Care Pain Observation Tool, para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidades de terapia intensiva.
Utilizando a metodologia recomendada pelo Centro Cochrane, foi realizada revisão sistemática da literatura, na base de dados eletrônica EBSCO host (CINAHL Complete, MEDLINE®Complete, Nursing & Allied Health Collection: Comprehensive, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Library, Information Science & Technology Abstracts, MedicLatina). Foram realizadas duas pesquisas com os seguintes termos em inglês no campo de pesquisa: "behavioral pain scale" AND "critical care pain observation tool" AND "behavioral pain scale" OR "critical care pain observation tool". Dois revisores independentes realizaram a avaliação crítica, a extração e a síntese dos dados.
Foram incluídos 15 estudos que evidenciaram que a Behavioral Pain Scale e a Critical Care Pain Observation Tool eram duas escalas válidas e confiáveis para a avaliação da dor em pacientes intubados orotraquealmente e internados em unidade de terapia intensiva. As escalas apresentaram propriedades psicométricas semelhantes, bem como boa confiabilidade.
Ambas as escalas são adequadas para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidade de terapia intensiva, contudo, apresentam limitações em populações específicas como doentes vítimas de trauma, queimados e do foro neurocirurgico. É sugerida a realização de mais estudos sobre o tema e em populações específicas.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
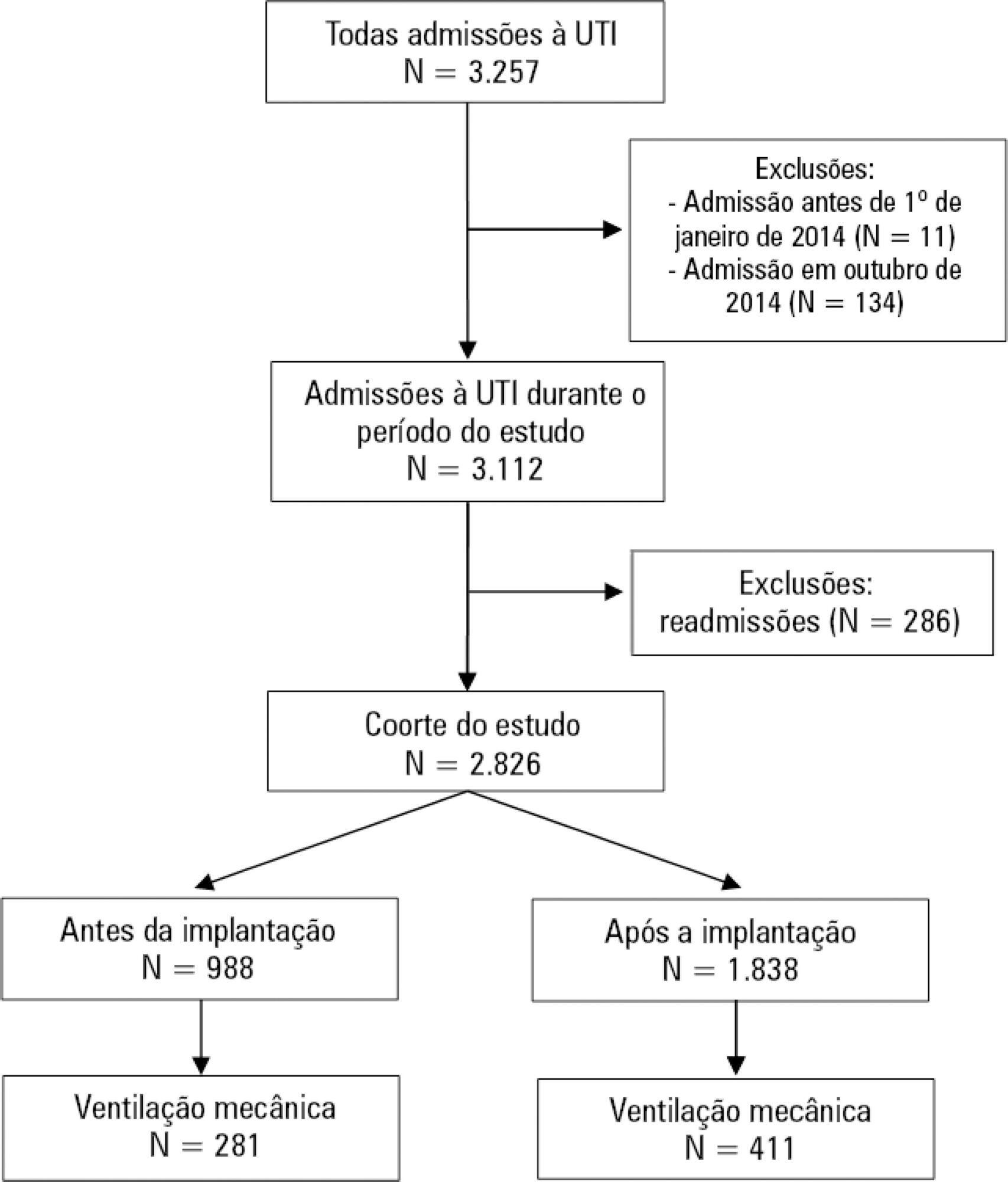
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 - 25; p = 0.002) but substantially decreased in level with the intervention (β = - 128; 95%CI -195 - -62; p = 0.001) and then progressively decreased (β = - 24; 95%CI -35 - -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 - -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 - -0.98; p < 0.001).
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 - 25; p = 0.002) but substantially decreased in level with the intervention (β = - 128; 95%CI -195 - -62; p = 0.001) and then progressively decreased (β = - 24; 95%CI -35 - -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 - -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 - -0.98; p < 0.001).
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):479-486
DOI 10.5935/0103-507X.20180069
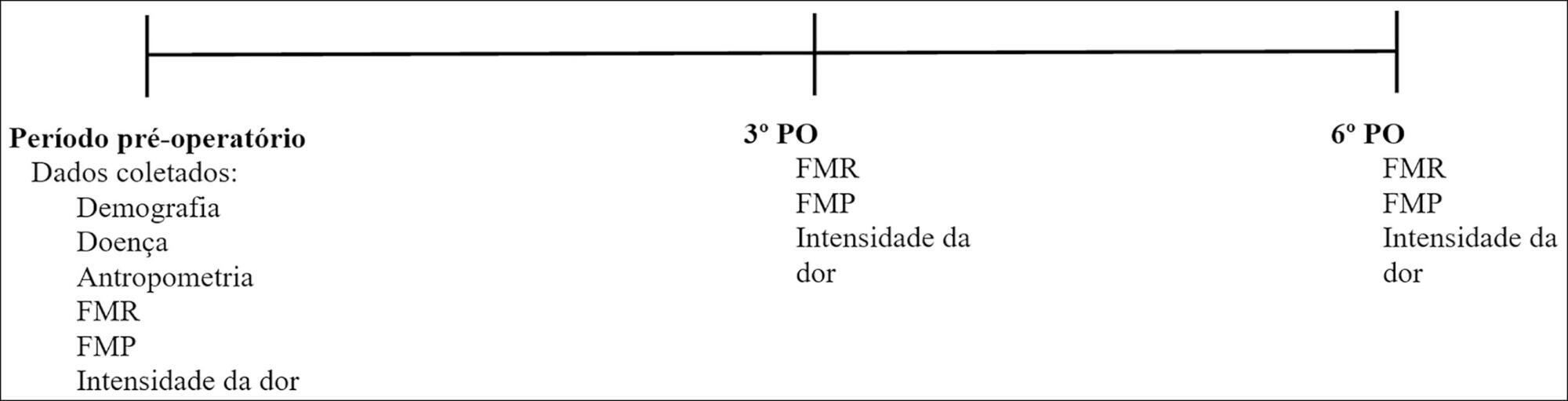
To evaluate respiratory and peripheral muscle strength after cardiac surgery. Additionally, we compared the changes in these variables on the third and sixth postoperative days.
Forty-six patients were recruited, including 17 women and 29 men, with a mean age of 60.50 years (SD = 9.20). Myocardial revascularization surgery was performed in 36 patients, replacement of the aortic valve in 5 patients, and replacement of the mitral valve in 5 patients.
A significant reduction in respiratory and peripheral muscle strength and a significant increase in pain intensity were observed on the third and sixth postoperative days (p < 0.05), except for the variable maximal inspiratory pressure; on the sixth postoperative day, maximal inspiratory pressure values were already similar to the preoperative and predicted values (p > 0.05). There was an association between peripheral muscle strength, specifically between maximal expiratory pressure preoperatively (rs = 0.383; p = 0.009), on the third postoperative day (rs = 0.468; p = 0.001) and on the sixth postoperative day (rs = 0.311; p = 0.037). The effect sizes were consistently moderate-to-large for respiratory muscle strength, the Medical Research Council scale and the visual analog scale, in particular between preoperative assessment and the sixth postoperative day.
There is a decrease in respiratory and peripheral muscle strength after cardiac surgery. In addition, maximal expiratory pressure is the variable that is most associated with peripheral muscle strength. These variables, especially respiratory and peripheral muscle strength, should be considered by professionals working in the intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):479-486
DOI 10.5935/0103-507X.20180069
To evaluate respiratory and peripheral muscle strength after cardiac surgery. Additionally, we compared the changes in these variables on the third and sixth postoperative days.
Forty-six patients were recruited, including 17 women and 29 men, with a mean age of 60.50 years (SD = 9.20). Myocardial revascularization surgery was performed in 36 patients, replacement of the aortic valve in 5 patients, and replacement of the mitral valve in 5 patients.
A significant reduction in respiratory and peripheral muscle strength and a significant increase in pain intensity were observed on the third and sixth postoperative days (p < 0.05), except for the variable maximal inspiratory pressure; on the sixth postoperative day, maximal inspiratory pressure values were already similar to the preoperative and predicted values (p > 0.05). There was an association between peripheral muscle strength, specifically between maximal expiratory pressure preoperatively (rs = 0.383; p = 0.009), on the third postoperative day (rs = 0.468; p = 0.001) and on the sixth postoperative day (rs = 0.311; p = 0.037). The effect sizes were consistently moderate-to-large for respiratory muscle strength, the Medical Research Council scale and the visual analog scale, in particular between preoperative assessment and the sixth postoperative day.
There is a decrease in respiratory and peripheral muscle strength after cardiac surgery. In addition, maximal expiratory pressure is the variable that is most associated with peripheral muscle strength. These variables, especially respiratory and peripheral muscle strength, should be considered by professionals working in the intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
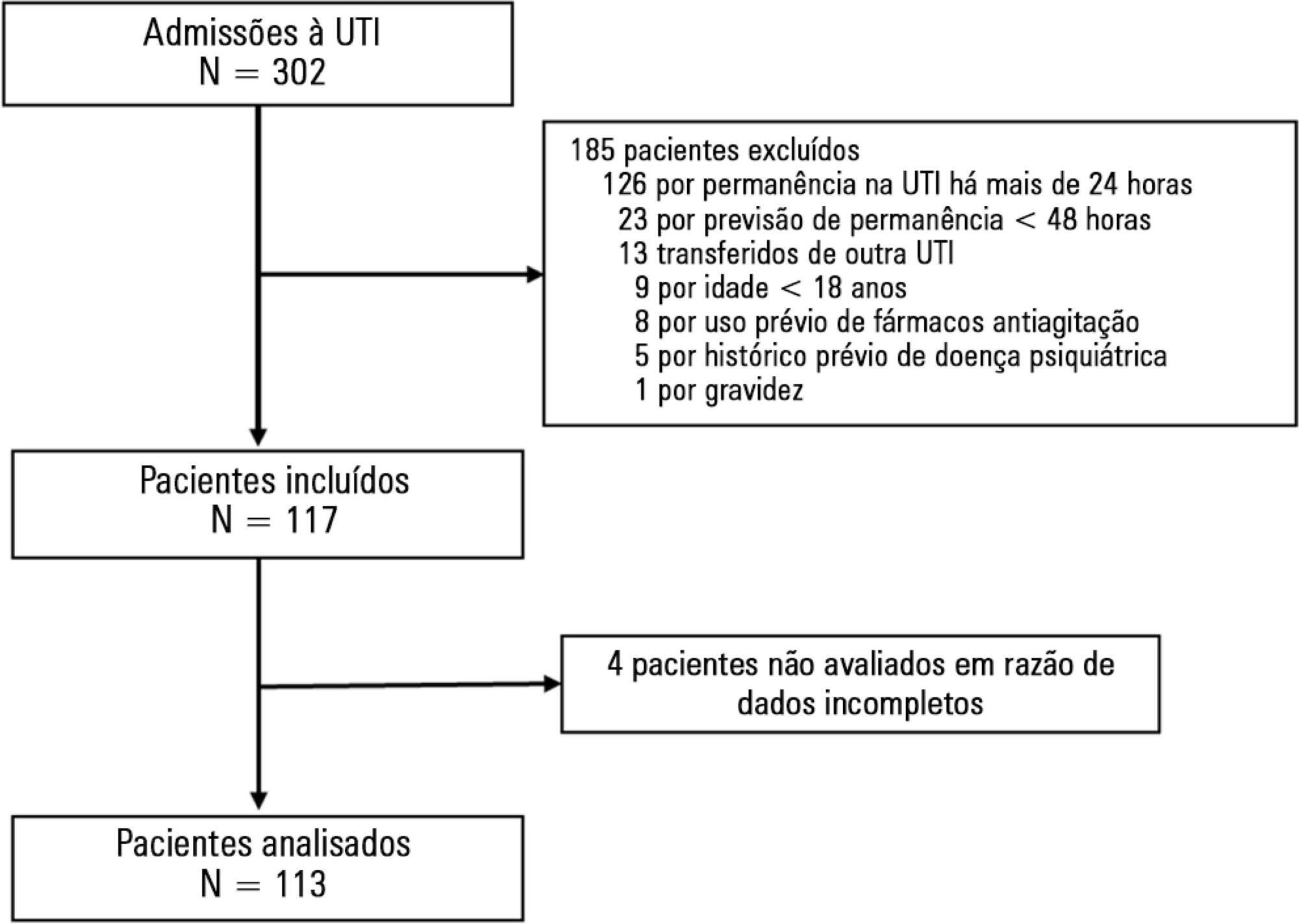
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 - 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):413-419
DOI 10.5935/0103-507X.20160074
To evaluate the incidence of agitation in the first 7 days after intensive care unit admission, its risk factors and its associations with clinical outcomes.
This single-center prospective cohort study included all patients older than 18 years with a predicted stay > 48 hours within the first 24 hours of intensive care unit admission. Agitation was defined as a Richmond Agitation Sedation Scale score ≥ +2, an episode of agitation or the use of a specific medication recorded in patient charts.
Agitation occurred in 31.8% of the 113 patients. Multivariate analysis showed that delirium [OR = 24.14; CI95% 5.15 - 113.14; p < 0.001], moderate or severe pain [OR = 5.74; CI95% 1.73 - 19.10; p = 0.004], mechanical ventilation [OR = 10.14; CI95% 2.93 - 35.10; p < 0.001], and smoking habits [OR = 4.49; CI95% 1.33 - 15.17; p = 0.015] were independent factors for agitation, while hyperlactatemia was associated with a lower risk [OR = 0.169; CI95% 0.04 - 0.77; p = 0.021]. Agitated patients had fewer mechanical ventilation-free days at day 7 (p = 0.003).
The incidence of agitation in the first 7 days after admission to the intensive care unit was high. Delirium, moderate/severe pain, mechanical ventilation, and smoking habits were independent risk factors. Agitated patients had fewer ventilator-free days in the first 7 days.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Although low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units' invasive procedures, therefore contributing to pain reduction
Abstract
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Although low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units' invasive procedures, therefore contributing to pain reduction
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)