
You searched for:"Antonio Paulo Nassar Júnior"
We found (15) results for your search.-
Review
High-value care for critically ill oncohematological patients: what do we know thus far?
- Fernanda Chohfi Atallah
 ,
, - Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola , [ … ],
- Thiago Gomes Romano
Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee moreViews7

Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee more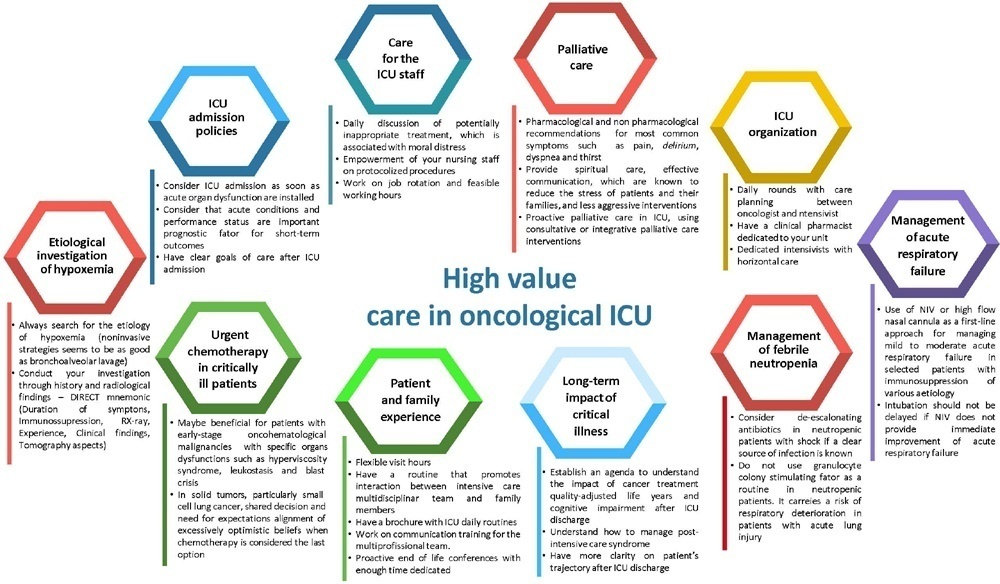
- Fernanda Chohfi Atallah
-
Letter to the Editor
Patient-level costs of central line-associated bloodstream infections caused by multidrug-resistant microorganisms in a public intensive care unit in Brazil: a retrospective cohort study
- Antonio Paulo Nassar Júnior ,
- Isabella Lott Bezerra ,
- Daniel Tavares Malheiro ,
- Maria Dolores Montoya Diaz ,
- Guilherme Paula Pinto Schettino , [ … ],
- Adriano José Pereira
Abstract
Letter to the EditorPatient-level costs of central line-associated bloodstream infections caused by multidrug-resistant microorganisms in a public intensive care unit in Brazil: a retrospective cohort study
Rev Bras Ter Intensiva. 2022;34(4):529-533
DOI 10.5935/0103-507X.20220313-en
- Antonio Paulo Nassar Júnior ,
- Isabella Lott Bezerra ,
- Daniel Tavares Malheiro ,
- Maria Dolores Montoya Diaz ,
- Guilherme Paula Pinto Schettino ,
- Adriano José Pereira
Views1TO THE EDITOR, Hospital-acquired infections (HAIs) are a major threat to patients and health care systems.() Hospital-acquired infections are associated with increased mortality and prolonged hospital length of stay.() However, it is not clear whether HAIs caused by multidrug-resistant (MDR) pathogens acquired in intensive care units (ICUs) are associated with increased costs when compared to […]See moreViews1Abstract
Letter to the EditorPatient-level costs of central line-associated bloodstream infections caused by multidrug-resistant microorganisms in a public intensive care unit in Brazil: a retrospective cohort study
Rev Bras Ter Intensiva. 2022;34(4):529-533
DOI 10.5935/0103-507X.20220313-en
- Antonio Paulo Nassar Júnior ,
- Isabella Lott Bezerra ,
- Daniel Tavares Malheiro ,
- Maria Dolores Montoya Diaz ,
- Guilherme Paula Pinto Schettino ,
- Adriano José Pereira
Views1TO THE EDITOR, Hospital-acquired infections (HAIs) are a major threat to patients and health care systems.() Hospital-acquired infections are associated with increased mortality and prolonged hospital length of stay.() However, it is not clear whether HAIs caused by multidrug-resistant (MDR) pathogens acquired in intensive care units (ICUs) are associated with increased costs when compared to […]See more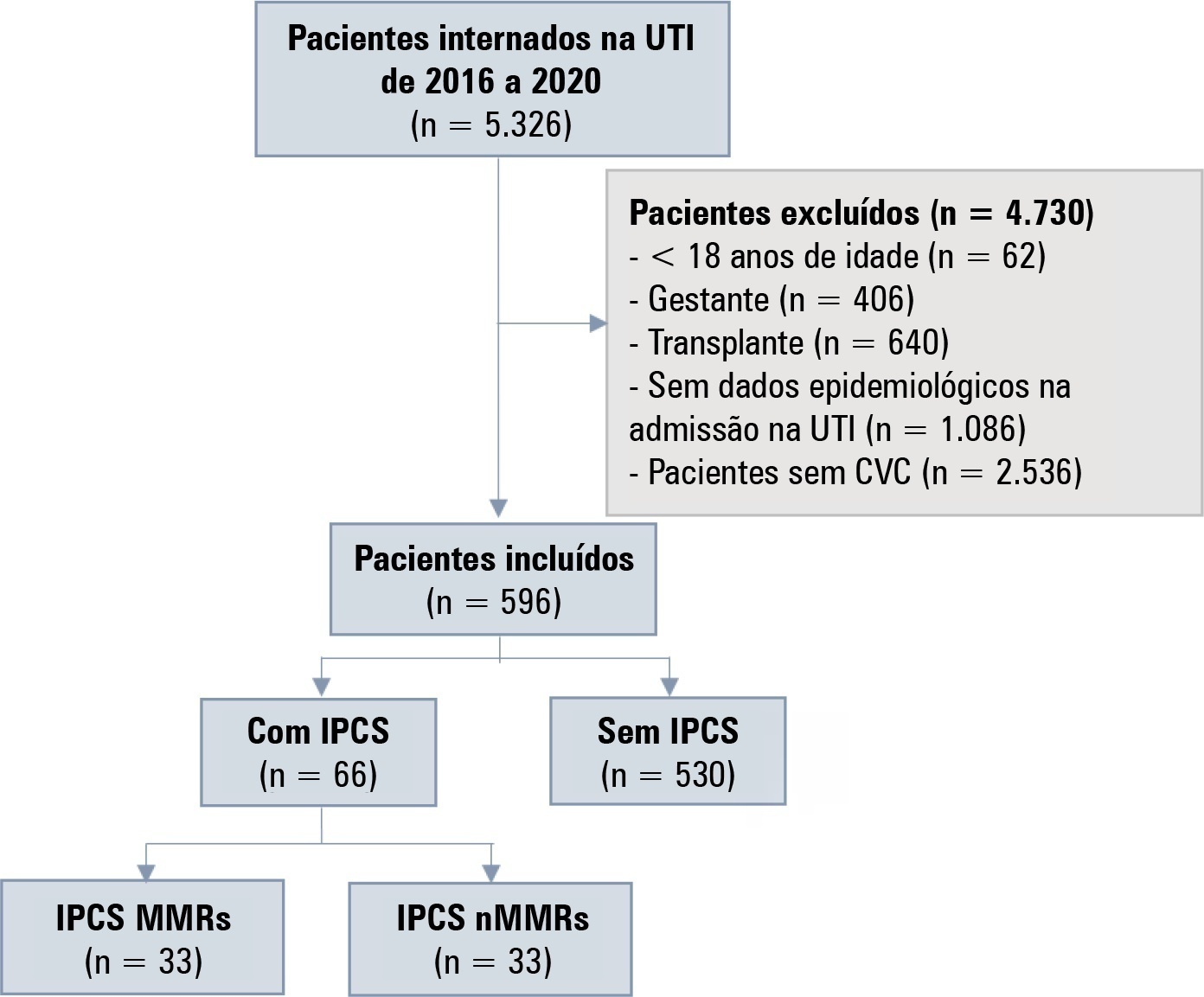
- Antonio Paulo Nassar Júnior
-
Original Article
Comparison of the accuracy of residents, senior physicians and surrogate decision-makers for predicting hospital mortality of critically ill patients
- Bárbara Vieira Carneiro ,
- Lucas Lonardoni Crozatti ,
- Pedro Vitale Mendes ,
- Antonio Paulo Nassar Júnior ,
- Leandro Utino Taniguchi
Abstract
Original ArticleComparison of the accuracy of residents, senior physicians and surrogate decision-makers for predicting hospital mortality of critically ill patients
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
- Bárbara Vieira Carneiro ,
- Lucas Lonardoni Crozatti ,
- Pedro Vitale Mendes ,
- Antonio Paulo Nassar Júnior ,
- Leandro Utino Taniguchi
Views2ABSTRACT
Objective:
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
Methods:
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
Results:
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Conclusion:
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Keywords:Critical illnessDecision MakingDelivery of health careHospitalizationIntensive care unitsInternship and residencyMortalityPrognosisSee moreViews2Abstract
Original ArticleComparison of the accuracy of residents, senior physicians and surrogate decision-makers for predicting hospital mortality of critically ill patients
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
- Bárbara Vieira Carneiro ,
- Lucas Lonardoni Crozatti ,
- Pedro Vitale Mendes ,
- Antonio Paulo Nassar Júnior ,
- Leandro Utino Taniguchi
Views2ABSTRACT
Objective:
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
Methods:
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
Results:
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Conclusion:
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Keywords:Critical illnessDecision MakingDelivery of health careHospitalizationIntensive care unitsInternship and residencyMortalityPrognosisSee more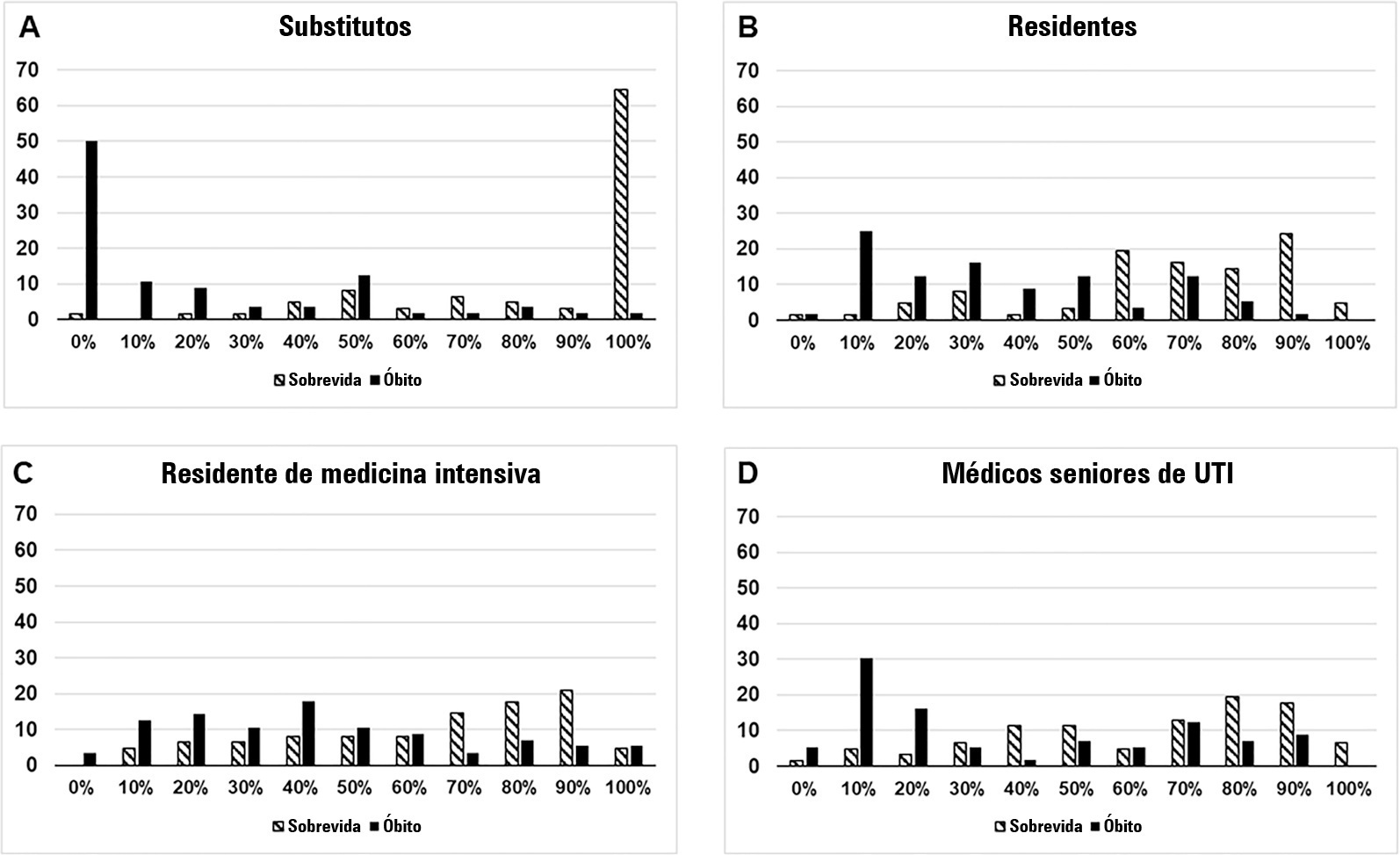
- Bárbara Vieira Carneiro
-
Original Article
Performance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
Abstract
Original ArticlePerformance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
DOI 10.5935/0103-507X.20210038
Views1See moreABSTRACT
Objective:
To evaluate how performance status impairment and acute organ dysfunction influence hospital mortality in critically ill patients with cancer who were admitted with suspected sepsis.
Methods:
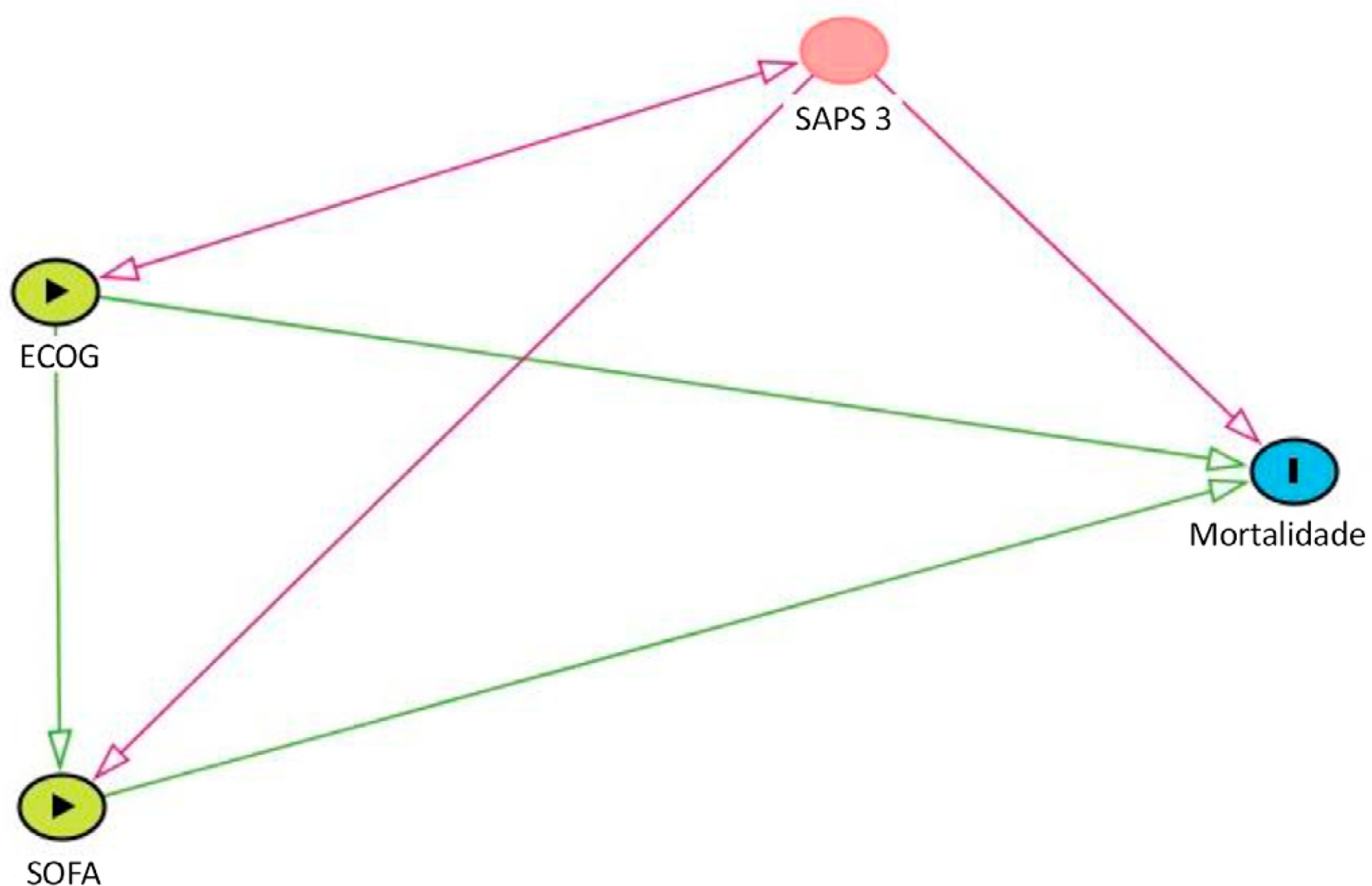
Data were obtained from a retrospective cohort of patients, admitted to an intensive care unit, with cancer and with a suspected infection who received parenteral antibiotics and underwent the collection of bodily fluid samples. We used logistic regression with hospital mortality as the outcome and the Sequential Organ Failure Assessment score, Eastern Cooperative Oncology Group status, and their interactions as predictors.
Results:
Of 450 patients included, 265 (58.9%) died in the hospital. For patients admitted to the intensive care unit with lower Sequential Organ Failure Assessment (≤ 6), performance status impairment influenced the in-hospital mortality, which was 32% among those with no and minor performance status impairment and 52% among those with moderate and severe performance status impairment, p < 0.01. However, for those with higher Sequential Organ Failure Assessment (> 6), performance status impairment did not influence the in-hospital mortality (73% among those with no and minor impairment and 84% among those with moderate and severe impairment; p = 0.1).
Conclusion:
Performance status impairment seems to influence hospital mortality in critically ill cancer patients with suspected sepsis when they have less severe acute organ dysfunction at the time of intensive care unit admission.
Views1Abstract
Original ArticlePerformance status and acute organ dysfunction influence hospital mortality in critically ill patients with cancer and suspected infection: a retrospective cohort analysis
Rev Bras Ter Intensiva. 2021;33(2):298-303
DOI 10.5935/0103-507X.20210038
Views1See moreABSTRACT
Objective:
To evaluate how performance status impairment and acute organ dysfunction influence hospital mortality in critically ill patients with cancer who were admitted with suspected sepsis.
Methods:
Data were obtained from a retrospective cohort of patients, admitted to an intensive care unit, with cancer and with a suspected infection who received parenteral antibiotics and underwent the collection of bodily fluid samples. We used logistic regression with hospital mortality as the outcome and the Sequential Organ Failure Assessment score, Eastern Cooperative Oncology Group status, and their interactions as predictors.
Results:
Of 450 patients included, 265 (58.9%) died in the hospital. For patients admitted to the intensive care unit with lower Sequential Organ Failure Assessment (≤ 6), performance status impairment influenced the in-hospital mortality, which was 32% among those with no and minor performance status impairment and 52% among those with moderate and severe performance status impairment, p < 0.01. However, for those with higher Sequential Organ Failure Assessment (> 6), performance status impairment did not influence the in-hospital mortality (73% among those with no and minor impairment and 84% among those with moderate and severe impairment; p = 0.1).
Conclusion:
Performance status impairment seems to influence hospital mortality in critically ill cancer patients with suspected sepsis when they have less severe acute organ dysfunction at the time of intensive care unit admission.
-
Original Article
Nursing workload associated with the frequency of multidisciplinary rounds: a cross-sectional study
Rev Bras Ter Intensiva. 2021;33(1):82-87
Abstract
Original ArticleNursing workload associated with the frequency of multidisciplinary rounds: a cross-sectional study
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
Views1See moreAbstract
Objective:
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
Methods:
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
Results:
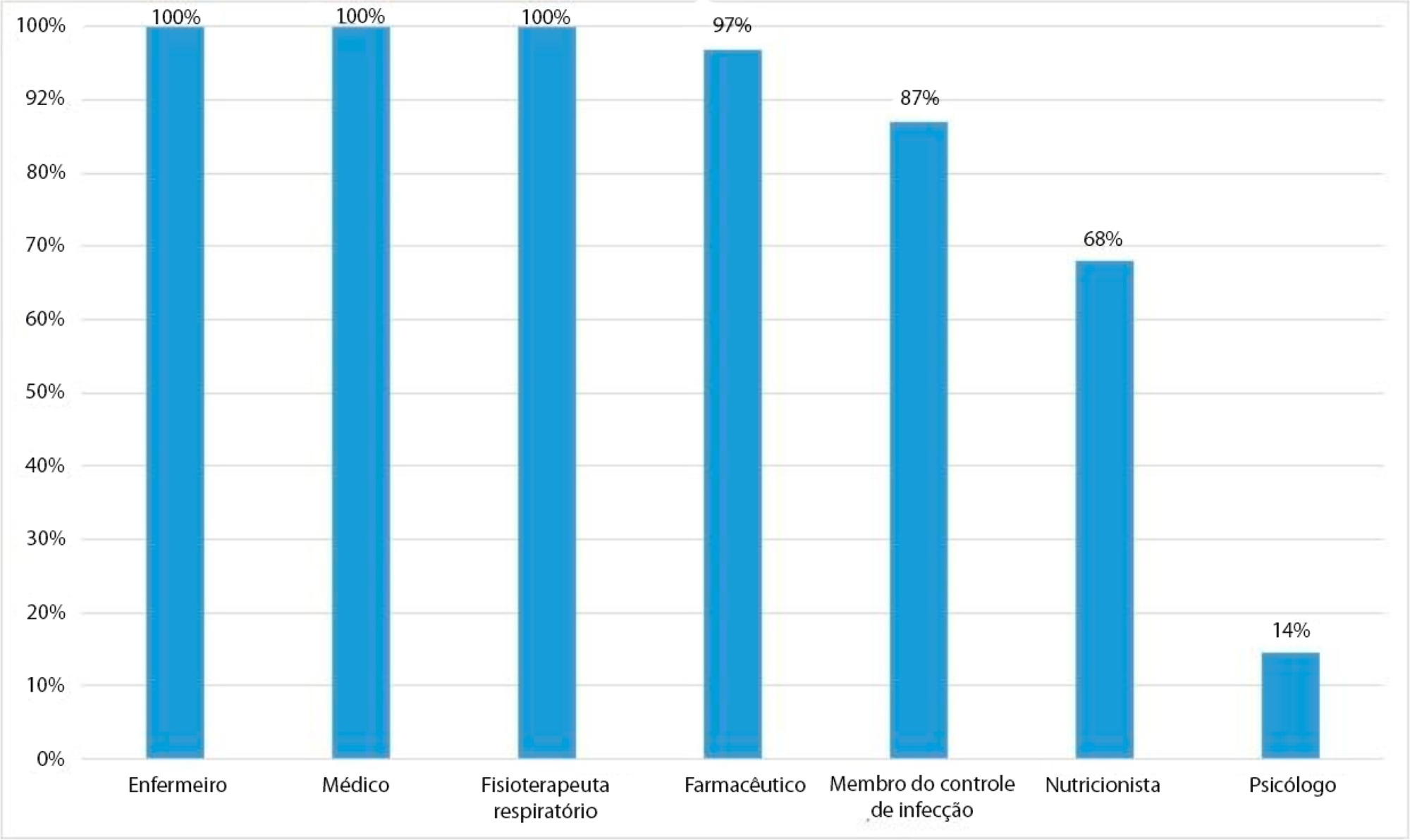
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 – 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Conclusion:
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
Views1Abstract
Original ArticleNursing workload associated with the frequency of multidisciplinary rounds: a cross-sectional study
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
Views1See moreAbstract
Objective:
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
Methods:
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
Results:
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 – 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Conclusion:
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
-
Original Article
Characteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes, [ … ],
- Antonio Paulo Nassar Júnior
Abstract
Original ArticleCharacteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes,
- Pedro Caruso,
- Antonio Paulo Nassar Júnior
Views0ABSTRACT
Objective:
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
Methods:
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Results:
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 – 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 – 15.05) were independently associated with in-hospital mortality.
Conclusion:
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Keywords:Critical careCritical care outcomesepidemiologyEsophageal neoplasmsMortalityPrognosisRespiration, artificialSee moreViews0Abstract
Original ArticleCharacteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes,
- Pedro Caruso,
- Antonio Paulo Nassar Júnior
Views0ABSTRACT
Objective:
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
Methods:
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Results:
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 – 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 – 15.05) were independently associated with in-hospital mortality.
Conclusion:
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Keywords:Critical careCritical care outcomesepidemiologyEsophageal neoplasmsMortalityPrognosisRespiration, artificialSee more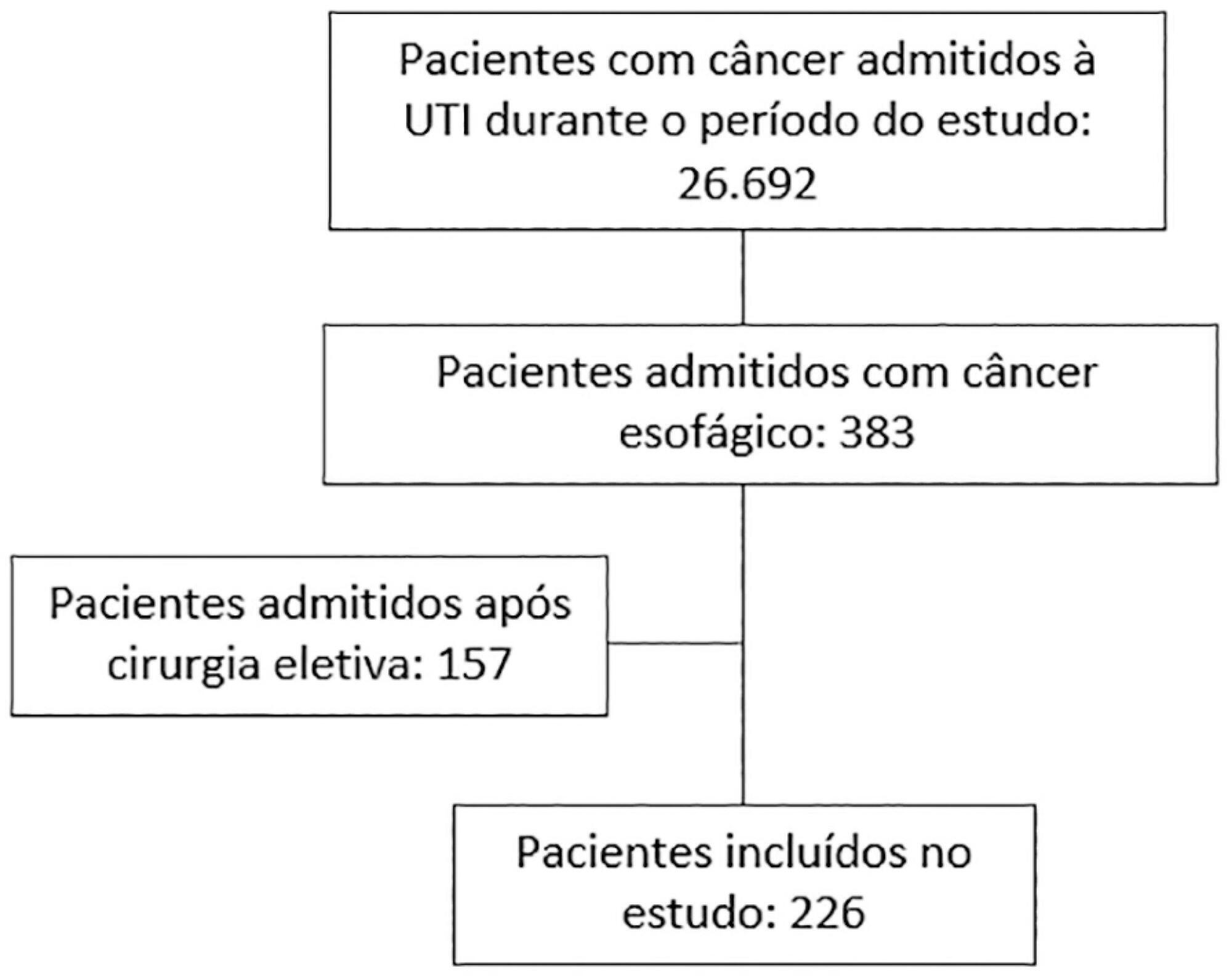
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more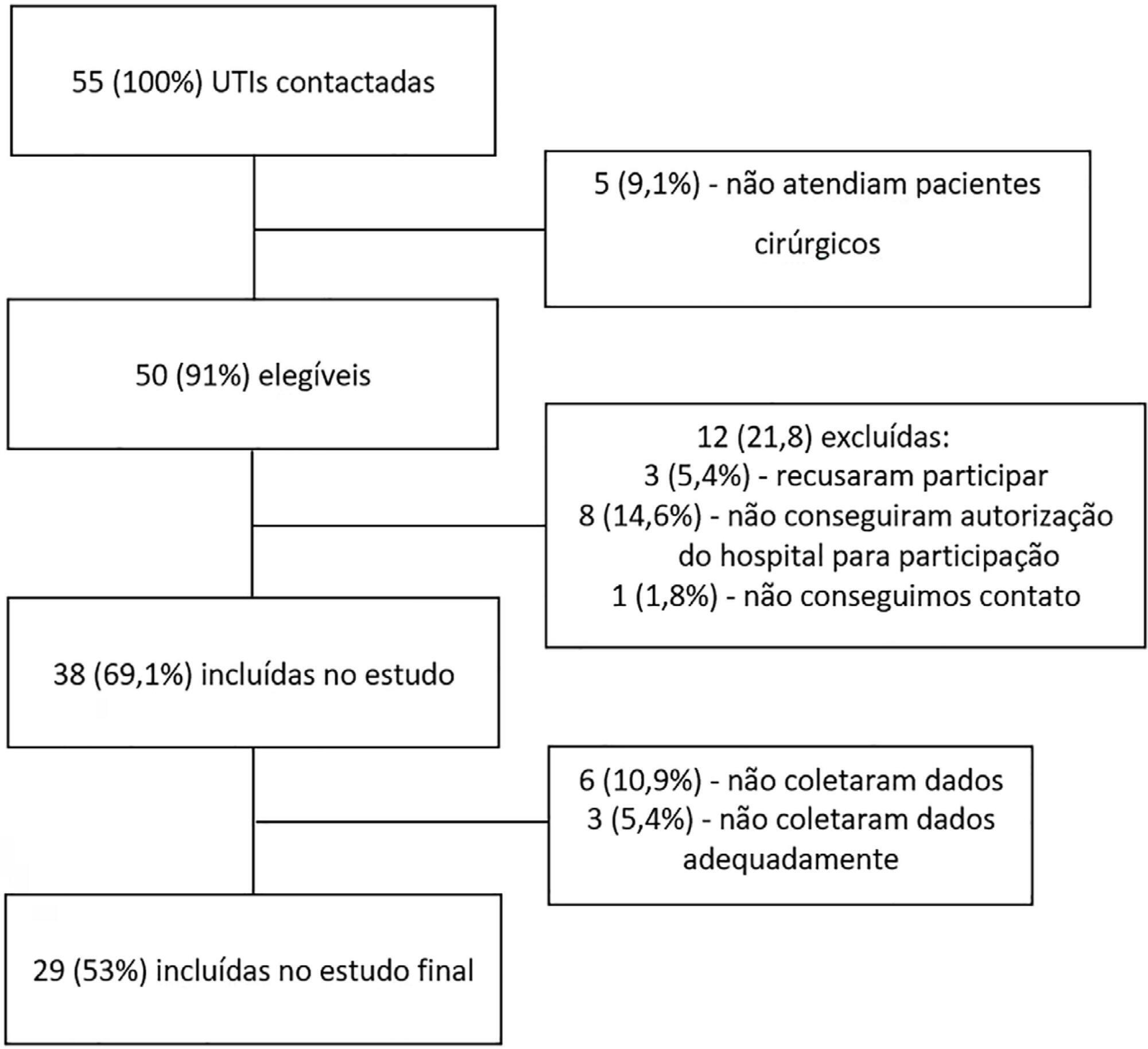
- João Manoel Silva Júnior
-
Original Articles
Pain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza, [ … ],
- Lucas Fernandes de Oliveira
Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
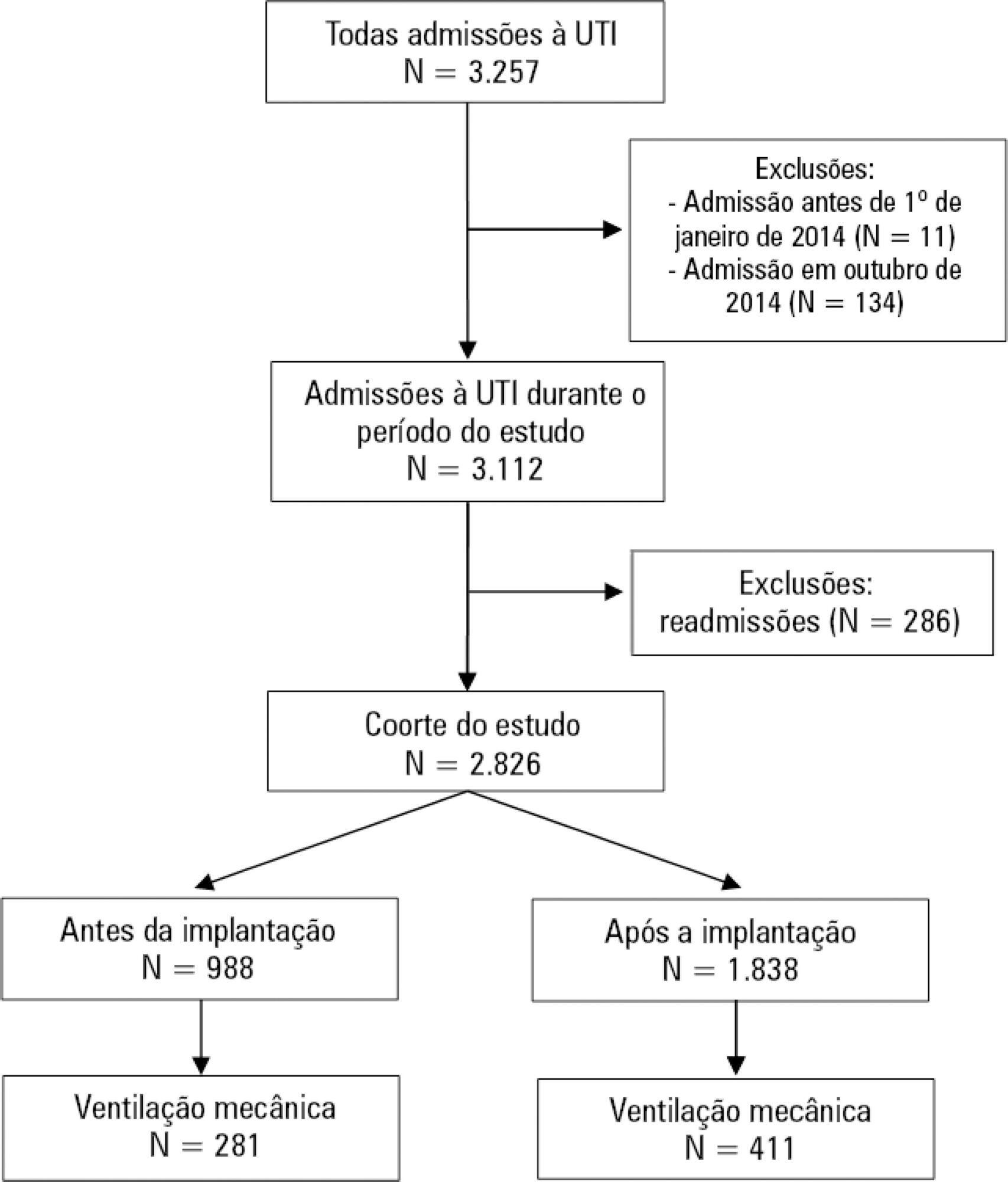
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Views1Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
- Bruno Adler Maccagnan Pinheiro Besen
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis