bioethics Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(1):38-47
DOI 10.5935/0103-507X.20210004
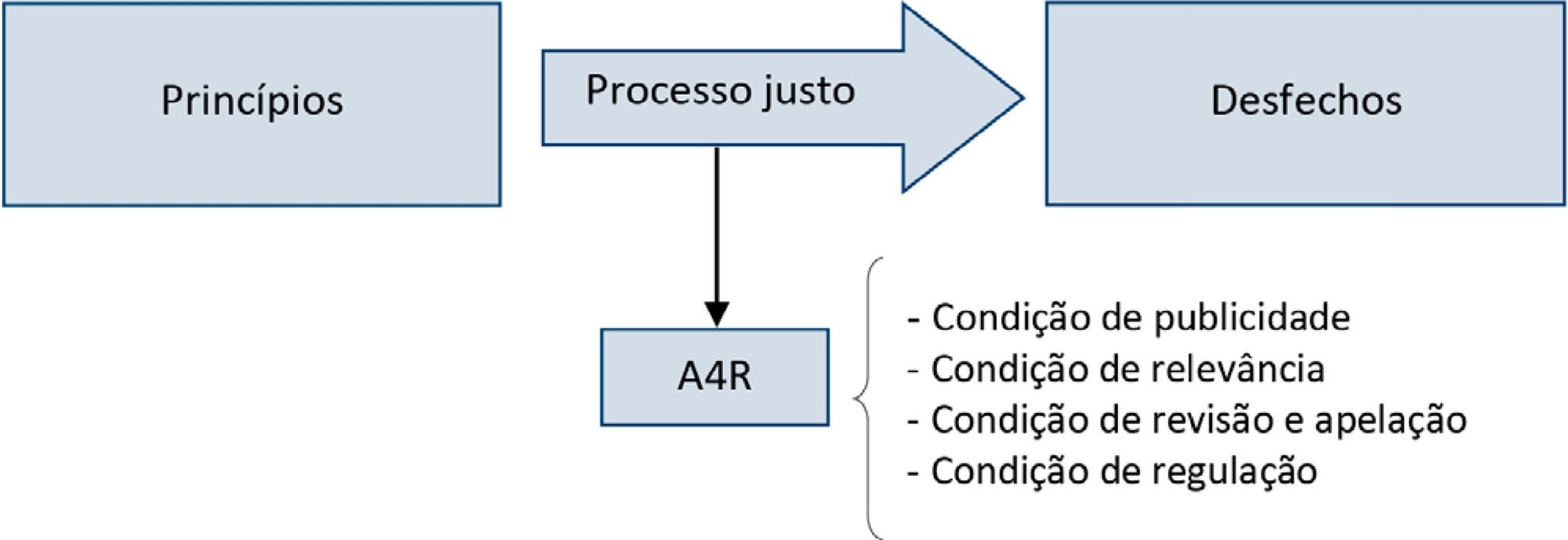
Triage for intensive care unit admission is a frequent event and is associated to worse clinical outcomes. The process of triage is variable and may be influenced by biases and prejudices, which could lead to potentially unfair decisions. The Brazilian Federal Council of Medicine (Conselho Federal de Medicina) has recently released a guideline for intensive care unit admission and discharge. The aim of this paper is to evaluate the ethical dilemmas related to the implementation of this guideline, through the accountability for reasonabless approach, known as A4R, as elaborated by Norman Daniels. We conclude that the guideline contemplates A4R conditions, but we observe that there is a need for indication of A4R-concordant criteria to operationalize the guidelines.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):38-47
DOI 10.5935/0103-507X.20210004
Triage for intensive care unit admission is a frequent event and is associated to worse clinical outcomes. The process of triage is variable and may be influenced by biases and prejudices, which could lead to potentially unfair decisions. The Brazilian Federal Council of Medicine (Conselho Federal de Medicina) has recently released a guideline for intensive care unit admission and discharge. The aim of this paper is to evaluate the ethical dilemmas related to the implementation of this guideline, through the accountability for reasonabless approach, known as A4R, as elaborated by Norman Daniels. We conclude that the guideline contemplates A4R conditions, but we observe that there is a need for indication of A4R-concordant criteria to operationalize the guidelines.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
The world is aging. In Brazil, and in several other countries in the world, changes in population's age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
The world is aging. In Brazil, and in several other countries in the world, changes in population's age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
PURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects' speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors' experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses' actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses' feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses' view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):148-154
DOI 10.1590/S0103-507X2009000200006
PURPOSE: Identify and evaluate the perception of Intensivist Nurses in a University Hospital in Londrina, of dysthanasia in terminal patients at the Intensive Care Unit. METHODS: Qualitative study. Data were collected by semi-structured recorded interview involving nine nurses working in a university hospital intensive care units, during January 2009. A thematic analysis was used to evaluate subjects' speech and identify discussion categories. RESULTS: Five categories were identified, discussed based on the authors' experience and literature, namely: measures prolonging life of patients with no chance of cure in the intensive care unit; nurses' actions/reactions when facing dysthanasia; reasons leading to prolonging life of patients with no chance of cure; nurses' feelings about dysthanasia and life prolongation; care measures as opposed to dysthanasia. CONCLUSION: Experiencing of nurses when facing dysthanasia actions was shown to be complex, a factor of suffering, frustration and discomfort for these professionals. In the nurses' view, lack of communication stands out as an important factor for dysthanasia, and measures to replace dysthanasia are those relieving suffering.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
OBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student's t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):141-147
DOI 10.1590/S0103-507X2009000200005
OBJECTIVES: To evaluate the medical decisions at end-of-life of patients admitted at HU/UFSC and to compare these decisions and the profile of patients who died in the intensive care unit (ICU) to those who died in medical (MW) and surgical wards (SW). METHODS: This is a retrospective and observational study. Demographic data, clinical features, treatment and the end-of-life care decisions of adult patients who died in wards and the intensive care unit of HU/UFSC from July/2004 to December/2008 were analyzed . For statistical analysis the Student's t, χ2 and ANOVA tests were used: (significance p <0.05). RESULTS: An analysis was made of 1124 deaths: 404 occurred in ICU, 607 in MW and 113 in SW. The overall hospital mortality rate was 5.9% (ICU=24.49%, MW=7.2%, SW=1.69%). Mean ages of patients were: ICU=56.7, MW=69.3 and SW=70.4 years (p <0.01). Withholding/withdrawing life support was performed prior to 30.7% of deaths in the intensive care unit and 10% in the wards (p <0.01). Cardiopulmonary resuscitation was not carried out in 65% of cases in ICU, 79% in MW and 62% in SW. Besides cardiopulmonary resuscitation, the more frequent withholding/withdrawing life support in the intensive care unit were vasoactive drugs and in the wards refusal of admission to intensive care unit . Do-not-resuscitate order was documented in 2.4% of cases in ICU and 2.6% in MW. Palliative and comfort care were provided to 2% of patients in ICU, 11.5% in MW and 8% in SW. Terminality of the disease was recognized in 40% of cases in ICU, 34.6% in MW and 16.8% in SW. CONCLUSIONS: The profile of patients who died and medical decisions during the end-of-life process were different in the intensive care unit, clinical and surgical wards.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):364-368
DOI 10.1590/S0103-507X2007000300018
BACKGROUND AND OBJECTIVES: To analyze and discuss the medical aspects related to the family involvement in the decision making process regarding end of life care to children admitted to the pediatric intensive care unit (PICU). CONTENTS: The authors selected articles on end-of-life care published during the last years searching the PubMed, MedLine and LILACS database, with special interest on studies of death conducted in pediatric intensive care units in Brazil, Latin America, Europe and North America, using the following keywords: death, bioethics, PICU, decision-making, terminal care, parents interview and life support limitation (LSL). CONCLUSIONS: Several studies have demonstrated the relevance of the family participation in the decision making process regarding LSL. In our region the family participation in this process is not stimulated and valued, ranging from 20%-55%. The authors present a practical sequence for discussing and defining LSL with the families. Despite of the family participation in the decision making process for LSL be legally, morally and ethically accepted in developed countries, this approach is adopted in a very few cases in our region. To explain this difficulty observed among the Brazilian pediatric intensivist, some studies should be conducted in our region.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):364-368
DOI 10.1590/S0103-507X2007000300018
BACKGROUND AND OBJECTIVES: To analyze and discuss the medical aspects related to the family involvement in the decision making process regarding end of life care to children admitted to the pediatric intensive care unit (PICU). CONTENTS: The authors selected articles on end-of-life care published during the last years searching the PubMed, MedLine and LILACS database, with special interest on studies of death conducted in pediatric intensive care units in Brazil, Latin America, Europe and North America, using the following keywords: death, bioethics, PICU, decision-making, terminal care, parents interview and life support limitation (LSL). CONCLUSIONS: Several studies have demonstrated the relevance of the family participation in the decision making process regarding LSL. In our region the family participation in this process is not stimulated and valued, ranging from 20%-55%. The authors present a practical sequence for discussing and defining LSL with the families. Despite of the family participation in the decision making process for LSL be legally, morally and ethically accepted in developed countries, this approach is adopted in a very few cases in our region. To explain this difficulty observed among the Brazilian pediatric intensivist, some studies should be conducted in our region.