Terminal care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2011;23(1):78-86
DOI 10.1590/S0103-507X2011000100013
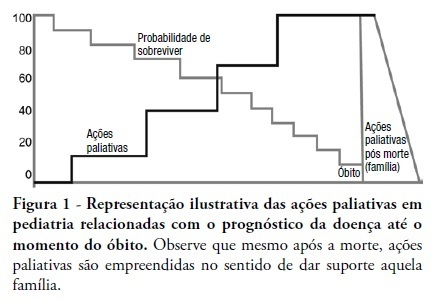
This review discusses the main dilemmas and difficulties related to end-of-life decision's in children with terminal and irreversible diseases and propose a rational sequence for delivering palliative care to this patients' group. The Medline and Lilacs databases were searched using the terms 'end of life', 'palliative care', 'death' and 'terminal disease' for articles published in recent years. The most relevant articles and those enrolling pediatric patients were selected and compared to previous authors' studies in this field. The current Brazilian Medical Ethics Code (2010) was analyzed regarding end-oflife practices and palliative care for terminal patients. Lack of knowledge, insufficient specific training, and legal concerns are the main reasons why end-of-life decisions in terminal children are based on medical opinion with scarce family participation. The current Brazilian Medical Ethics Code (2010) fully supports end-of-life decisions made consensually with active family participation. Honest dialogue with the family regarding diagnostic, prognostic, therapeutic and palliative care measures should be established gradually to identify the best strategy to meet the child's end-of-life needs. Treatment focused on the child's welfare combined with the family's participation is the basis for successful palliative care of children with terminal diseases.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):78-86
DOI 10.1590/S0103-507X2011000100013
This review discusses the main dilemmas and difficulties related to end-of-life decision's in children with terminal and irreversible diseases and propose a rational sequence for delivering palliative care to this patients' group. The Medline and Lilacs databases were searched using the terms 'end of life', 'palliative care', 'death' and 'terminal disease' for articles published in recent years. The most relevant articles and those enrolling pediatric patients were selected and compared to previous authors' studies in this field. The current Brazilian Medical Ethics Code (2010) was analyzed regarding end-oflife practices and palliative care for terminal patients. Lack of knowledge, insufficient specific training, and legal concerns are the main reasons why end-of-life decisions in terminal children are based on medical opinion with scarce family participation. The current Brazilian Medical Ethics Code (2010) fully supports end-of-life decisions made consensually with active family participation. Honest dialogue with the family regarding diagnostic, prognostic, therapeutic and palliative care measures should be established gradually to identify the best strategy to meet the child's end-of-life needs. Treatment focused on the child's welfare combined with the family's participation is the basis for successful palliative care of children with terminal diseases.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
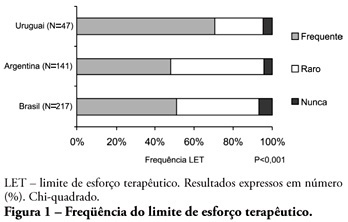
ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
PURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects' speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors' experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses' actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses' feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses' view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
PURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects' speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors' experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses' actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses' feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses' view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.