Medical Ethics Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
The world is aging. In Brazil, and in several other countries in the world, changes in population's age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):432-436
DOI 10.1590/S0103-507X2009000400014
The world is aging. In Brazil, and in several other countries in the world, changes in population's age composition have been accompanied by an increase in demand for types of health care whose cost is high. Actually, some moral conflicts are arising from allocation of public resources for health, because the magnitude of social inequalities in health and limited resources require that priorities for public management are based on knowledge of the health situation and the impact of policies, programs, projects and actions on health. In this context, the intensive medicine, managers and physicians in intensive care are subject to moral conflicts, especially at the fair micro allocation resources for the elderly in the intensive care unit level. This paper attempts to review the situation of conflicts in the light of the tools of bioethics.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):247-254
DOI 10.1590/S0103-507X2009000300003
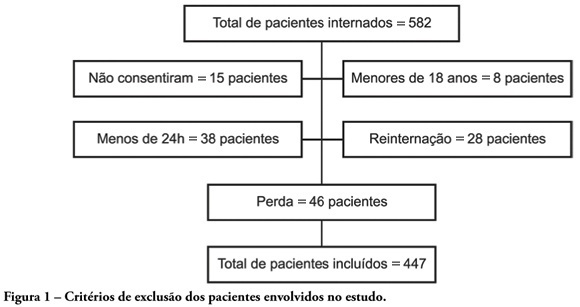
OBJECTIVES: Availability of state-of-the-art technology at intensive care units has often turned into a tool aggravating suffering by prolonging the end-of-life process. Distinguishing therapeutic persistence from therapeutic obstinacy has become a great challenge for present-day medicine. The aim of this study was to assess the benefit-harm relation in the use of life-sustaining therapies by means of an evolutionary system of individual prognostic assessment. METHODS: A cohort, prospective, observational study at the intensive care unit of the São Francisco De Paula University Hospital of UCPel, Pelotas RS from March 2006 to August 31, 2007. Individual prognostic assessments were recorded by using an evolutionary system, the UNICAMP II index, associated with albumin transferrin and lymphocytes serum levels, life- sustaining therapies and the outcome. Statistical analysis was carried out by the Student's t-test, ANOVA test, Chi-square test, Fisher's exact test, Spearman's correlation test and area under the receiver-operating characteristic curve. A p value < 0.05 was considered statistically significant. RESULTS: Four hundred forty seven patients were assessed during the study. Prevalence of death was significantly higher among those who received life-sustaining therapies at a later stage of the intervention, and those whose prognostic index and nutritional status worsened at an early stage of intervention. CONCLUSION: Assessment of individual evolutionary prognostic proved to be a useful method to objectively subsidize ethical decisions related to therapeutic persistence and therapeutic obstinacy.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):247-254
DOI 10.1590/S0103-507X2009000300003
OBJECTIVES: Availability of state-of-the-art technology at intensive care units has often turned into a tool aggravating suffering by prolonging the end-of-life process. Distinguishing therapeutic persistence from therapeutic obstinacy has become a great challenge for present-day medicine. The aim of this study was to assess the benefit-harm relation in the use of life-sustaining therapies by means of an evolutionary system of individual prognostic assessment. METHODS: A cohort, prospective, observational study at the intensive care unit of the São Francisco De Paula University Hospital of UCPel, Pelotas RS from March 2006 to August 31, 2007. Individual prognostic assessments were recorded by using an evolutionary system, the UNICAMP II index, associated with albumin transferrin and lymphocytes serum levels, life- sustaining therapies and the outcome. Statistical analysis was carried out by the Student's t-test, ANOVA test, Chi-square test, Fisher's exact test, Spearman's correlation test and area under the receiver-operating characteristic curve. A p value < 0.05 was considered statistically significant. RESULTS: Four hundred forty seven patients were assessed during the study. Prevalence of death was significantly higher among those who received life-sustaining therapies at a later stage of the intervention, and those whose prognostic index and nutritional status worsened at an early stage of intervention. CONCLUSION: Assessment of individual evolutionary prognostic proved to be a useful method to objectively subsidize ethical decisions related to therapeutic persistence and therapeutic obstinacy.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):359-363
DOI 10.1590/S0103-507X2007000300017
BACKGROUND AND OBJECTIVES: To analyze and discuss the medical practices related to the end-of-life care provided to children admitted to pediatric intensive care unit (PICU) in Brazil and in some countries located in the northern hemisphere. CONTENTS: Selected articles on end-of-life care published during the last years searching the PubMed, MedLine and LILACS database, with special interest on studies of death conducted in pediatric intensive care units in Brazil, Latin America, Europe and North America, using the following key words: death, bioethics, PICU, cardiopulmonary resuscitation and life support limitation (LSL). CONCLUSIONS: In North America and North Europe, the incidence of LSL is greater (60%-80%) than in south Europe and Latin America (30%-40%). In Brazil the incidence of LSL depends on the region and in the last decade it is increasing from 6% to 40%; being the do-not-reanimated order the most frequent mode of LSL. The family participation in the decision making process is not stimulated and incipient. Based on the literature review and on their experience the authors present the measures that they consider most efficient and recommended for managing this situation in our region. Despite of LSL in children with terminal and irreversible disease be considered ethically, morally and legally; these measures are still adopted in a very few circumstances in our region. Urgent changes in this behavior are necessary, specially related to family participation in the decision-making process.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):359-363
DOI 10.1590/S0103-507X2007000300017
BACKGROUND AND OBJECTIVES: To analyze and discuss the medical practices related to the end-of-life care provided to children admitted to pediatric intensive care unit (PICU) in Brazil and in some countries located in the northern hemisphere. CONTENTS: Selected articles on end-of-life care published during the last years searching the PubMed, MedLine and LILACS database, with special interest on studies of death conducted in pediatric intensive care units in Brazil, Latin America, Europe and North America, using the following key words: death, bioethics, PICU, cardiopulmonary resuscitation and life support limitation (LSL). CONCLUSIONS: In North America and North Europe, the incidence of LSL is greater (60%-80%) than in south Europe and Latin America (30%-40%). In Brazil the incidence of LSL depends on the region and in the last decade it is increasing from 6% to 40%; being the do-not-reanimated order the most frequent mode of LSL. The family participation in the decision making process is not stimulated and incipient. Based on the literature review and on their experience the authors present the measures that they consider most efficient and recommended for managing this situation in our region. Despite of LSL in children with terminal and irreversible disease be considered ethically, morally and legally; these measures are still adopted in a very few circumstances in our region. Urgent changes in this behavior are necessary, specially related to family participation in the decision-making process.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):137-143
DOI 10.1590/S0103-507X2007000200001
BACKGROUND AND OBJECTIVES: There is a growing tendency of looking for "dying with dignity", rather than to prolong death and suffering of terminal patients on intensive care units (ICU). This study aims to evaluate medical practices that suggest therapeutic limitation (TL) in patients who died in an adult ICU. METHODS: A retrospective exploratory study was carried out to evaluate medical records of patients who died in a general adult ICU of a private hospital in Salvador-BA, between January and August of 2003, after at least 24 hours from the admission. The patients were classified, in relation to their deaths, in: "not responding to cardiopulmonary resuscitation", "brain death", "decision not to resuscitate" (DNR) and "withhold or withdrawal life-support measures". RESULTS: Sixty seven patients were included, corresponding to 90.4% of the deaths occurred in this ICU during the referred period. The most of them (56.7%) were women and the patients’ mean age was 66.58 ± 17.86 years. Suggestive measures of TL were found in 59.7% of the patients, being "withhold of life-support measures" the most important (35.8%), followed by DNR (17.9%) and "withdrawal of life-support measures" (6%). The procedures most commonly omitted were use of vasoactive drugs and dialysis, while antibiotics were the most discontinued. The use of TL measures was more frequent in clinical patients. CONCLUSIONS: The results of the present study suggest high frequencies of medical conducts suggestive of TL in a general ICU in Northeast of Brazil. Therapeutic methods that could cause discomfort or suffering to the patients, as nutrition, sedation and analgesia, were rarely omitted or discontinued.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):137-143
DOI 10.1590/S0103-507X2007000200001
BACKGROUND AND OBJECTIVES: There is a growing tendency of looking for "dying with dignity", rather than to prolong death and suffering of terminal patients on intensive care units (ICU). This study aims to evaluate medical practices that suggest therapeutic limitation (TL) in patients who died in an adult ICU. METHODS: A retrospective exploratory study was carried out to evaluate medical records of patients who died in a general adult ICU of a private hospital in Salvador-BA, between January and August of 2003, after at least 24 hours from the admission. The patients were classified, in relation to their deaths, in: "not responding to cardiopulmonary resuscitation", "brain death", "decision not to resuscitate" (DNR) and "withhold or withdrawal life-support measures". RESULTS: Sixty seven patients were included, corresponding to 90.4% of the deaths occurred in this ICU during the referred period. The most of them (56.7%) were women and the patients’ mean age was 66.58 ± 17.86 years. Suggestive measures of TL were found in 59.7% of the patients, being "withhold of life-support measures" the most important (35.8%), followed by DNR (17.9%) and "withdrawal of life-support measures" (6%). The procedures most commonly omitted were use of vasoactive drugs and dialysis, while antibiotics were the most discontinued. The use of TL measures was more frequent in clinical patients. CONCLUSIONS: The results of the present study suggest high frequencies of medical conducts suggestive of TL in a general ICU in Northeast of Brazil. Therapeutic methods that could cause discomfort or suffering to the patients, as nutrition, sedation and analgesia, were rarely omitted or discontinued.