respiratory failure Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
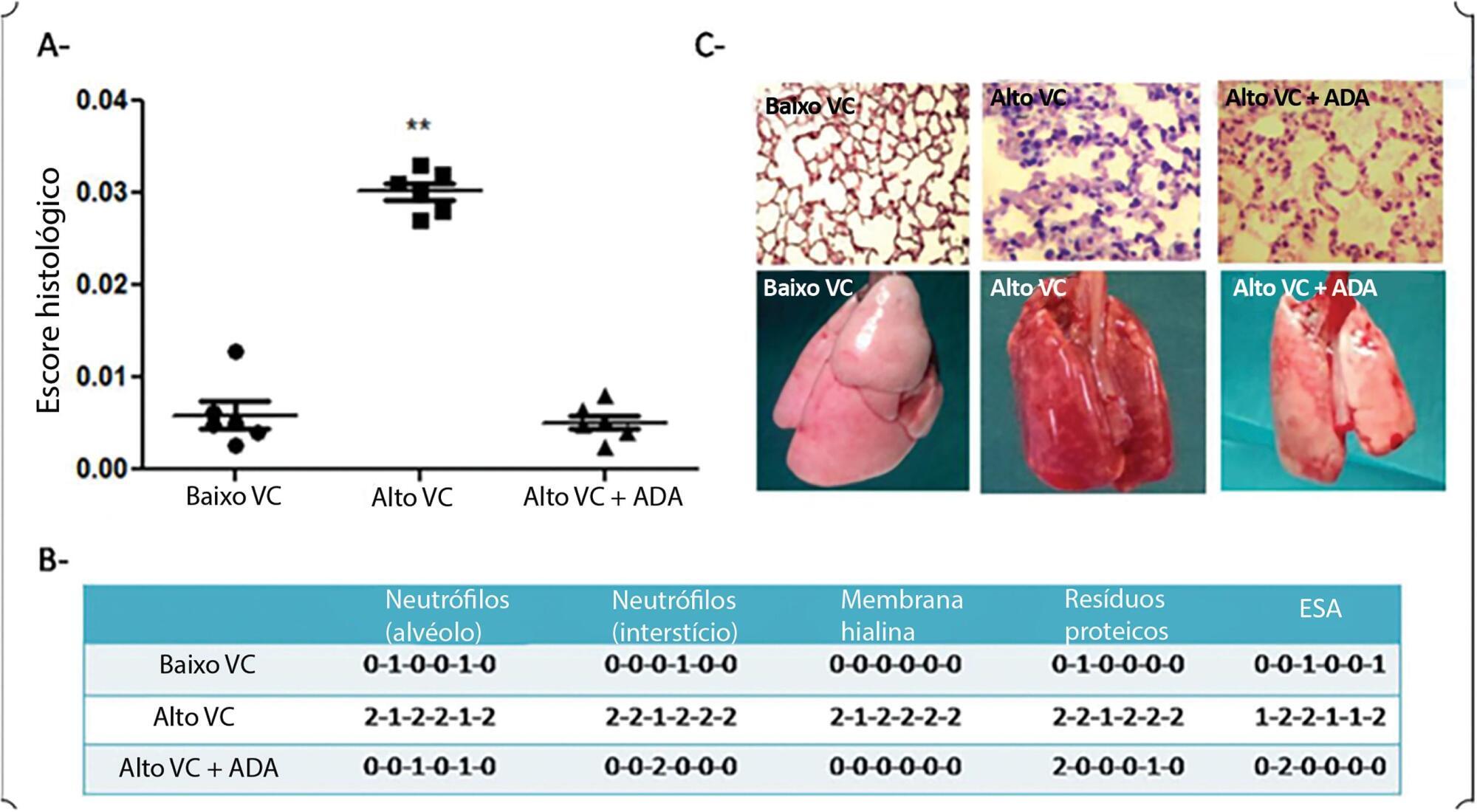
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
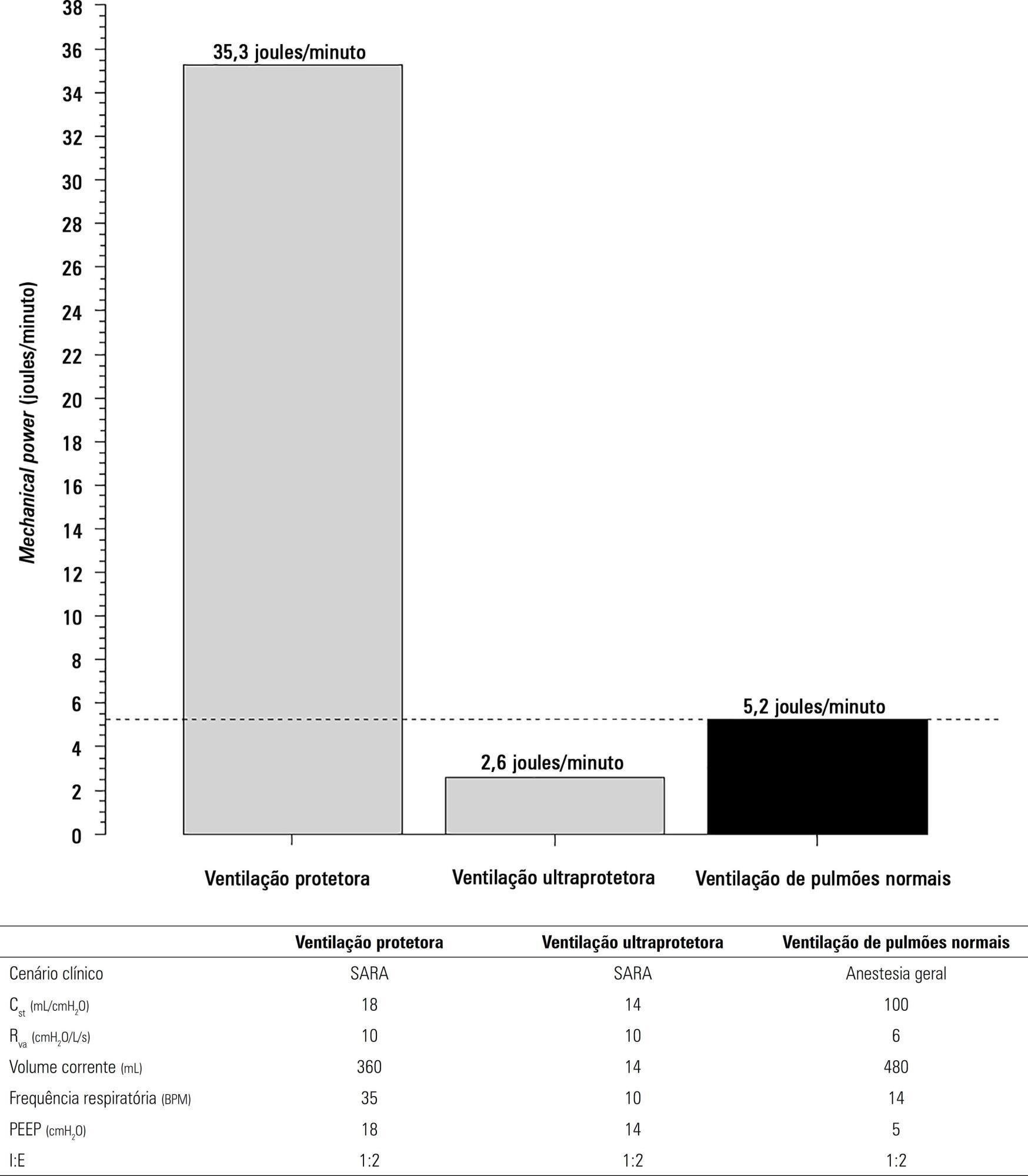
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Mathematical modeling approach with hypothetical scenarios using computer simulation.
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Mathematical modeling approach with hypothetical scenarios using computer simulation.
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
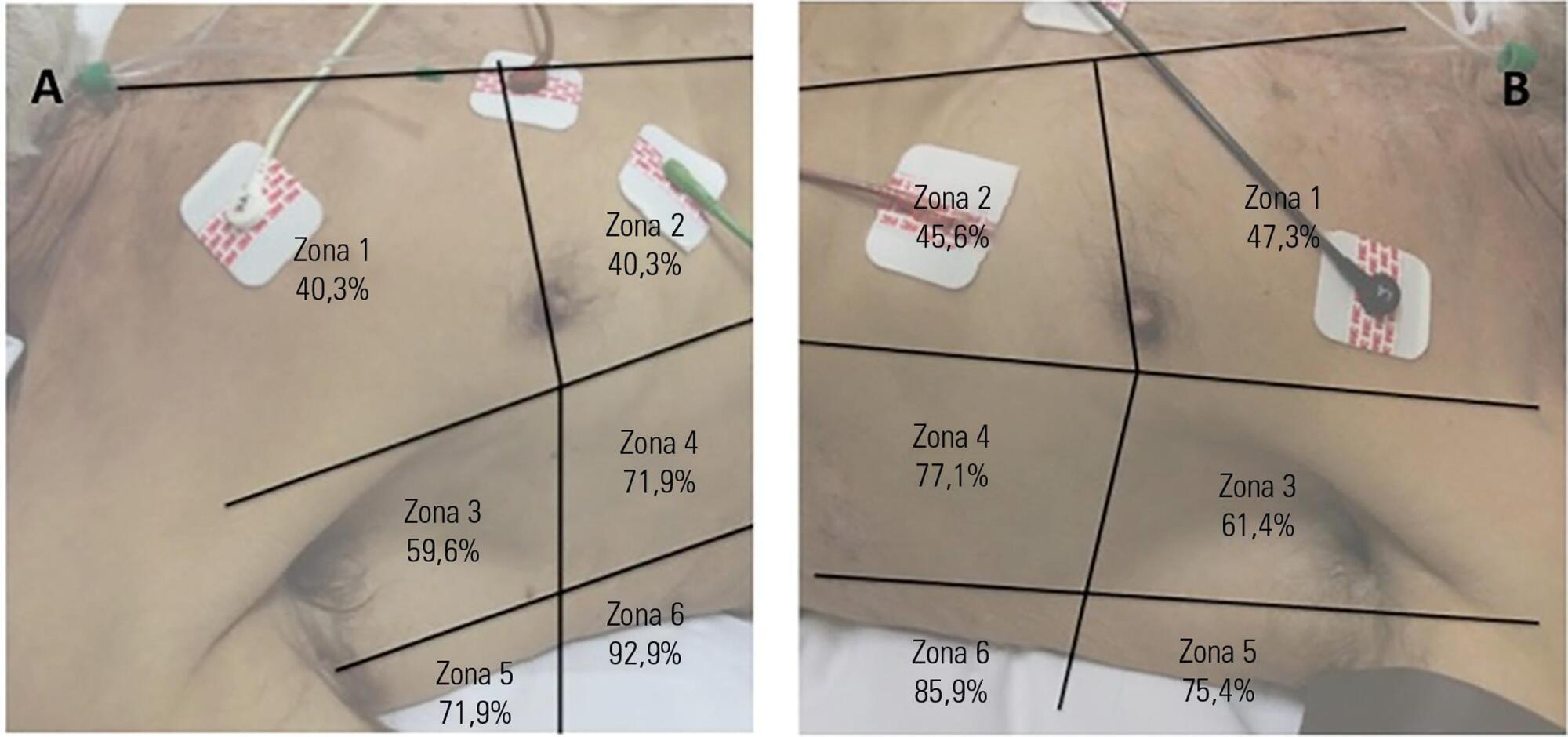
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
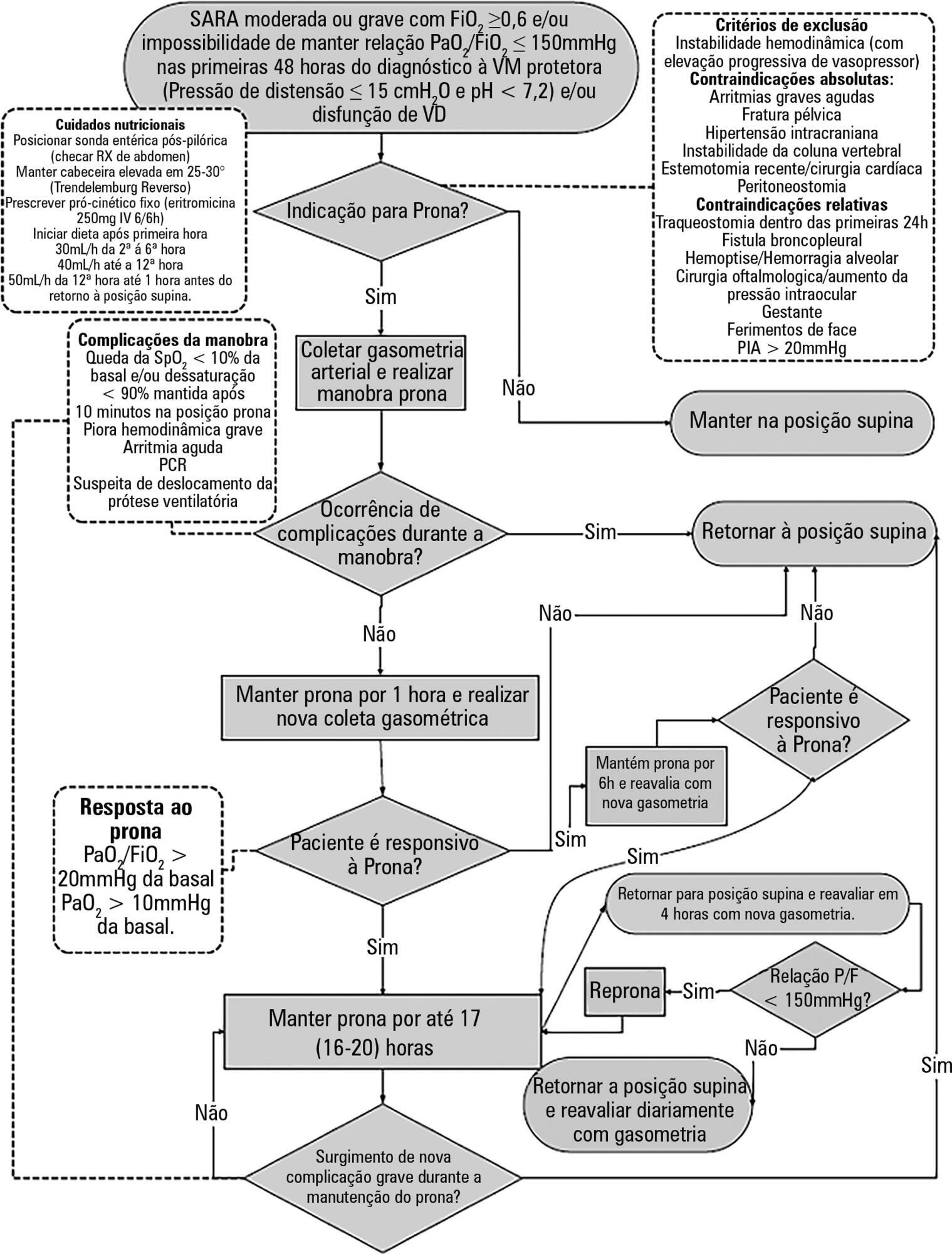
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team's understanding of the tool's importance to patient safety and training in its use are necessary for its success.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team's understanding of the tool's importance to patient safety and training in its use are necessary for its success.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
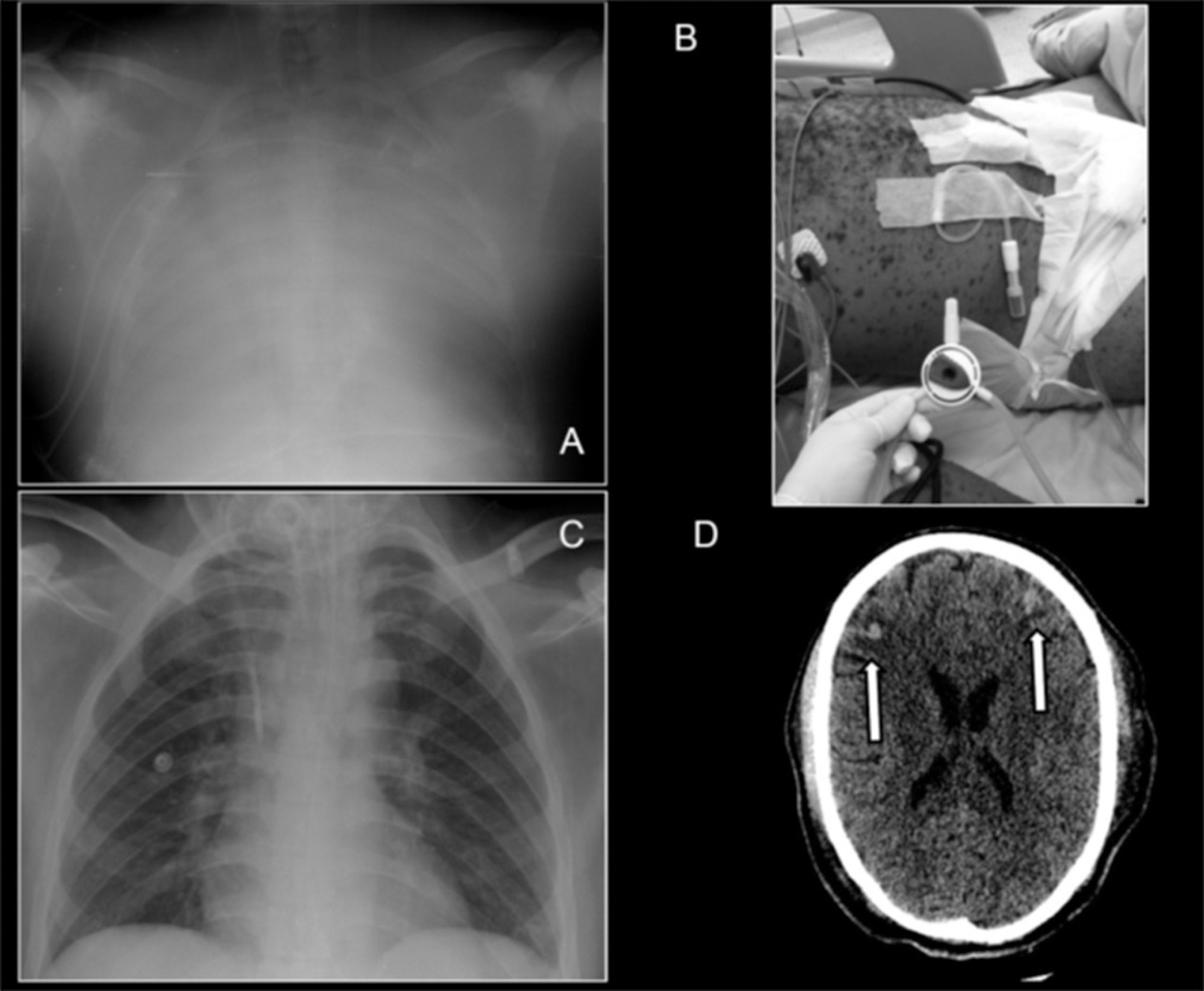
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.

Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation's causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):151-160
DOI 10.1590/S0103-507X2007000200003
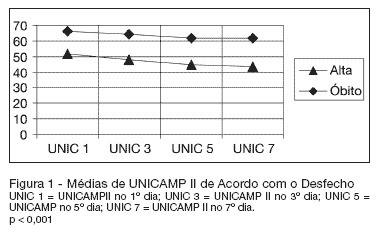
BACKGROUND AND OBJECTIVES: Currently, the reformulation of intensive care goals, often shifting from the search for a cure to offering comfort, has become more and more necessary. The intensivist is frequently confronted with the decision to suspend or not offer a specific therapy, despite its availability. The objective of this study was to estimate the developing risk of probability of death for individual ICU patients with respiratory failure, identify which life-sustaining therapies were administered, time of internment and outcome. Compare the death outcome in relation to UNICAMP II and APACHE II models, as well as verify if the life-sustaining therapies may be limited or suspended. METHODS: It is the observational, prospective cohort study of 150 patients with respiratory failure confined to the intensive care unit. Statistical analysis was carried out using Generalized Linear Models. RESULTS: Age, sex, race or morbidity did not reveal statistical significance in predicting outcome. This prediction was confirmed more accurately by means of changes in the individual prognostic index of death probability during the first seven days of ICU internment. A 10% worsening prognosis in patients who presented initial death risk of 70% to 80%, utilizing the UNICAMP II Model, showed a specificity of 97.4% - 98.6%. CONCLUSIONS: Prognostic changes in patients during the first seven days of ICU internment are of great aid, from an objective point of view, for ethical decision-making in relation to not-offering new life-sustaining therapies.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):151-160
DOI 10.1590/S0103-507X2007000200003
BACKGROUND AND OBJECTIVES: Currently, the reformulation of intensive care goals, often shifting from the search for a cure to offering comfort, has become more and more necessary. The intensivist is frequently confronted with the decision to suspend or not offer a specific therapy, despite its availability. The objective of this study was to estimate the developing risk of probability of death for individual ICU patients with respiratory failure, identify which life-sustaining therapies were administered, time of internment and outcome. Compare the death outcome in relation to UNICAMP II and APACHE II models, as well as verify if the life-sustaining therapies may be limited or suspended. METHODS: It is the observational, prospective cohort study of 150 patients with respiratory failure confined to the intensive care unit. Statistical analysis was carried out using Generalized Linear Models. RESULTS: Age, sex, race or morbidity did not reveal statistical significance in predicting outcome. This prediction was confirmed more accurately by means of changes in the individual prognostic index of death probability during the first seven days of ICU internment. A 10% worsening prognosis in patients who presented initial death risk of 70% to 80%, utilizing the UNICAMP II Model, showed a specificity of 97.4% - 98.6%. CONCLUSIONS: Prognostic changes in patients during the first seven days of ICU internment are of great aid, from an objective point of view, for ethical decision-making in relation to not-offering new life-sustaining therapies.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)