Perioperative care Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(4):402-410
DOI 10.5935/2965-2774.20230174-pt
To describe, with a larger number of patients in a real-world scenario following routine implementation, intensivist-led ultrasound-guided percutaneous dilational tracheostomy and the possible risks and complications of the procedure not identified in clinical trials.
This was a phase IV cohort study of patients admitted to three intensive care units of a quaternary academic hospital who underwent intensivist-led ultrasound-guided percutaneous tracheostomy in Brazil from September 2017 to December 2021.
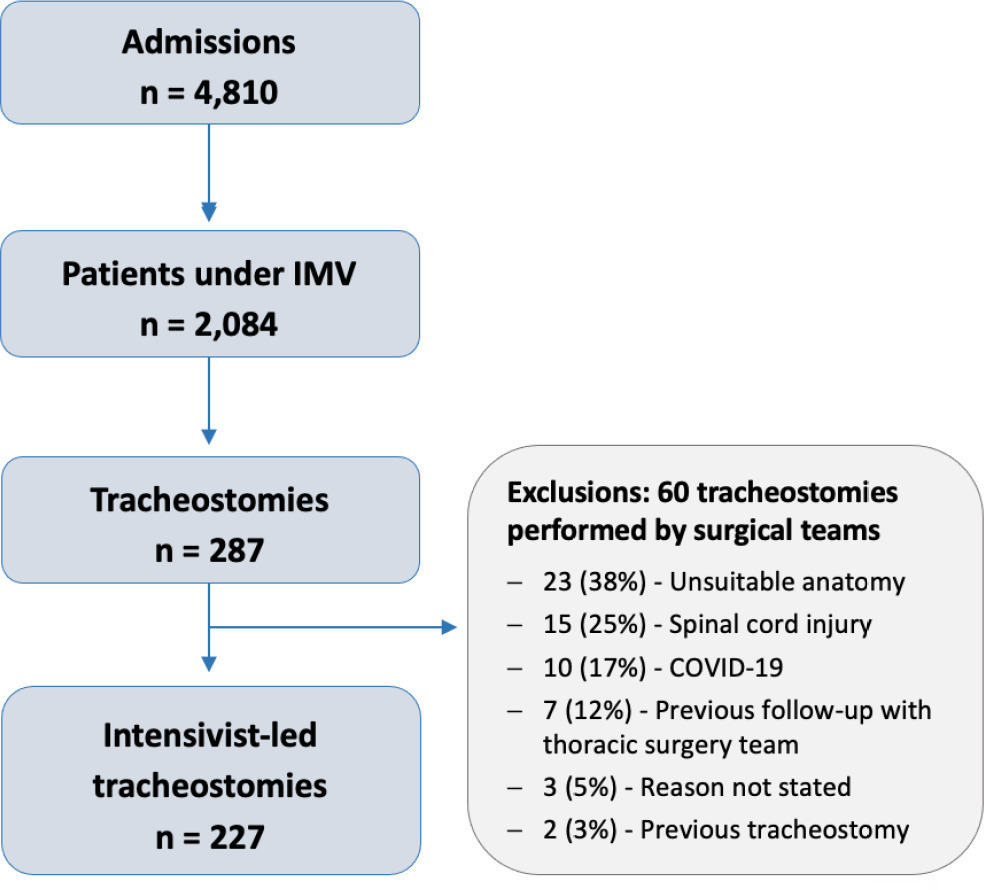
There were 4,810 intensive care unit admissions during the study period; 2,084 patients received mechanical ventilation, and 287 underwent tracheostomy, 227 of which were performed at bedside by the intensive care team. The main reason for intensive care unit admission was trauma, and for perform a tracheostomy it was a neurological impairment or an inability to protect the airways. The median time from intubation to tracheostomy was 14 days. Intensive care residents performed 76% of the procedures. At least one complication occurred in 29.5% of the procedures, the most common being hemodynamic instability and extubation during the procedure, with only 3 serious complications. The intensive care unit mortality was 29.1%, and the hospital mortality was 43.6%.
Intensivist-led ultrasound-guided percutaneous tracheostomy is feasible out of a clinical trial context with outcomes and complications comparable to those in the literature. Intensivists can acquire this competence during their training but should be aware of potential complications to enhance procedural safety.
Abstract
Crit Care Sci. 2023;35(4):402-410
DOI 10.5935/2965-2774.20230174-pt
To describe, with a larger number of patients in a real-world scenario following routine implementation, intensivist-led ultrasound-guided percutaneous dilational tracheostomy and the possible risks and complications of the procedure not identified in clinical trials.
This was a phase IV cohort study of patients admitted to three intensive care units of a quaternary academic hospital who underwent intensivist-led ultrasound-guided percutaneous tracheostomy in Brazil from September 2017 to December 2021.
There were 4,810 intensive care unit admissions during the study period; 2,084 patients received mechanical ventilation, and 287 underwent tracheostomy, 227 of which were performed at bedside by the intensive care team. The main reason for intensive care unit admission was trauma, and for perform a tracheostomy it was a neurological impairment or an inability to protect the airways. The median time from intubation to tracheostomy was 14 days. Intensive care residents performed 76% of the procedures. At least one complication occurred in 29.5% of the procedures, the most common being hemodynamic instability and extubation during the procedure, with only 3 serious complications. The intensive care unit mortality was 29.1%, and the hospital mortality was 43.6%.
Intensivist-led ultrasound-guided percutaneous tracheostomy is feasible out of a clinical trial context with outcomes and complications comparable to those in the literature. Intensivists can acquire this competence during their training but should be aware of potential complications to enhance procedural safety.
Abstract
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 - 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 - 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Abstract
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 - 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 - 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):325-330
DOI 10.5935/0103-507X.20170050
To compare the incidence of complications and the duration of hospitalization of patients undergoing bariatric surgery admitted to the intensive care unit or a post-surgical hospitalization unit.
This retrospective observational study included 828 patients admitted between January 2010 and February 2015 during the immediate postoperative period of bariatric surgery in a hospital. Data were collected via electronic medical records. The Mann-Whitney test was used to compare continuous variables, and the chi-square was used to compare categorical variables.
Patients in both groups had similar demographic characteristics, with no significant differences in anthropometric data and comorbidities. There was no significant difference in the comparison of complications between the two groups. However, the group admitted to the intensive care unit had longer hospitalization times (median of 3 days versus 2 days, p < 0.05), and hospital costs were 8% higher.
The present study found no benefit in the routine admittance of patients to the intensive care unit after undergoing bariatric surgery. This practice increased hospitalization time and hospital costs, which wasted resources. It is necessary to create objective criteria to identify patients requiring intensive care unit admission after bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):325-330
DOI 10.5935/0103-507X.20170050
To compare the incidence of complications and the duration of hospitalization of patients undergoing bariatric surgery admitted to the intensive care unit or a post-surgical hospitalization unit.
This retrospective observational study included 828 patients admitted between January 2010 and February 2015 during the immediate postoperative period of bariatric surgery in a hospital. Data were collected via electronic medical records. The Mann-Whitney test was used to compare continuous variables, and the chi-square was used to compare categorical variables.
Patients in both groups had similar demographic characteristics, with no significant differences in anthropometric data and comorbidities. There was no significant difference in the comparison of complications between the two groups. However, the group admitted to the intensive care unit had longer hospitalization times (median of 3 days versus 2 days, p < 0.05), and hospital costs were 8% higher.
The present study found no benefit in the routine admittance of patients to the intensive care unit after undergoing bariatric surgery. This practice increased hospitalization time and hospital costs, which wasted resources. It is necessary to create objective criteria to identify patients requiring intensive care unit admission after bariatric surgery.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (33) COVID-19 (45) Critical care (115) Critical illness (54) ICU (25) Infant, newborn (27) Intensive care (72) Intensive care units (254) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (75) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (117) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)