
You searched for:"Lucienne Tibery Queiroz Cardoso"
We found (9) results for your search.-
Original Article
Refusal of beds and triage of patients admitted to intensive care units in Brazil: a cross-sectional national survey
- Rafaela de Lemos Lepre
 ,
, - Ana Luiza Mezzaroba ,
- Lucienne Tibery Queiroz Cardoso ,
- Tiemi Matsuo ,
- Cíntia Magalhães Carvalho Grion
Abstract
Original ArticleRefusal of beds and triage of patients admitted to intensive care units in Brazil: a cross-sectional national survey
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
- Rafaela de Lemos Lepre ,
- Ana Luiza Mezzaroba ,
- Lucienne Tibery Queiroz Cardoso ,
- Tiemi Matsuo ,
- Cíntia Magalhães Carvalho Grion
Views4See moreABSTRACT
Objective:
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
Methods:
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
Results:
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Conclusions:
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
Views4

Abstract
Original ArticleRefusal of beds and triage of patients admitted to intensive care units in Brazil: a cross-sectional national survey
Rev Bras Ter Intensiva. 2022;34(4):484-491
DOI 10.5935/0103-507X.20220264-en
- Rafaela de Lemos Lepre ,
- Ana Luiza Mezzaroba ,
- Lucienne Tibery Queiroz Cardoso ,
- Tiemi Matsuo ,
- Cíntia Magalhães Carvalho Grion
Views4See moreABSTRACT
Objective:
To obtain data on bed refusal in intensive care units in Brazil and to evaluate the use of triage systems by professionals.
Methods:
A cross-sectional survey. Using the Delphi methodology, a questionnaire was created contemplating the objectives of the study. Physicians and nurses enrolled in the research network of the Associação de Medicina Intensiva Brasileira (AMIBnet) were invited to participate. A web platform (SurveyMonkey®) was used to distribute the questionnaire. The variables in this study were measured in categories and expressed as proportions. The chi-square test or Fisher’s exact test was used to verify associations. The significance level was set at 5%.
Results:
In total, 231 professionals answered the questionnaire, representing all regions of the country. The national intensive care units had an occupancy rate of more than 90% always or frequently for 90.8% of the participants. Among the participants, 84.4% had already refused admitting patients to the intensive care unit due to the capacity of the unit. Half of the Brazilian institutions (49.7%) did not have triage protocols for admission to intensive beds.
Conclusions:
Bed refusal due to high occupancy rates is common in Brazilian intensive care units. Even so, half of the services in Brazil do not adopt protocols for triage of beds.
- Rafaela de Lemos Lepre
-
Original Article
Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee moreViews0Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee more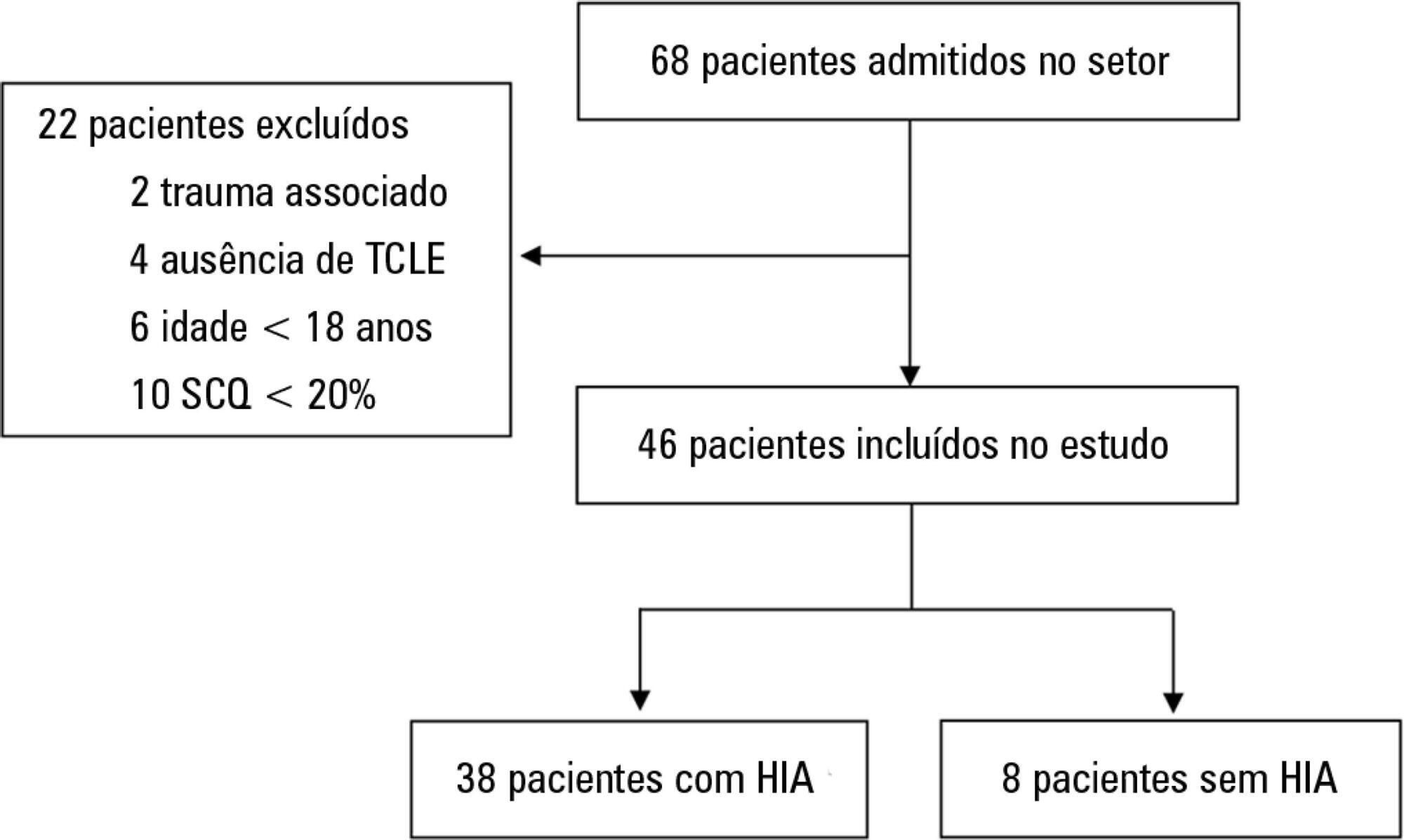
-
Original Articles
Evaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee moreViews1Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee more
-
Original Article
Nursing Activities Score and workload in the intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2014;26(3):292-298
Abstract
Original ArticleNursing Activities Score and workload in the intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
Views1See moreObjective:
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
Methods:
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
Results:
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients’ condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
Conclusion:
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.
Views1Abstract
Original ArticleNursing Activities Score and workload in the intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
Views1See moreObjective:
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
Methods:
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
Results:
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients’ condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
Conclusion:
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.
-
Original Articles – Clinical Research
The performance of a rapid response team in the management of code yellow events at a university hospital
Rev Bras Ter Intensiva. 2013;25(2):99-105
Abstract
Original Articles – Clinical ResearchThe performance of a rapid response team in the management of code yellow events at a university hospital
Rev Bras Ter Intensiva. 2013;25(2):99-105
DOI 10.5935/0103-507X.20130020
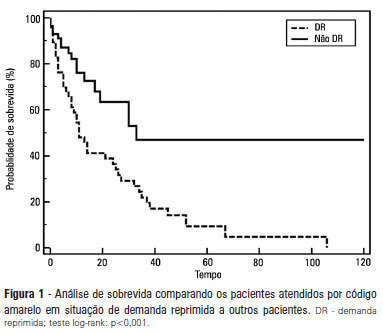
Views0See moreOBJECTIVE: To describe the epidemiological data of the clinical instability events in patients attended to by the rapid response team and to identify prognostic factors. METHODS: This was a longitudinal study, performed from January to July 2010, with an adult inpatient population in a hospital environment. The data collected regarding the code yellow service included the criteria of the clinical instability, the drug and non-drug therapies administered and the activities and procedures performed. The outcomes evaluated were the need for intensive care unit admission and the hospital mortality rates. A level of p=0.05 was considered to be significant. RESULTS: A total of 150 code yellow events that occurred in 104 patients were evaluated. The most common causes were related to acute respiratory insufficiency with hypoxia or a change in the respiratory rate and a concern of the team about the patient’s clinical condition. It was necessary to request a transfer to the intensive care unit in 80 of the 150 cases (53.3%). It was necessary to perform 42 procedures. The most frequent procedures were orotracheal intubation and the insertion of a central venous catheter. The patients who were in critical condition and had to wait for an intensive care unit bed had a higher risk of death compared to the other patients (hazard ratio: 3.12; 95% CI: 1.80-5.40; p<0.001). CONCLUSIONS: There are patients in critical condition that require expert intensive care in the regular ward unit hospital beds. The events that most frequently led to the code yellow activation were related to hemodynamic and respiratory support. The interventions performed indicate the need for a physician on the team. The situation of pent-up demand is associated with a higher mortality rate.
Views0Abstract
Original Articles – Clinical ResearchThe performance of a rapid response team in the management of code yellow events at a university hospital
Rev Bras Ter Intensiva. 2013;25(2):99-105
DOI 10.5935/0103-507X.20130020
Views0See moreOBJECTIVE: To describe the epidemiological data of the clinical instability events in patients attended to by the rapid response team and to identify prognostic factors. METHODS: This was a longitudinal study, performed from January to July 2010, with an adult inpatient population in a hospital environment. The data collected regarding the code yellow service included the criteria of the clinical instability, the drug and non-drug therapies administered and the activities and procedures performed. The outcomes evaluated were the need for intensive care unit admission and the hospital mortality rates. A level of p=0.05 was considered to be significant. RESULTS: A total of 150 code yellow events that occurred in 104 patients were evaluated. The most common causes were related to acute respiratory insufficiency with hypoxia or a change in the respiratory rate and a concern of the team about the patient’s clinical condition. It was necessary to request a transfer to the intensive care unit in 80 of the 150 cases (53.3%). It was necessary to perform 42 procedures. The most frequent procedures were orotracheal intubation and the insertion of a central venous catheter. The patients who were in critical condition and had to wait for an intensive care unit bed had a higher risk of death compared to the other patients (hazard ratio: 3.12; 95% CI: 1.80-5.40; p<0.001). CONCLUSIONS: There are patients in critical condition that require expert intensive care in the regular ward unit hospital beds. The events that most frequently led to the code yellow activation were related to hemodynamic and respiratory support. The interventions performed indicate the need for a physician on the team. The situation of pent-up demand is associated with a higher mortality rate.
-
Original Articles
Parenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
Abstract
Original ArticlesParenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
Views2Objective:
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
Methods:
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
Results:
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Conclusions:
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Keywords:Acinetobacter baumanniiAcute kidney injuryColistin/therapeutic useCross infection/drug therapyDeathIntensive carePseudomonas aeruginosaSee moreViews2Abstract
Original ArticlesParenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
Views2Objective:
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
Methods:
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
Results:
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Conclusions:
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Keywords:Acinetobacter baumanniiAcute kidney injuryColistin/therapeutic useCross infection/drug therapyDeathIntensive carePseudomonas aeruginosaSee more
-
Original Articles
The experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
Abstract
Original ArticlesThe experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
Views0OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient’s stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient’s admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Keywords:Family relationsIn-patientsIntensive care unitsProfessional-family relationsQualitative researchSee moreViews0Abstract
Original ArticlesThe experience of family members of patients staying in intensive care units
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
Views0OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient’s stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient’s admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Keywords:Family relationsIn-patientsIntensive care unitsProfessional-family relationsQualitative researchSee more
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis