ICU Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
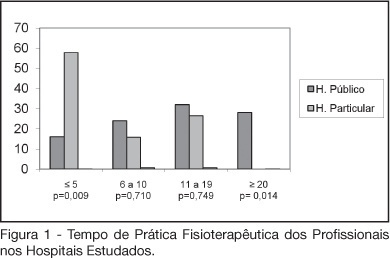
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
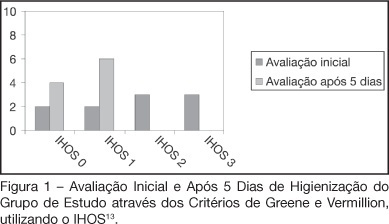
BACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
BACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
BACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists' knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient's family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
BACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists' knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient's family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
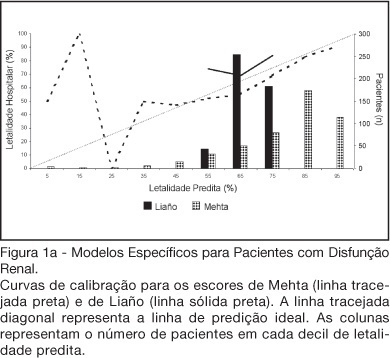
BACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
BACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
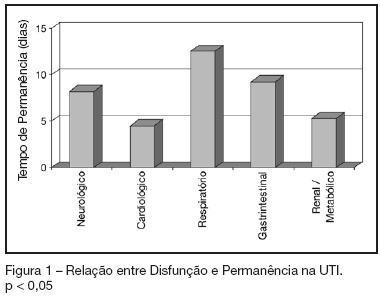
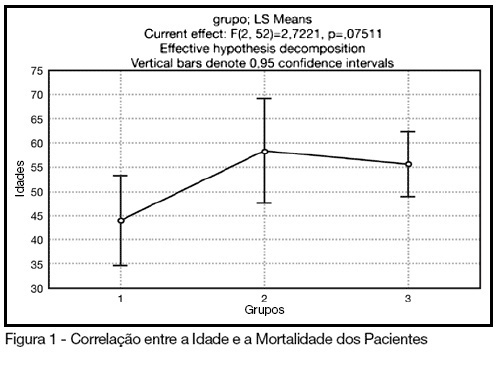
BACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
BACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):276-281
DOI 10.1590/S0103-507X2006000300010
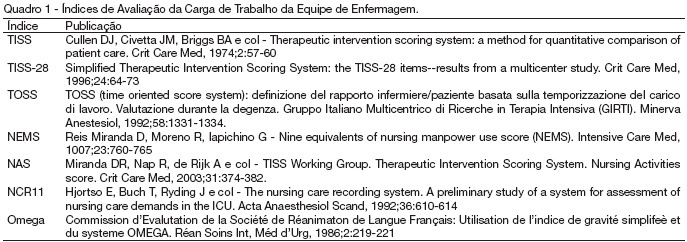
BACKGROUND AND OBJECTIVES: ICU is the hospital sectors that have interrupt assistance. Assistance with quality is a challenge for those who run human resources. It is also important to know the risk of the patient to the better use of resources. The aim of this study is to identify most used severity indexes in intensive care and classify them according with their finality METHODS: Library research (medline), using the key words: "Scoring systems and ICU". The articles were selected in the period from March to May 2005. Books and thesis were also used. RESULTS: We identify seven indexes evaluating nursing workload: TISS, TISS-28, TOSS, NEMS, NAS, NCR11, and Omega. We identify 21 indexes evaluating clinical status: Killip Glasgow CRI APACHE II e III, Ransom, SS, SSS, SAPS, MLR, MPM, LIS, ARPI, SAPS (II), MPM II, ODIN, Ontario, MODS, SOFA, LOD, and PSI). CONCLUSIONS: Although indexes evaluating nursing workload are in a lower number, they are also fundamental to preview the need for material and human resources.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):276-281
DOI 10.1590/S0103-507X2006000300010
BACKGROUND AND OBJECTIVES: ICU is the hospital sectors that have interrupt assistance. Assistance with quality is a challenge for those who run human resources. It is also important to know the risk of the patient to the better use of resources. The aim of this study is to identify most used severity indexes in intensive care and classify them according with their finality METHODS: Library research (medline), using the key words: "Scoring systems and ICU". The articles were selected in the period from March to May 2005. Books and thesis were also used. RESULTS: We identify seven indexes evaluating nursing workload: TISS, TISS-28, TOSS, NEMS, NAS, NCR11, and Omega. We identify 21 indexes evaluating clinical status: Killip Glasgow CRI APACHE II e III, Ransom, SS, SSS, SAPS, MLR, MPM, LIS, ARPI, SAPS (II), MPM II, ODIN, Ontario, MODS, SOFA, LOD, and PSI). CONCLUSIONS: Although indexes evaluating nursing workload are in a lower number, they are also fundamental to preview the need for material and human resources.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):190-195
DOI 10.1590/S0103-507X2006000200013
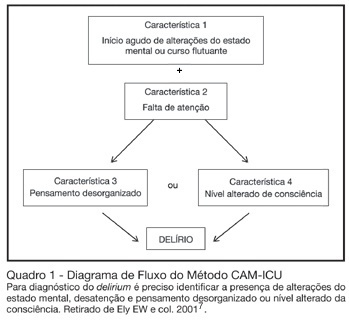
BACKGROUND AND OBJECTIVES: Delirium is a frequent finding in the critically ill patient. Although it is associated with increased morbidity and mortality, it is often not recognized by intensive care doctors. This review will address the main issues regarding delirium in critically ill patients. CONTENTS: Definition, incidence, mortality, risk factors, diagnosis, and treatment of delirium in the critically ill. CONCLUSIONS: Deliriumis defined as a disturbance of consciousness, attention, cognition and perception that occurs frequently in critically ill patients. It occurs in as many as 80% of mechanically ventilated ICU patients. Risk factors for delirium include acute systemic illnesses, older age, pre-existing cognitive impairment, sleep deprivation, and medications with anticholinergic activity. Although new assessment tools are available for rapidly and accurately measuring deliriumin critically ill patients, healthcare professionals still do not regularly monitor for this condition. In recent years, the emphasis in the approach to delirium has shifted to systematic screening and prevention. Haloperidol remains the standard treatment for delirium, but there is some evidence for the efficacy of risperidone.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):190-195
DOI 10.1590/S0103-507X2006000200013
BACKGROUND AND OBJECTIVES: Delirium is a frequent finding in the critically ill patient. Although it is associated with increased morbidity and mortality, it is often not recognized by intensive care doctors. This review will address the main issues regarding delirium in critically ill patients. CONTENTS: Definition, incidence, mortality, risk factors, diagnosis, and treatment of delirium in the critically ill. CONCLUSIONS: Deliriumis defined as a disturbance of consciousness, attention, cognition and perception that occurs frequently in critically ill patients. It occurs in as many as 80% of mechanically ventilated ICU patients. Risk factors for delirium include acute systemic illnesses, older age, pre-existing cognitive impairment, sleep deprivation, and medications with anticholinergic activity. Although new assessment tools are available for rapidly and accurately measuring deliriumin critically ill patients, healthcare professionals still do not regularly monitor for this condition. In recent years, the emphasis in the approach to delirium has shifted to systematic screening and prevention. Haloperidol remains the standard treatment for delirium, but there is some evidence for the efficacy of risperidone.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (33) COVID-19 (45) Critical care (115) Critical illness (54) Infant, newborn (27) Intensive care (72) Intensive care units (254) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (75) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (117) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98) Septic shock (25)