
You searched for:"Carlos Eduardo Brandão"
We found (2) results for your search.-
Original Article
Mechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
- Fábio Holanda Lacerda
 ,
, - Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte, [ … ],
- Bruno Adler Maccagnan Pinheiro Besen
Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
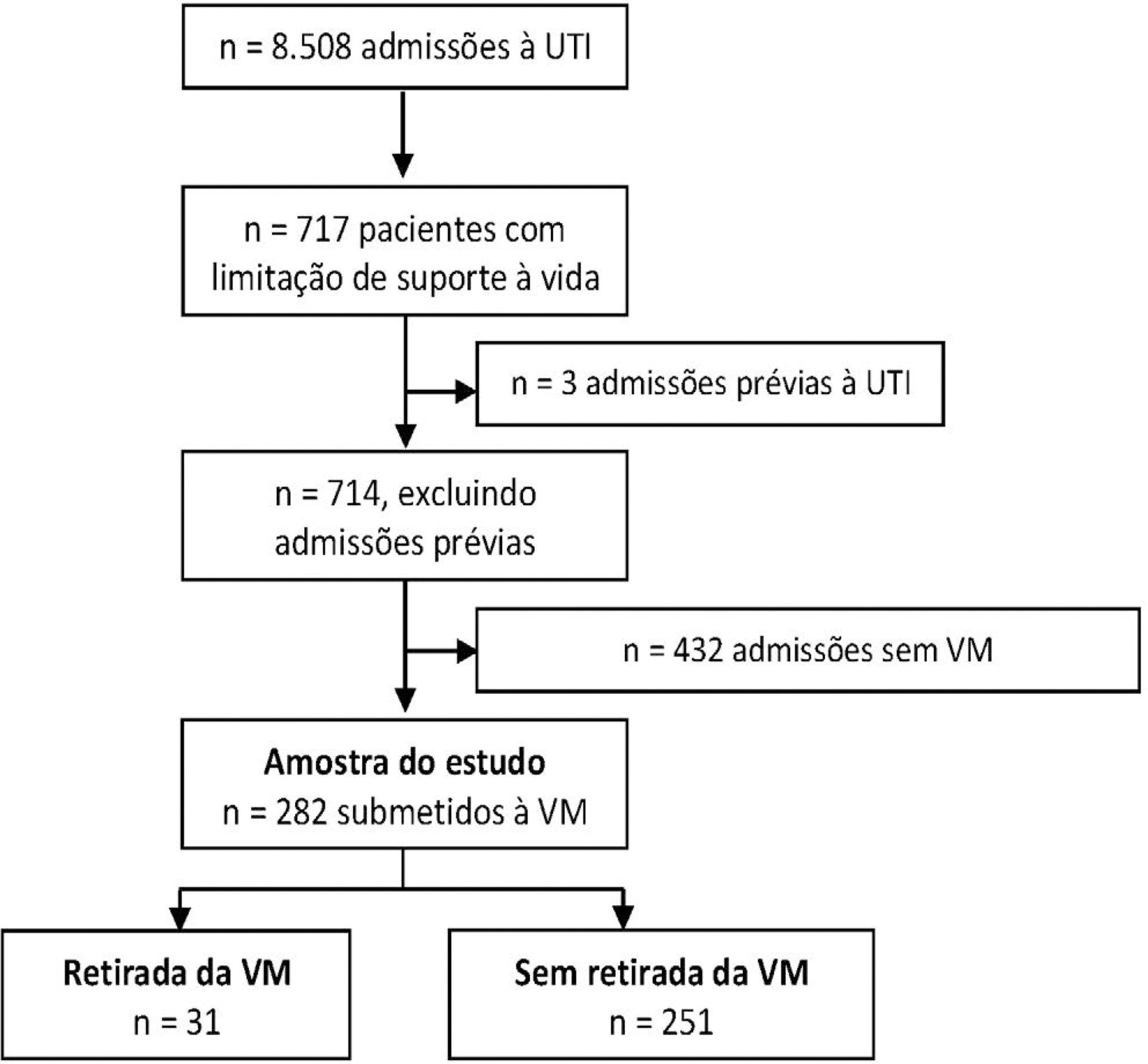
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
Views1

Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
- Fábio Holanda Lacerda
-
Original Articles
Pain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza, [ … ],
- Lucas Fernandes de Oliveira
Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
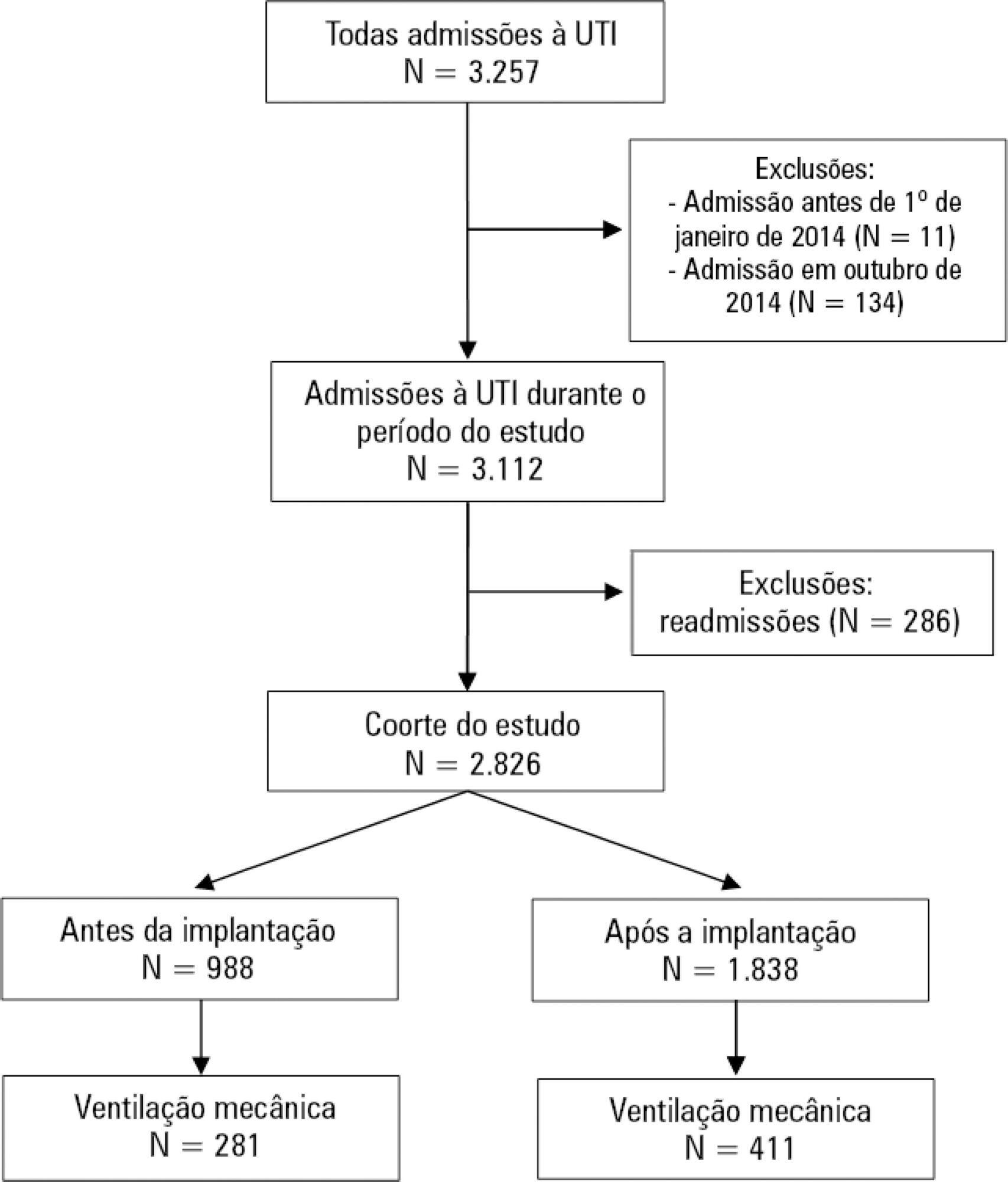
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Views1Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
- Bruno Adler Maccagnan Pinheiro Besen
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis