
You searched for:"Fernando Osni Machado"
We found (15) results for your search.-
Special Articles
Guidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
Abstract
Special ArticlesGuidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views0See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
Views0

Abstract
Special ArticlesGuidelines for the assessment and acceptance of potential brain-dead organ donors
Rev Bras Ter Intensiva. 2016;28(3):220-255
DOI 10.5935/0103-507X.20160049
Views0See moreABSTRACT
Organ transplantation is the only alternative for many patients with terminal diseases. The increasing disproportion between the high demand for organ transplants and the low rate of transplants actually performed is worrisome. Some of the causes of this disproportion are errors in the identification of potential organ donors and in the determination of contraindications by the attending staff. Therefore, the aim of the present document is to provide guidelines for intensive care multi-professional staffs for the recognition, assessment and acceptance of potential organ donors.
-
Original Articles – Clinical Research
Routine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
Abstract
Original Articles – Clinical ResearchRoutine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
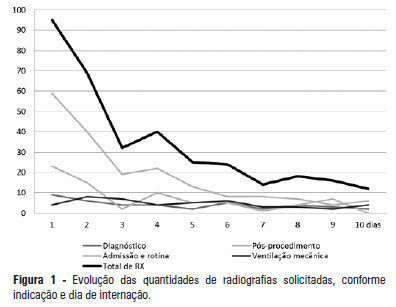
Views0See moreOBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
Views0Abstract
Original Articles – Clinical ResearchRoutine chest radiography in intensive care: impact on decision-making
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
Views0See moreOBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
-
Special Articles
Guidelines for potential multiple organ donors (adult). Part III: organ-specific recommendations
Rev Bras Ter Intensiva. 2011;23(4):410-425
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult). Part III: organ-specific recommendations
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
Views0See moreBrain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient’s metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
Views0Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult). Part III: organ-specific recommendations
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
Views0See moreBrain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient’s metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
-
Special Articles
Guidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
Views0Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
-
Special Articles
Guidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
Views0See moreThe role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
Views0Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part II. Mechanical ventilation, endocrine metabolic management, hematological and infectious aspects
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
Views0See moreThe role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
-
Original Articles
Perceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
Abstract
Original ArticlesPerceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
Views0ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Keywords:Medical FutilityQuestionnairesTerminal careTerminally illTreatment refusalWithholding TreatmentSee moreViews0Abstract
Original ArticlesPerceptions about end of life treatment in Argentina, Brazil and Uruguay intensive care units
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
Views0ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Keywords:Medical FutilityQuestionnairesTerminal careTerminally illTreatment refusalWithholding TreatmentSee more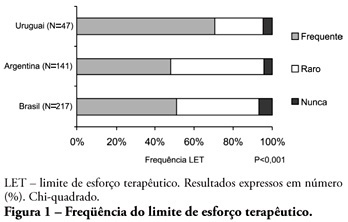
-
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
Abstract
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
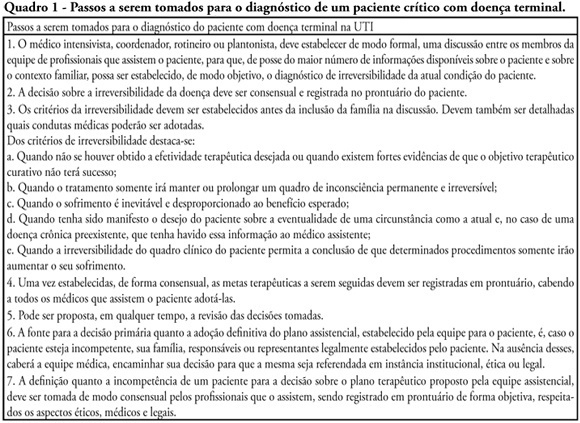
Views4See moreWithholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB – Brazilian Association of Intensive Care.
Views4Abstract
1st Forum of the Southern Cone End-of-Life Study Group: proposal for care of patients, bearers of terminal disease staying in the ICU
Rev Bras Ter Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
Views4See moreWithholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB – Brazilian Association of Intensive Care.
-
Original Articles
Evaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
Abstract
Original ArticlesEvaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
Views0See moreOBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student’s t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
Views0Abstract
Original ArticlesEvaluation of medical decisions at the end-of-life process
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
Views0See moreOBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student’s t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis