artificial respiration Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):72-78
DOI 10.1590/S0103-507X2012000100011
OBJECTIVE: To assess the effects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients. METHODS: This cross-sectional, quantitative, observational study enrolled patients who were admitted to the intensive care unit, sedated and mechanically ventilated. The infusion of sedative and analgesic drugs aimed to maintain a Ramsay scale sedation level of 4 to 6. Passive mobilization consisted of hip and knee flexion-extension movements for five minutes. After 10 minutes of rest, an additional five minutes of flexion-extension passive movements was performed for the shoulders. Hemodynamic assessments (heart rate and systolic, diastolic and mean blood pressure) were performed one minute before the mobilization protocol and one minute after each phase. The double product and myocardial oxygen consumption were calculated using appropriate formulas. RESULTS: A total of 13 patients (69.2% male, with a mean age of 69.1 ± 15.8 years) were admitted from June to December, 2011. Passive mobilization led to statistically significant increases in heart rate, double product and myocardial oxygen consumption. However, mean blood pressure was not significantly altered. CONCLUSIONS: Our results suggest that passive mobilization of mechanically ventilated and sedated patients is safe and provides beneficial effects on acute hemodynamic parameters, particularly heart rate, although mean blood pressure is not significantly altered
Abstract
Rev Bras Ter Intensiva. 2012;24(1):72-78
DOI 10.1590/S0103-507X2012000100011
OBJECTIVE: To assess the effects of passive mobilization on acute hemodynamic responses in mechanically ventilated patients. METHODS: This cross-sectional, quantitative, observational study enrolled patients who were admitted to the intensive care unit, sedated and mechanically ventilated. The infusion of sedative and analgesic drugs aimed to maintain a Ramsay scale sedation level of 4 to 6. Passive mobilization consisted of hip and knee flexion-extension movements for five minutes. After 10 minutes of rest, an additional five minutes of flexion-extension passive movements was performed for the shoulders. Hemodynamic assessments (heart rate and systolic, diastolic and mean blood pressure) were performed one minute before the mobilization protocol and one minute after each phase. The double product and myocardial oxygen consumption were calculated using appropriate formulas. RESULTS: A total of 13 patients (69.2% male, with a mean age of 69.1 ± 15.8 years) were admitted from June to December, 2011. Passive mobilization led to statistically significant increases in heart rate, double product and myocardial oxygen consumption. However, mean blood pressure was not significantly altered. CONCLUSIONS: Our results suggest that passive mobilization of mechanically ventilated and sedated patients is safe and provides beneficial effects on acute hemodynamic parameters, particularly heart rate, although mean blood pressure is not significantly altered
Abstract
Rev Bras Ter Intensiva. 2010;22(3):264-269
DOI 10.1590/S0103-507X2010000300008
OBJECTIVES: In mechanically ventilated patients, humidifier devices are used to heat and moisturize the inspired gas. Heating and humidifying inspired gas may prevent complications associated with the respiratory mucosa dryness such as mucus plugging and endotracheal tube occlusion. Two devices have been commonly used to this, either heated humidifier or the heat moisture exchange filter. This study aimed to compare the effects of the heated humidifier and a model of heat moisture exchange filter on respiratory mechanics in mechanically ventilated neurological patients. METHODS: This was a randomized crossover trial, involving 31 neurological patients under mechanical ventilation randomly assigned to the humidification devices. Expired tidal volume, peak inspiratory flow, peak expiratory flow, static compliance, dynamic compliance and respiratory system resistance were evaluated. Statistical analysis used the Kolmogorov-Smirnov test and Student's t test for paired samples, in which P values < 0.05 were considered significant. RESULTS: The heat moisture exchanger filter decreased expired tidal volume, peak inspiratory flow, peak expiratory flow (p < 0.001) and dynamic compliance (p = 0.002), and increased respiratory system resistance (p < 0.001). CONCLUSION: In the studied population, the use of a heat moisture exchange filter model leaded to several changes on respiratory mechanics parameters.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):264-269
DOI 10.1590/S0103-507X2010000300008
OBJECTIVES: In mechanically ventilated patients, humidifier devices are used to heat and moisturize the inspired gas. Heating and humidifying inspired gas may prevent complications associated with the respiratory mucosa dryness such as mucus plugging and endotracheal tube occlusion. Two devices have been commonly used to this, either heated humidifier or the heat moisture exchange filter. This study aimed to compare the effects of the heated humidifier and a model of heat moisture exchange filter on respiratory mechanics in mechanically ventilated neurological patients. METHODS: This was a randomized crossover trial, involving 31 neurological patients under mechanical ventilation randomly assigned to the humidification devices. Expired tidal volume, peak inspiratory flow, peak expiratory flow, static compliance, dynamic compliance and respiratory system resistance were evaluated. Statistical analysis used the Kolmogorov-Smirnov test and Student's t test for paired samples, in which P values < 0.05 were considered significant. RESULTS: The heat moisture exchanger filter decreased expired tidal volume, peak inspiratory flow, peak expiratory flow (p < 0.001) and dynamic compliance (p = 0.002), and increased respiratory system resistance (p < 0.001). CONCLUSION: In the studied population, the use of a heat moisture exchange filter model leaded to several changes on respiratory mechanics parameters.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
OBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient's positioning in the bed during hospitalization in intensive care unity, it's necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
OBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient's positioning in the bed during hospitalization in intensive care unity, it's necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):38-44
DOI 10.1590/S0103-507X2006000100008
BACKGROUND AND OBJECTIVES: The ventilator-associated pneumonia (VAP) is a severe infection that presents multiple causes which can vary depending on the type of intensive care unit, type of patients, emphasizing the needs for vigilance measures with local data. The aim of this study is to describe the incidence, risk factors and mortality of VAP in patients in a surgical ICU. METHODS: Prospective cohort conducted from January 2004 to January 2005. It was included all the patients in mechanical ventilation, followed daily to collect data about demographics, diagnostic, APACHE II and TISS 28 scores, duration of mechanical ventilation, length of stay, incidence of VAP and mortality. RESULTS: 462 patients were studied; age 57.2 ± 16.6 years, 55% men. The mean APACHE II score was 18.3 and the incidence of VAP was 18.8%. The TISS score at admission OR = 1.050 (IC 95%: 1.003-1.050) and the enteral nutrition OR = 5.609 (IC 3.351-9.388) were factors associated with VAP and the prophylactic use of antibiotics was a factor of protection OR = 0.399 (IC95%: 0.177-0.902). The patients with VAP had longer length of stay in ICU (10.3 ± 10.7 vs 4.9 ± 3.3 days), higher median of duration of mechanical ventilation (4 vs 1 days), higher mean of TISS 28 (24.4 ± 4.6 vs 22.8 ± 4.5), and higher crude mortality (46 vs 28.8%) when compared with the patients without VAP. CONCLUSIONS: VAP was a frequent infection in surgical patients in mechanical ventilation. Enteral nutrition and admission TISS were risk factors and the previous use of antibiotics was protection factor to develop VAP. In our sample the results demonstrate that VAP is associated with higher duration in mechanical ventilation, longer length of stay and higher mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):38-44
DOI 10.1590/S0103-507X2006000100008
BACKGROUND AND OBJECTIVES: The ventilator-associated pneumonia (VAP) is a severe infection that presents multiple causes which can vary depending on the type of intensive care unit, type of patients, emphasizing the needs for vigilance measures with local data. The aim of this study is to describe the incidence, risk factors and mortality of VAP in patients in a surgical ICU. METHODS: Prospective cohort conducted from January 2004 to January 2005. It was included all the patients in mechanical ventilation, followed daily to collect data about demographics, diagnostic, APACHE II and TISS 28 scores, duration of mechanical ventilation, length of stay, incidence of VAP and mortality. RESULTS: 462 patients were studied; age 57.2 ± 16.6 years, 55% men. The mean APACHE II score was 18.3 and the incidence of VAP was 18.8%. The TISS score at admission OR = 1.050 (IC 95%: 1.003-1.050) and the enteral nutrition OR = 5.609 (IC 3.351-9.388) were factors associated with VAP and the prophylactic use of antibiotics was a factor of protection OR = 0.399 (IC95%: 0.177-0.902). The patients with VAP had longer length of stay in ICU (10.3 ± 10.7 vs 4.9 ± 3.3 days), higher median of duration of mechanical ventilation (4 vs 1 days), higher mean of TISS 28 (24.4 ± 4.6 vs 22.8 ± 4.5), and higher crude mortality (46 vs 28.8%) when compared with the patients without VAP. CONCLUSIONS: VAP was a frequent infection in surgical patients in mechanical ventilation. Enteral nutrition and admission TISS were risk factors and the previous use of antibiotics was protection factor to develop VAP. In our sample the results demonstrate that VAP is associated with higher duration in mechanical ventilation, longer length of stay and higher mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):344-350
DOI 10.1590/S0103-507X2006000400005
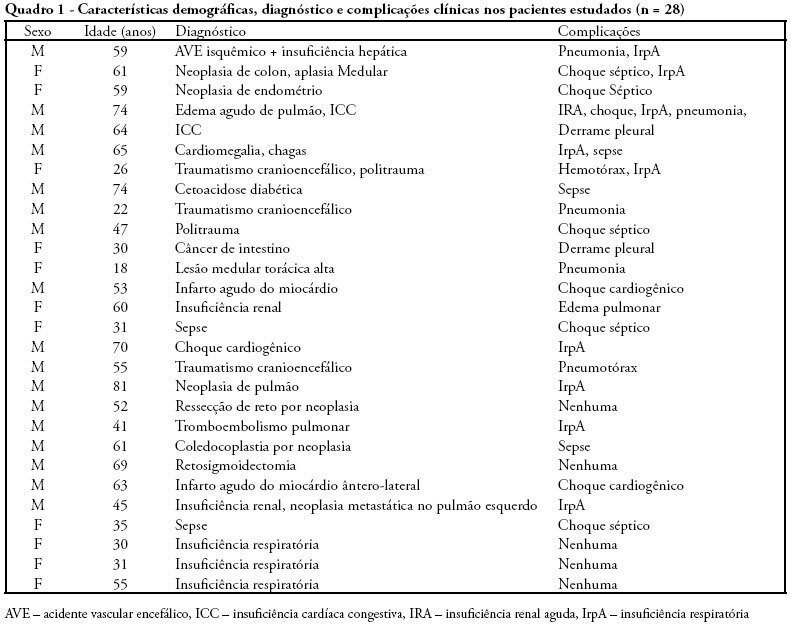
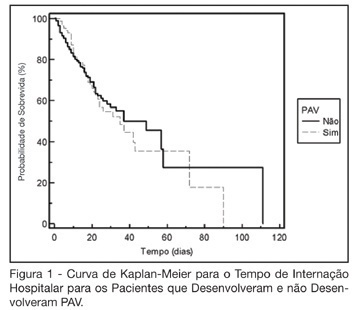
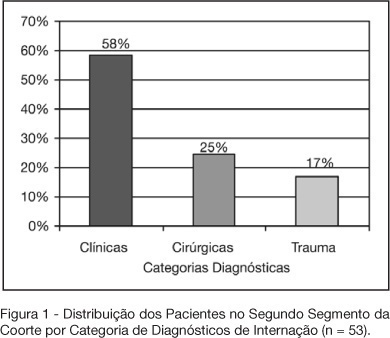
BACKGROUND AND OBJECTIVES: Variable magnitude of impact on the outcomes of the critically ill patients has been credited to ventilation-associated pneumonia, in terms of mortality, length of hospital stay and mechanic ventilation days. Three objectives have been defined in this study: mortality and incidence of ventilation-associated pneumonia before and after the implantation of a prophylaxis protocol (primary objectives); microbiologic mapping (secondary objective) as an instrument to optimize therapy. METHODS: A historical cohort was followed during the period of August 2001 to January 2004, fragmented in two segments, pre (until January 2003, n = 52) and post-implantation of the mentioned protocol, the analysis of mortality and microbiologic mapping been performed in the second segment (control group n = 39 and case group n = 14). RESULTS: The incidence rates from 2001 to 2003 were respectively 28.05‰ ± 12.92‰, 22.45‰ ± 10.18‰ and 10.75‰ ± 7.61‰. The decrease in this rate after the intervention did not reach statistical significance (p > 0.4). Mortality rates were 49% in the control group (CI 95 = 33% to 65%) and 43% in the case group (CI 95 = 14% to 72%), OR = 0.88 (CI 95 = 0.26 to 2.94), without statistical significance either (p = 0.65). Eight bronco-alveolar lavage were obtained (57%), 50% with multiple flora. Pseudomonas aeruginosa was isolated in six patients (75%), Acinetobacter sp in one case (12.5 %) and methicilin-resistent Staphylococcus aureus (MRSA) in one (12.5%). Other Gram negative bacilli producers of extended spectrum betalactamase (ESBL) were isolated in two cases (25%) and Stenotrophomonas maltophilia in another (12.5%). CONCLUSIONS: The incidence rate of ventilation-associated pneumonia revealed a tendency to considerable reduction after the utilization of the prophylaxis protocol, while the results suggest no impact on mortality rates. Further prospective evaluation of a greater sample is required, in order to get to definite conclusions regarding prognosis. The isolated germs were, in its majority, high risk pathogens to multiresistance to antibiotics, pointing the necessity of knowledge of local susceptibility profile, so that an adequate initial therapeutic strategy can be undertaken.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):344-350
DOI 10.1590/S0103-507X2006000400005
BACKGROUND AND OBJECTIVES: Variable magnitude of impact on the outcomes of the critically ill patients has been credited to ventilation-associated pneumonia, in terms of mortality, length of hospital stay and mechanic ventilation days. Three objectives have been defined in this study: mortality and incidence of ventilation-associated pneumonia before and after the implantation of a prophylaxis protocol (primary objectives); microbiologic mapping (secondary objective) as an instrument to optimize therapy. METHODS: A historical cohort was followed during the period of August 2001 to January 2004, fragmented in two segments, pre (until January 2003, n = 52) and post-implantation of the mentioned protocol, the analysis of mortality and microbiologic mapping been performed in the second segment (control group n = 39 and case group n = 14). RESULTS: The incidence rates from 2001 to 2003 were respectively 28.05‰ ± 12.92‰, 22.45‰ ± 10.18‰ and 10.75‰ ± 7.61‰. The decrease in this rate after the intervention did not reach statistical significance (p > 0.4). Mortality rates were 49% in the control group (CI 95 = 33% to 65%) and 43% in the case group (CI 95 = 14% to 72%), OR = 0.88 (CI 95 = 0.26 to 2.94), without statistical significance either (p = 0.65). Eight bronco-alveolar lavage were obtained (57%), 50% with multiple flora. Pseudomonas aeruginosa was isolated in six patients (75%), Acinetobacter sp in one case (12.5 %) and methicilin-resistent Staphylococcus aureus (MRSA) in one (12.5%). Other Gram negative bacilli producers of extended spectrum betalactamase (ESBL) were isolated in two cases (25%) and Stenotrophomonas maltophilia in another (12.5%). CONCLUSIONS: The incidence rate of ventilation-associated pneumonia revealed a tendency to considerable reduction after the utilization of the prophylaxis protocol, while the results suggest no impact on mortality rates. Further prospective evaluation of a greater sample is required, in order to get to definite conclusions regarding prognosis. The isolated germs were, in its majority, high risk pathogens to multiresistance to antibiotics, pointing the necessity of knowledge of local susceptibility profile, so that an adequate initial therapeutic strategy can be undertaken.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)