Renal insufficiency Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 - 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 - 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Abstract
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 - 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 - 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
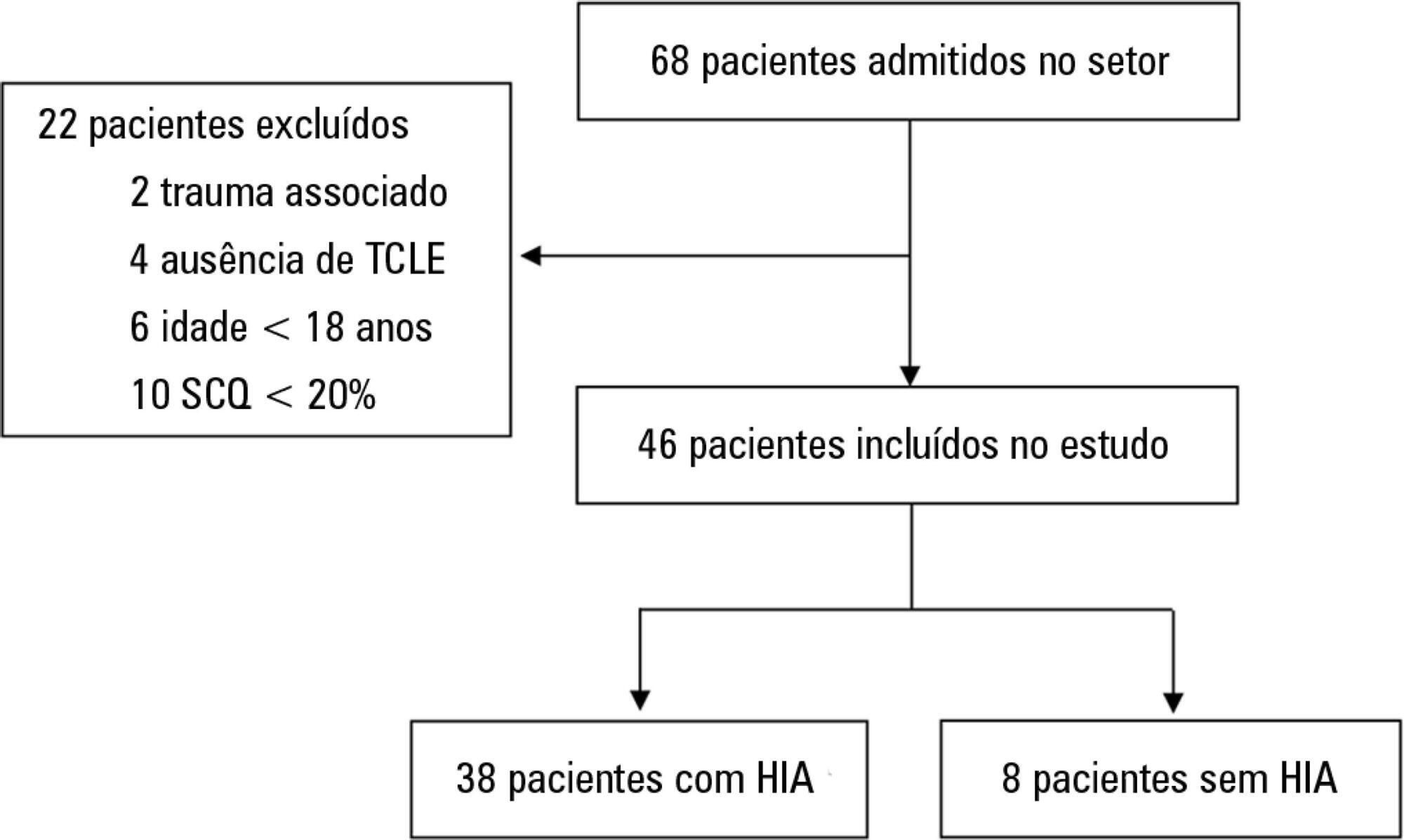
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
In the 2014 - 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 - 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
In the 2014 - 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 - 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.

Abstract
Rev Bras Ter Intensiva. 2017;29(3):346-353
DOI 10.5935/0103-507X.20170045
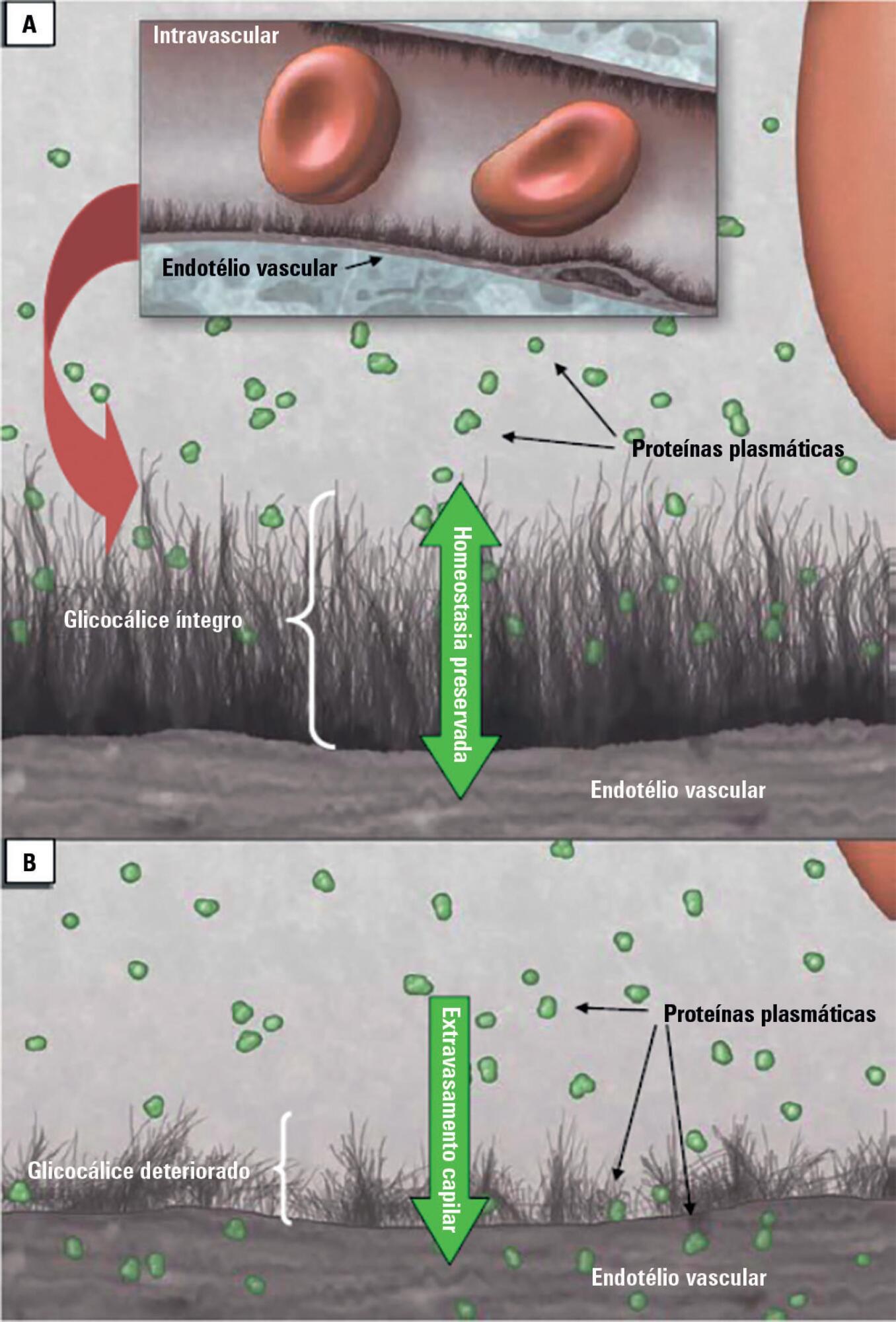
Patients admitted to an intensive care unit are prone to cumulated fluid overload and receive intravenous volumes through the aggressive resuscitation recommended for septic shock treatment, as well as other fluid sources related to medications and nutritional support. The liberal liquid supply strategy has been associated with higher morbidity and mortality. Although there are few prospective pediatric studies, new strategies are being proposed. This non-systematic review discusses the pathophysiology of fluid overload, its consequences, and the available therapeutic strategies. During systemic inflammatory response syndrome, the endothelial glycocalyx is damaged, favoring fluid extravasation and resulting in interstitial edema. Extravasation to the third space results in longer mechanical ventilation, a greater need for renal replacement therapy, and longer intensive care unit and hospital stays, among other changes. Proper hemodynamic monitoring, as well as cautious infusion of fluids, can minimize these damages. Once cumulative fluid overload is established, treatment with long-term use of loop diuretics may lead to resistance to these medications. Strategies that can reduce intensive care unit morbidity and mortality include the early use of vasopressors (norepinephrine) to improve cardiac output and renal perfusion, the use of a combination of diuretics and aminophylline to induce diuresis, and the use of sedation and early mobilization protocols.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):346-353
DOI 10.5935/0103-507X.20170045
Patients admitted to an intensive care unit are prone to cumulated fluid overload and receive intravenous volumes through the aggressive resuscitation recommended for septic shock treatment, as well as other fluid sources related to medications and nutritional support. The liberal liquid supply strategy has been associated with higher morbidity and mortality. Although there are few prospective pediatric studies, new strategies are being proposed. This non-systematic review discusses the pathophysiology of fluid overload, its consequences, and the available therapeutic strategies. During systemic inflammatory response syndrome, the endothelial glycocalyx is damaged, favoring fluid extravasation and resulting in interstitial edema. Extravasation to the third space results in longer mechanical ventilation, a greater need for renal replacement therapy, and longer intensive care unit and hospital stays, among other changes. Proper hemodynamic monitoring, as well as cautious infusion of fluids, can minimize these damages. Once cumulative fluid overload is established, treatment with long-term use of loop diuretics may lead to resistance to these medications. Strategies that can reduce intensive care unit morbidity and mortality include the early use of vasopressors (norepinephrine) to improve cardiac output and renal perfusion, the use of a combination of diuretics and aminophylline to induce diuresis, and the use of sedation and early mobilization protocols.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):373-381
DOI 10.5935/0103-507X.20170051
Novel biomarkers can be suitable for early acute kidney injury diagnosis and the prediction of the need for dialysis. It remains unclear whether such biomarkers may also play a role in the prediction of recovery after established acute kidney injury or in aiding the decision of when to stop renal support therapy. PubMed, Web of Science and Google Scholar were searched for studies that reported on the epidemiology of renal recovery after acute kidney injury, the risk factors of recovery versus non-recovery after acute kidney injury, and potential biomarkers of acute kidney injury recovery. The reference lists of these articles and relevant review articles were also reviewed. Final references were selected for inclusion in the review based on their relevance. New biomarkers exhibited a potential role in the early diagnosis of acute kidney injury recovery. Urine HGF, IGFBP-7, TIMP-2 and NGAL may improve our ability to predict the odds and timing of recovery and eventually renal support withdrawal. Acute kidney injury recovery requires more study, and its definition needs to be standardized to allow for better and more powerful research on biomarkers because some of them show potential for the prediction of acute kidney injury recovery.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):373-381
DOI 10.5935/0103-507X.20170051
Novel biomarkers can be suitable for early acute kidney injury diagnosis and the prediction of the need for dialysis. It remains unclear whether such biomarkers may also play a role in the prediction of recovery after established acute kidney injury or in aiding the decision of when to stop renal support therapy. PubMed, Web of Science and Google Scholar were searched for studies that reported on the epidemiology of renal recovery after acute kidney injury, the risk factors of recovery versus non-recovery after acute kidney injury, and potential biomarkers of acute kidney injury recovery. The reference lists of these articles and relevant review articles were also reviewed. Final references were selected for inclusion in the review based on their relevance. New biomarkers exhibited a potential role in the early diagnosis of acute kidney injury recovery. Urine HGF, IGFBP-7, TIMP-2 and NGAL may improve our ability to predict the odds and timing of recovery and eventually renal support withdrawal. Acute kidney injury recovery requires more study, and its definition needs to be standardized to allow for better and more powerful research on biomarkers because some of them show potential for the prediction of acute kidney injury recovery.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):111-114
DOI 10.5935/0103-507X.20170016
Rhabdomyolysis is a process of muscle destruction that can present with varying clinical manifestations. In pediatric patients, its main etiology is infectious diseases. We present a previously healthy adolescent who was admitted to our emergency department with a four-day history of myalgia, muscle weakness and dark urine. At presentation, she was dehydrated. Blood analysis revealed acute renal failure and increased muscular enzymes.
She was transferred to our pediatric intensive care unit. Medical therapies for correction of dehydration and the ionic and metabolic consequences of renal failure were performed. Due to oliguria, renal replacement therapy was initiated. An etiological investigation revealed a beta-oxidation defect. Metabolic diseases are a known cause of rhabdomyolysis. Muscular destruction should be diagnosed early in order to avoid its potential consequences. Generally, the treatment of rhabdomyolysis is conservative, although in some situations, a more invasive approach is needed.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):111-114
DOI 10.5935/0103-507X.20170016
Rhabdomyolysis is a process of muscle destruction that can present with varying clinical manifestations. In pediatric patients, its main etiology is infectious diseases. We present a previously healthy adolescent who was admitted to our emergency department with a four-day history of myalgia, muscle weakness and dark urine. At presentation, she was dehydrated. Blood analysis revealed acute renal failure and increased muscular enzymes.
She was transferred to our pediatric intensive care unit. Medical therapies for correction of dehydration and the ionic and metabolic consequences of renal failure were performed. Due to oliguria, renal replacement therapy was initiated. An etiological investigation revealed a beta-oxidation defect. Metabolic diseases are a known cause of rhabdomyolysis. Muscular destruction should be diagnosed early in order to avoid its potential consequences. Generally, the treatment of rhabdomyolysis is conservative, although in some situations, a more invasive approach is needed.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):70-77
DOI 10.5935/0103-507X.20160015
Identify prognostic factors related to mortality and non-recovery of renal function.
A prospective single-center study was conducted at the intensive care medicine department of a university hospital between 2012 and 2015. Patients with acute kidney injury receiving continuous renal replacement therapy were included in the study. Clinical and analytical parameters were collected, and the reasons for initiation and discontinuation of renal replacement therapy were examined.
A total of 41 patients were included in the study, of whom 43.9% had sepsis. The median Simplified Acute Physiology Score II (SAPSII) was 56 and the mortality was 53.7%, with a predicted mortality of 59.8%. The etiology of acute kidney injury was often multifactorial (56.1%). Survivors had lower cumulative fluid balance (median = 3,600mL, interquartile range [IQR] = 1,175 - 8,025) than non-survivors (median = 12,000mL, IQR = 6,625 - 17,875; p = 0.004). Patients who recovered renal function (median = 51.0, IQR = 45.8 - 56.2) had lower SAPS II than those who do not recover renal function (median = 73, IQR = 54 - 85; p = 0.005) as well as lower fluid balance (median = 3,850, IQR = 1,425 - 8,025 versus median = 11,500, IQR = 6,625 - 16,275; p = 0.004).
SAPS II at admission and cumulative fluid balance during renal support therapy were risk factors for mortality and non-recovery of renal function among critically ill patients with acute kidney injury needing renal replacement therapy.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):70-77
DOI 10.5935/0103-507X.20160015
Identify prognostic factors related to mortality and non-recovery of renal function.
A prospective single-center study was conducted at the intensive care medicine department of a university hospital between 2012 and 2015. Patients with acute kidney injury receiving continuous renal replacement therapy were included in the study. Clinical and analytical parameters were collected, and the reasons for initiation and discontinuation of renal replacement therapy were examined.
A total of 41 patients were included in the study, of whom 43.9% had sepsis. The median Simplified Acute Physiology Score II (SAPSII) was 56 and the mortality was 53.7%, with a predicted mortality of 59.8%. The etiology of acute kidney injury was often multifactorial (56.1%). Survivors had lower cumulative fluid balance (median = 3,600mL, interquartile range [IQR] = 1,175 - 8,025) than non-survivors (median = 12,000mL, IQR = 6,625 - 17,875; p = 0.004). Patients who recovered renal function (median = 51.0, IQR = 45.8 - 56.2) had lower SAPS II than those who do not recover renal function (median = 73, IQR = 54 - 85; p = 0.005) as well as lower fluid balance (median = 3,850, IQR = 1,425 - 8,025 versus median = 11,500, IQR = 6,625 - 16,275; p = 0.004).
SAPS II at admission and cumulative fluid balance during renal support therapy were risk factors for mortality and non-recovery of renal function among critically ill patients with acute kidney injury needing renal replacement therapy.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)