Medical Futility Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
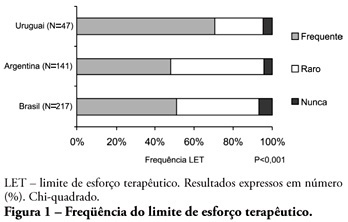
ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):125-132
DOI 10.1590/S0103-507X2010000200005
ABSTRACT OBJECTIVE: To evaluate end-of-life procedures in intensive care units. METHODS: A questionnaire was prepared by the End-of-Life Study Group of the Argentinean, Brazilian and Uruguayan Intensive Care societies, collecting data on the participants’ demographics, institutions and limit therapeutic effort (LTE) decision making process. During this cross sectional study, the societies’ multidisciplinary teams members completed the questionnaire either during scientific meetings or online. The variables were analyzed with the Chi-square test, with a p<0.05 significance level. RESULTS: 420 professionals completed the questionnaire. The Brazilian units had more beds, unrestricted visit was less frequent, their professionals were younger and worked more recently in intensive care units, and more non-medical professionals completed the questionnaire. Three visits daily was the more usual number of visits for the three countries. The most influencing LTE factors were prognosis, co-morbidities, and therapeutic futility. In the three countries, more than 90% of the completers had already made LTE decisions. Cardiopulmonary resuscitation, vasoactive drugs administration, dialysis and parenteral nutrition were the most suspended/refused therapies in the three countries. Suspension of mechanic ventilation was more frequent in Argentina, followed by Uruguay. Sedation and analgesia were the less suspended therapies in the three countries. Legal definement and ethical issues were mentioned as the main barriers for the LTE decision making process. CONCLUSION: LTE decisions are frequent among the professionals working in the three countries’ intensive care units. We found a more proactive LTE decision making trend In Argentina, and more equity for decisions distribution in Uruguay. This difference appears to be related to the participants’ different ages, experiences, professional types and genders.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):137-143
DOI 10.1590/S0103-507X2007000200001
BACKGROUND AND OBJECTIVES: There is a growing tendency of looking for "dying with dignity", rather than to prolong death and suffering of terminal patients on intensive care units (ICU). This study aims to evaluate medical practices that suggest therapeutic limitation (TL) in patients who died in an adult ICU. METHODS: A retrospective exploratory study was carried out to evaluate medical records of patients who died in a general adult ICU of a private hospital in Salvador-BA, between January and August of 2003, after at least 24 hours from the admission. The patients were classified, in relation to their deaths, in: "not responding to cardiopulmonary resuscitation", "brain death", "decision not to resuscitate" (DNR) and "withhold or withdrawal life-support measures". RESULTS: Sixty seven patients were included, corresponding to 90.4% of the deaths occurred in this ICU during the referred period. The most of them (56.7%) were women and the patients’ mean age was 66.58 ± 17.86 years. Suggestive measures of TL were found in 59.7% of the patients, being "withhold of life-support measures" the most important (35.8%), followed by DNR (17.9%) and "withdrawal of life-support measures" (6%). The procedures most commonly omitted were use of vasoactive drugs and dialysis, while antibiotics were the most discontinued. The use of TL measures was more frequent in clinical patients. CONCLUSIONS: The results of the present study suggest high frequencies of medical conducts suggestive of TL in a general ICU in Northeast of Brazil. Therapeutic methods that could cause discomfort or suffering to the patients, as nutrition, sedation and analgesia, were rarely omitted or discontinued.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):137-143
DOI 10.1590/S0103-507X2007000200001
BACKGROUND AND OBJECTIVES: There is a growing tendency of looking for "dying with dignity", rather than to prolong death and suffering of terminal patients on intensive care units (ICU). This study aims to evaluate medical practices that suggest therapeutic limitation (TL) in patients who died in an adult ICU. METHODS: A retrospective exploratory study was carried out to evaluate medical records of patients who died in a general adult ICU of a private hospital in Salvador-BA, between January and August of 2003, after at least 24 hours from the admission. The patients were classified, in relation to their deaths, in: "not responding to cardiopulmonary resuscitation", "brain death", "decision not to resuscitate" (DNR) and "withhold or withdrawal life-support measures". RESULTS: Sixty seven patients were included, corresponding to 90.4% of the deaths occurred in this ICU during the referred period. The most of them (56.7%) were women and the patients’ mean age was 66.58 ± 17.86 years. Suggestive measures of TL were found in 59.7% of the patients, being "withhold of life-support measures" the most important (35.8%), followed by DNR (17.9%) and "withdrawal of life-support measures" (6%). The procedures most commonly omitted were use of vasoactive drugs and dialysis, while antibiotics were the most discontinued. The use of TL measures was more frequent in clinical patients. CONCLUSIONS: The results of the present study suggest high frequencies of medical conducts suggestive of TL in a general ICU in Northeast of Brazil. Therapeutic methods that could cause discomfort or suffering to the patients, as nutrition, sedation and analgesia, were rarely omitted or discontinued.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):151-160
DOI 10.1590/S0103-507X2007000200003
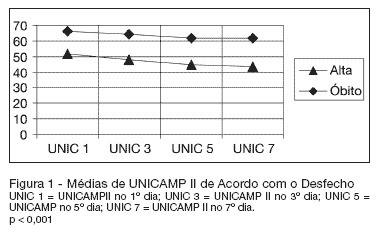
BACKGROUND AND OBJECTIVES: Currently, the reformulation of intensive care goals, often shifting from the search for a cure to offering comfort, has become more and more necessary. The intensivist is frequently confronted with the decision to suspend or not offer a specific therapy, despite its availability. The objective of this study was to estimate the developing risk of probability of death for individual ICU patients with respiratory failure, identify which life-sustaining therapies were administered, time of internment and outcome. Compare the death outcome in relation to UNICAMP II and APACHE II models, as well as verify if the life-sustaining therapies may be limited or suspended. METHODS: It is the observational, prospective cohort study of 150 patients with respiratory failure confined to the intensive care unit. Statistical analysis was carried out using Generalized Linear Models. RESULTS: Age, sex, race or morbidity did not reveal statistical significance in predicting outcome. This prediction was confirmed more accurately by means of changes in the individual prognostic index of death probability during the first seven days of ICU internment. A 10% worsening prognosis in patients who presented initial death risk of 70% to 80%, utilizing the UNICAMP II Model, showed a specificity of 97.4% - 98.6%. CONCLUSIONS: Prognostic changes in patients during the first seven days of ICU internment are of great aid, from an objective point of view, for ethical decision-making in relation to not-offering new life-sustaining therapies.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):151-160
DOI 10.1590/S0103-507X2007000200003
BACKGROUND AND OBJECTIVES: Currently, the reformulation of intensive care goals, often shifting from the search for a cure to offering comfort, has become more and more necessary. The intensivist is frequently confronted with the decision to suspend or not offer a specific therapy, despite its availability. The objective of this study was to estimate the developing risk of probability of death for individual ICU patients with respiratory failure, identify which life-sustaining therapies were administered, time of internment and outcome. Compare the death outcome in relation to UNICAMP II and APACHE II models, as well as verify if the life-sustaining therapies may be limited or suspended. METHODS: It is the observational, prospective cohort study of 150 patients with respiratory failure confined to the intensive care unit. Statistical analysis was carried out using Generalized Linear Models. RESULTS: Age, sex, race or morbidity did not reveal statistical significance in predicting outcome. This prediction was confirmed more accurately by means of changes in the individual prognostic index of death probability during the first seven days of ICU internment. A 10% worsening prognosis in patients who presented initial death risk of 70% to 80%, utilizing the UNICAMP II Model, showed a specificity of 97.4% - 98.6%. CONCLUSIONS: Prognostic changes in patients during the first seven days of ICU internment are of great aid, from an objective point of view, for ethical decision-making in relation to not-offering new life-sustaining therapies.