
You searched for:"Thiago Gomes Romano"
We found (7) results for your search.-
Review
High-value care for critically ill oncohematological patients: what do we know thus far?
- Fernanda Chohfi Atallah
 ,
, - Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola , [ … ],
- Thiago Gomes Romano
Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee moreViews7

Abstract
ReviewHigh-value care for critically ill oncohematological patients: what do we know thus far?
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
- Fernanda Chohfi Atallah ,
- Pedro Caruso ,
- Antonio Paulo Nassar Junior ,
- Andre Peretti Torelly ,
- Cristina Prata Amendola ,
- Jorge Ibrain Figueira Salluh ,
- Thiago Gomes Romano
Views7ABSTRACT
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Keywords:Cost of illnessCritical illnessHospital costsIntensive care unitsLow-value careNeoplasmsPatient care managementSee more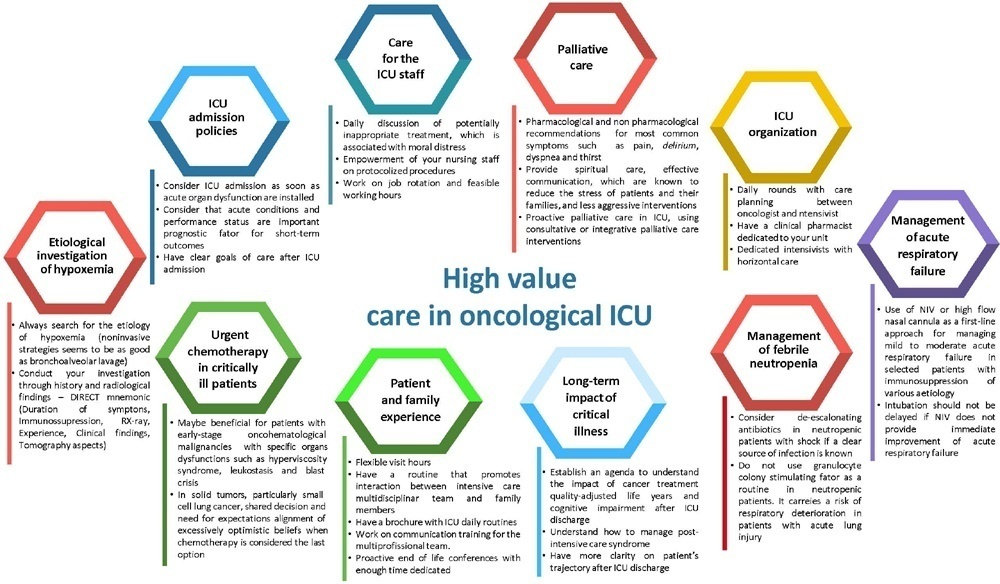
- Fernanda Chohfi Atallah
-
Original Article
IMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee moreViews2Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee more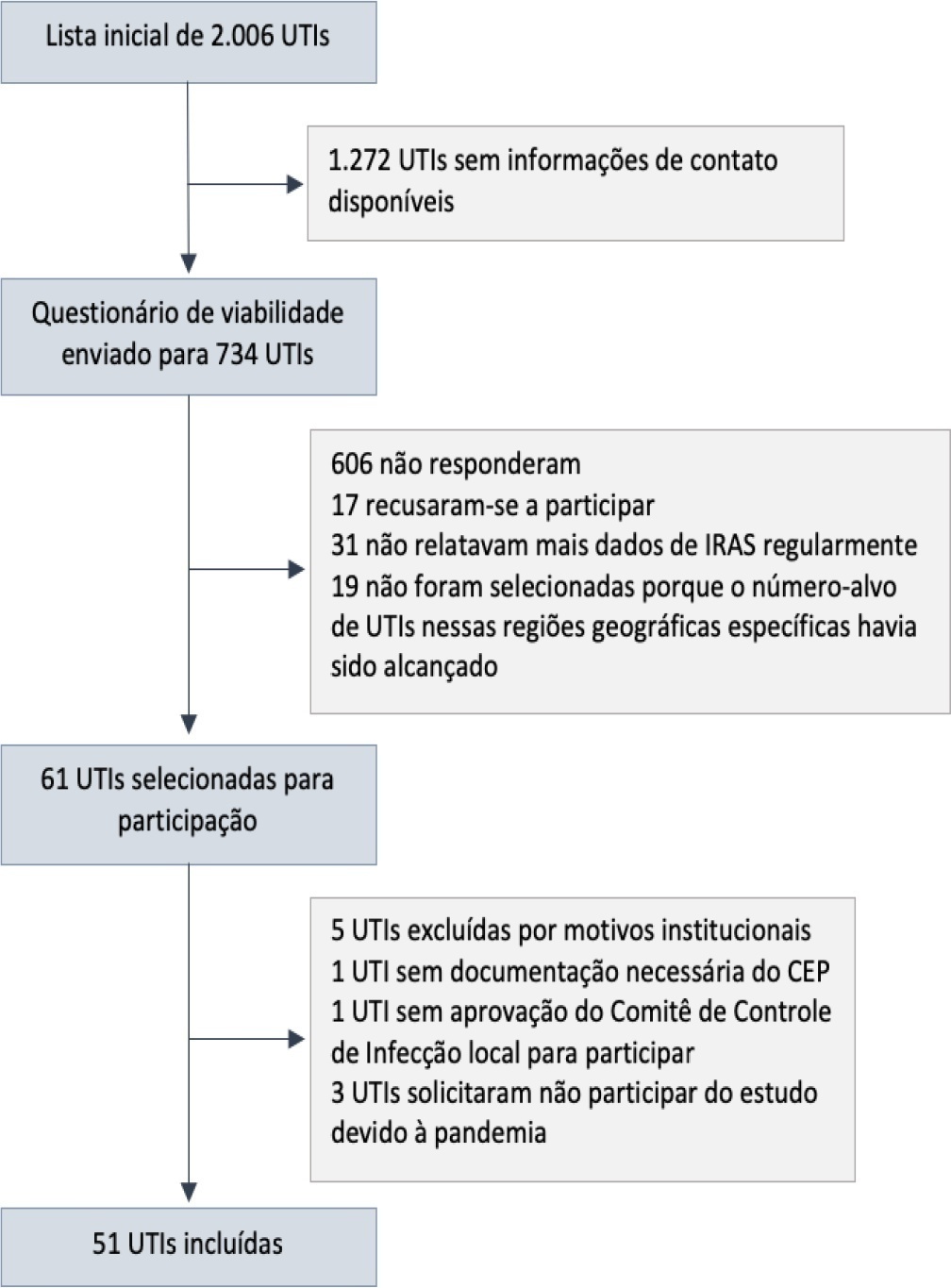
- Bruno M Tomazini
-
Original Article
Oxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
Abstract
Original ArticleOxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
Views0ABSTRACT
Objective:
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Methods:
Mathematical modeling approach with hypothetical scenarios using computer simulation.
Results:
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Conclusion:
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive Care UnitMathematical modelmechanical ventilationrespiratory failureSee moreViews0Abstract
Original ArticleOxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
Views0ABSTRACT
Objective:
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Methods:
Mathematical modeling approach with hypothetical scenarios using computer simulation.
Results:
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Conclusion:
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive Care UnitMathematical modelmechanical ventilationrespiratory failureSee more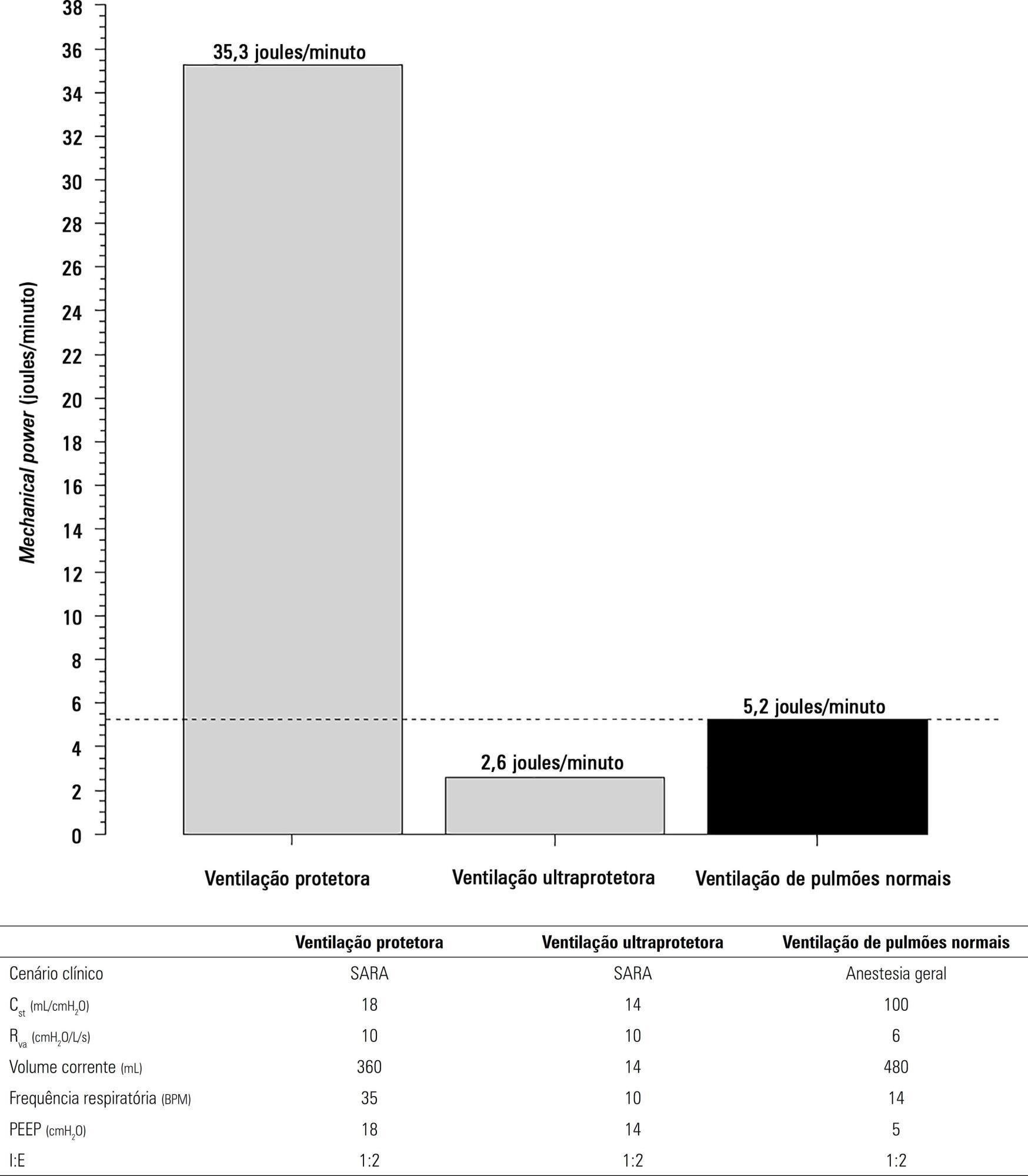
-
Original Article
Characterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
Abstract
Original ArticleCharacterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
Views0ABSTRACT
Objective:
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
Methods:
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
Results:
From 2011 to 2017, 18 patients aged 29 (25 – 31) years with a SAPS 3 of 84 (68 – 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 – 82) km was traveled on each rescue mission during a period of 360 (308 – 431) min. A median of one (0 – 2) nurse, three (2 – 3) physicians, and one (0 – 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Conclusions:
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Keywords:artificial respirationCritical illnessExtracorporeal membrane oxygenationIntensive care unitsRespiratory insufficiencyTransportation of patientsSee moreViews0Abstract
Original ArticleCharacterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
Views0ABSTRACT
Objective:
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
Methods:
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
Results:
From 2011 to 2017, 18 patients aged 29 (25 – 31) years with a SAPS 3 of 84 (68 – 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 – 82) km was traveled on each rescue mission during a period of 360 (308 – 431) min. A median of one (0 – 2) nurse, three (2 – 3) physicians, and one (0 – 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Conclusions:
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Keywords:artificial respirationCritical illnessExtracorporeal membrane oxygenationIntensive care unitsRespiratory insufficiencyTransportation of patientsSee more -
Original Article
Metabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
Abstract
Original ArticleMetabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Views0ABSTRACT
Objective:
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
Methods:
The data were retrieved from a prospective collected database. Variables from patients’ admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
Results:
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
Conclusion:
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Keywords:Acid-base equilibriumAcidosis, respiratoryIntensive care unitsRespiration, artificialRespiratory distress syndrome, adultSee moreViews0Abstract
Original ArticleMetabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2016;28(1):19-26
DOI 10.5935/0103-507X.20160009
Views0ABSTRACT
Objective:
Hypercapnia resulting from protective ventilation in acute respiratory distress syndrome triggers metabolic pH compensation, which is not entirely characterized. We aimed to describe this metabolic compensation.
Methods:
The data were retrieved from a prospective collected database. Variables from patients’ admission and from hypercapnia installation until the third day after installation were gathered. Forty-one patients with acute respiratory distress syndrome were analyzed, including twenty-six with persistent hypercapnia (PaCO2 > 50mmHg > 24 hours) and 15 non-hypercapnic (control group). An acid-base quantitative physicochemical approach was used for the analysis.
Results:
The mean ages in the hypercapnic and control groups were 48 ± 18 years and 44 ± 14 years, respectively. After the induction of hypercapnia, pH markedly decreased and gradually improved in the ensuing 72 hours, consistent with increases in the standard base excess. The metabolic acid-base adaptation occurred because of decreases in the serum lactate and strong ion gap and increases in the inorganic apparent strong ion difference. Furthermore, the elevation in the inorganic apparent strong ion difference occurred due to slight increases in serum sodium, magnesium, potassium and calcium. Serum chloride did not decrease for up to 72 hours after the initiation of hypercapnia.
Conclusion:
In this explanatory study, the results indicate that metabolic acid-base adaptation, which is triggered by acute persistent hypercapnia in patients with acute respiratory distress syndrome, is complex. Furthermore, further rapid increases in the standard base excess of hypercapnic patients involve decreases in serum lactate and unmeasured anions and increases in the inorganic apparent strong ion difference by means of slight increases in serum sodium, magnesium, calcium, and potassium. Serum chloride is not reduced.
Keywords:Acid-base equilibriumAcidosis, respiratoryIntensive care unitsRespiration, artificialRespiratory distress syndrome, adultSee more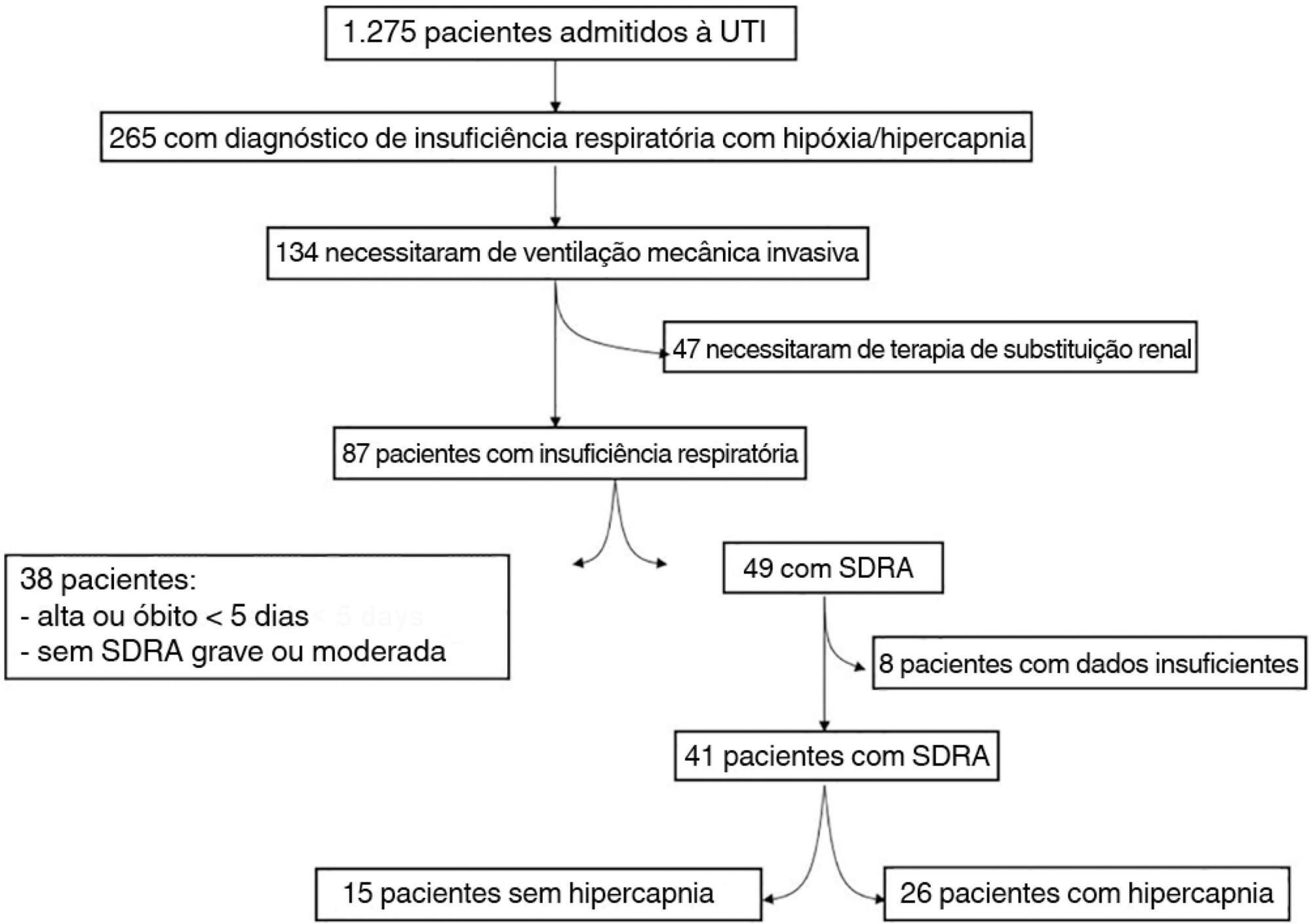
-
Original Article
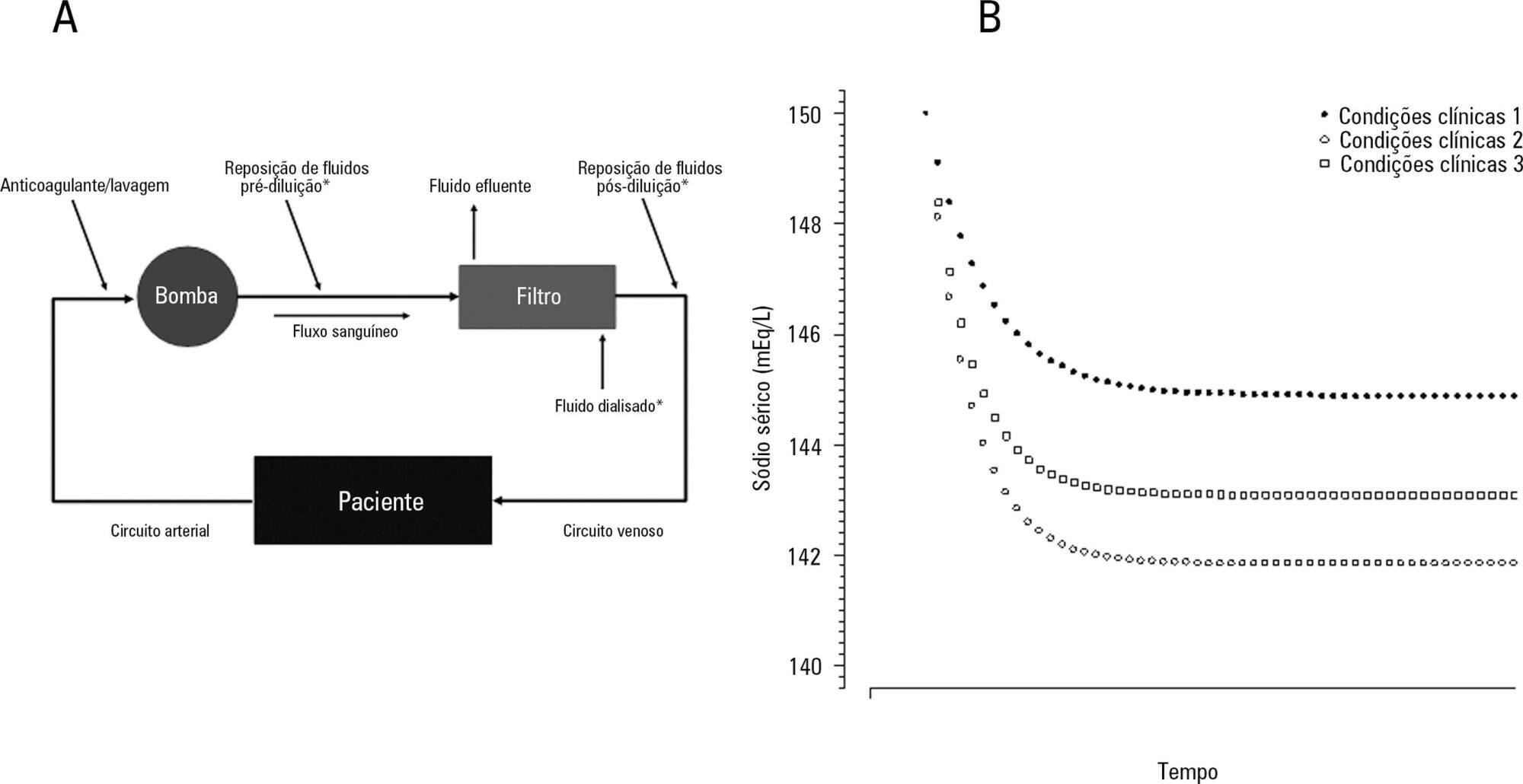
Insights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
Abstract
Original ArticleInsights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
Methods:
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
Results:
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Conclusions:
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose – formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
Views0Abstract
Original ArticleInsights about serum sodium behavior after 24 hours of continuous renal replacement therapy
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
Methods:
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
Results:
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Conclusions:
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose – formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
-
Case Reports
Varicella associated acute respiratory distress syndrome in an adult patient: an example for extracorporeal respiratory support in Brazilian endemic diseases
Rev Bras Ter Intensiva. 2014;26(4):410-415
Abstract
Case ReportsVaricella associated acute respiratory distress syndrome in an adult patient: an example for extracorporeal respiratory support in Brazilian endemic diseases
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
Views0A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Keywords:Case reportsChickenpoxExtracorporeal membrane oxygenationIntensive care unitsRespiration, artificialrespiratory failureSee moreViews0Abstract
Case ReportsVaricella associated acute respiratory distress syndrome in an adult patient: an example for extracorporeal respiratory support in Brazilian endemic diseases
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
Views0A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Keywords:Case reportsChickenpoxExtracorporeal membrane oxygenationIntensive care unitsRespiration, artificialrespiratory failureSee more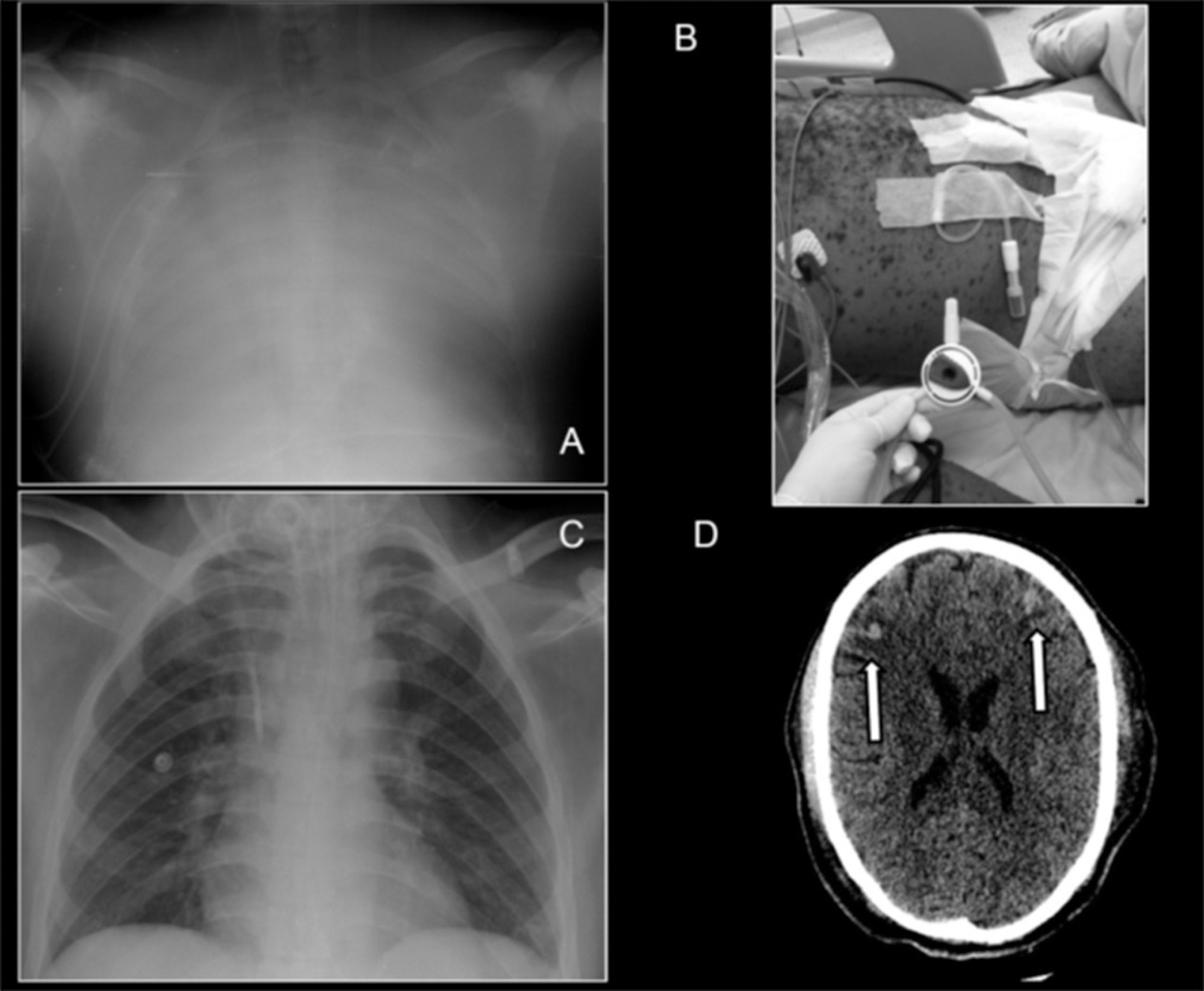
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis