Hospital costs Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
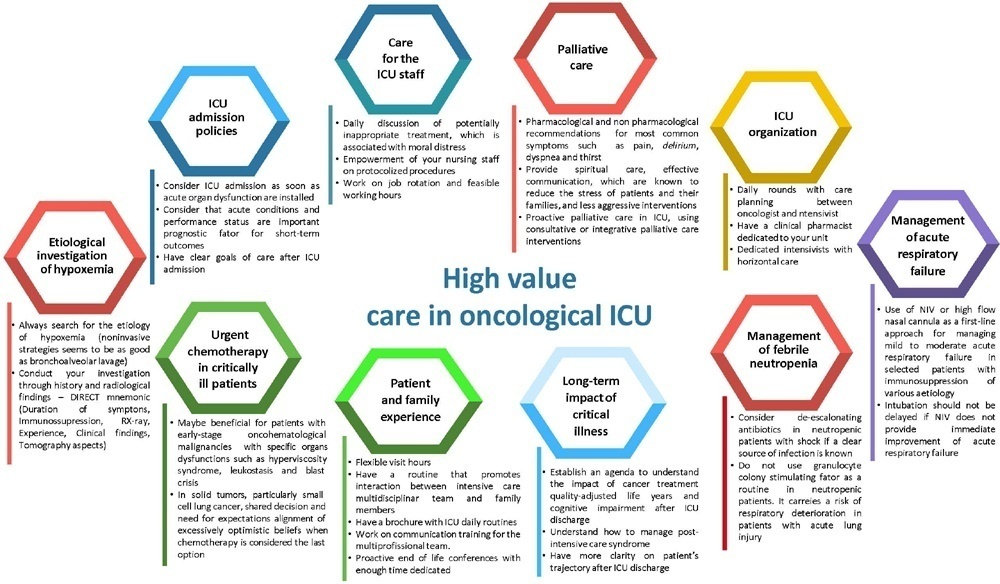
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):357-361
DOI 10.1590/S0103-507X2012000400011
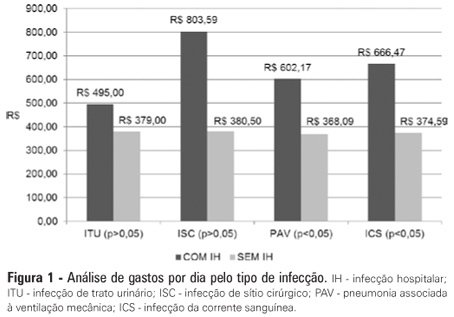
OBJECTIVE: Infections in intensive care units are often associated with a high morbidity and mortality in addition to high costs. An analysis of these aspects can assist in optimizing the allocation of relevant financial resources. METHODS: This retrospective study analyzed the hospital administration and quality in intensive care medical databases [Sistema de Gestão Hospitalar (SGH)] and RM Janus®. A cost analysis was performed by evaluating the medical products and materials used in direct medical care. The costs are reported in the Brazilian national currency (Real). The cost and length of stay analyses were performed for all the costs studied. The median was used to determine the costs involved. Costs were also adjusted by the patients' length of stay in the intensive care unit. RESULTS: In total, 974 individuals were analyzed, of which 51% were male, and the mean age was 57±18.24 years. There were 87 patients (8.9%) identified who had nosocomial infections associated with the intensive care unit. The median cost per admission and the length of stay for all the patients sampled were R$1.257,53 and 3 days, respectively. Compared to the patients without an infection, the patients with an infection had longer hospital stays (15 [11-25] versus 3 [2-6] days, p<0.01), increased costs per patient in the intensive care unit (median R$9.763,78 [5445.64 - 18,007.90] versus R$1.093,94 [416.14 - 2755.90], p<0.01) and increased costs per day of hospitalization in the intensive care unit (R$618,00 [407.81 - 838.69] versus R$359,00 [174.59 - 719.12], p<0.01). CONCLUSION: Nosocomial infections associated with the intensive care unit were determinants of increased costs and longer hospital stays. However, the study design did not allow us to evaluate specific aspects of cause and effect.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):357-361
DOI 10.1590/S0103-507X2012000400011
OBJECTIVE: Infections in intensive care units are often associated with a high morbidity and mortality in addition to high costs. An analysis of these aspects can assist in optimizing the allocation of relevant financial resources. METHODS: This retrospective study analyzed the hospital administration and quality in intensive care medical databases [Sistema de Gestão Hospitalar (SGH)] and RM Janus®. A cost analysis was performed by evaluating the medical products and materials used in direct medical care. The costs are reported in the Brazilian national currency (Real). The cost and length of stay analyses were performed for all the costs studied. The median was used to determine the costs involved. Costs were also adjusted by the patients' length of stay in the intensive care unit. RESULTS: In total, 974 individuals were analyzed, of which 51% were male, and the mean age was 57±18.24 years. There were 87 patients (8.9%) identified who had nosocomial infections associated with the intensive care unit. The median cost per admission and the length of stay for all the patients sampled were R$1.257,53 and 3 days, respectively. Compared to the patients without an infection, the patients with an infection had longer hospital stays (15 [11-25] versus 3 [2-6] days, p<0.01), increased costs per patient in the intensive care unit (median R$9.763,78 [5445.64 - 18,007.90] versus R$1.093,94 [416.14 - 2755.90], p<0.01) and increased costs per day of hospitalization in the intensive care unit (R$618,00 [407.81 - 838.69] versus R$359,00 [174.59 - 719.12], p<0.01). CONCLUSION: Nosocomial infections associated with the intensive care unit were determinants of increased costs and longer hospital stays. However, the study design did not allow us to evaluate specific aspects of cause and effect.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)