Pulmonary Ventilation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.

Abstract
Rev Bras Ter Intensiva. 2016;28(1):27-32
DOI 10.5935/0103-507X.20160010
To determine the efficacy of lung hyperinflation maneuvers via a mechanical ventilator compared to isolated tracheal aspiration for removing secretions, normalizing hemodynamics and improving lung mechanics in patients on mechanical ventilation.
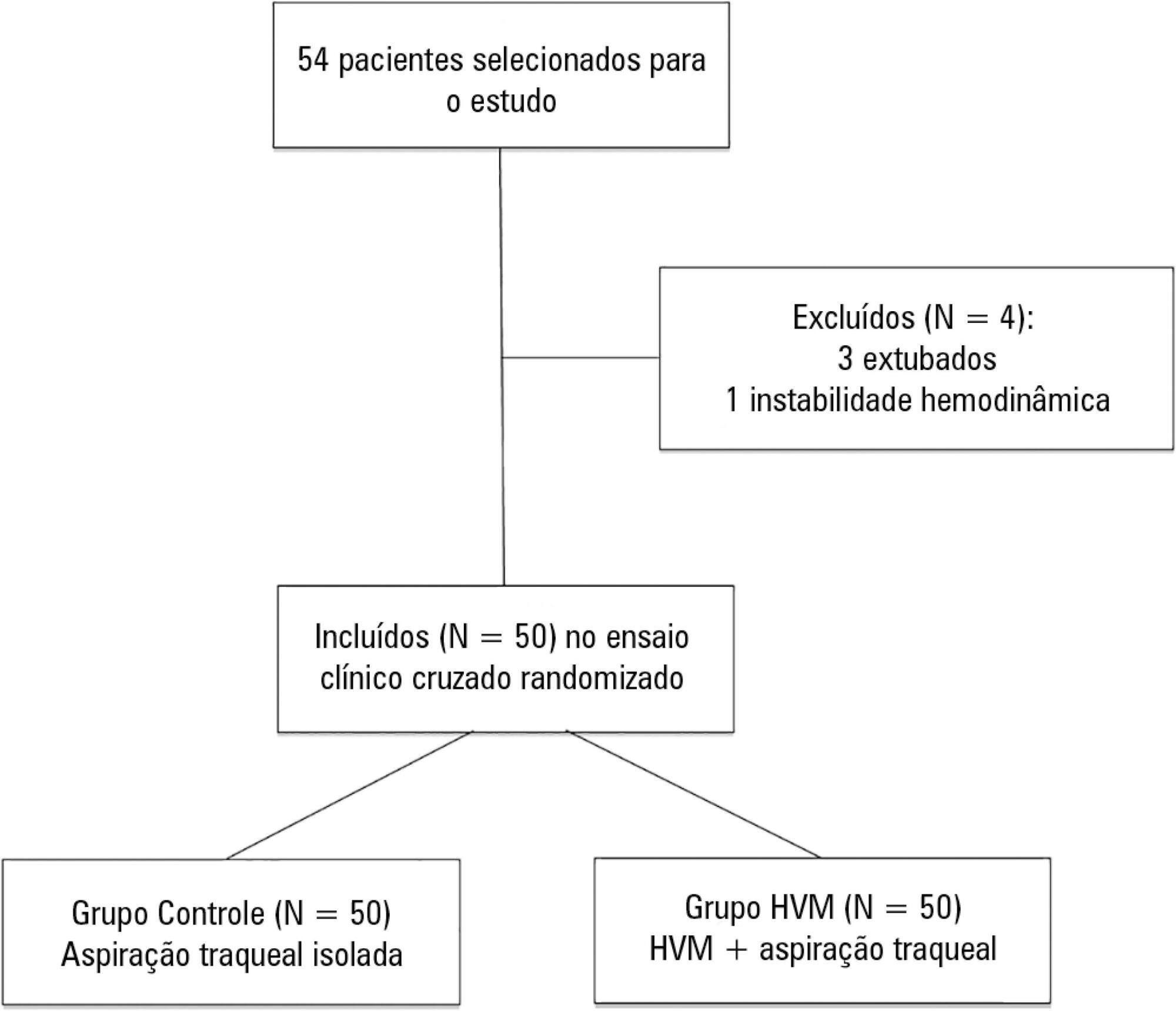
This was a randomized crossover clinical trial including patients admitted to the intensive care unit and on mechanical ventilation for more than 48 hours. Patients were randomized to receive either isolated tracheal aspiration (Control Group) or lung hyperinflation by mechanical ventilator (MVH Group). Hemodynamic and mechanical respiratory parameters were measured along with the amount of aspirated secretions.
A total of 50 patients were included. The mean age of the patients was 44.7 ± 21.6 years, and 31 were male. Compared to the Control Group, the MVH Group showed greater aspirated secretion amount (3.9g versus 6.4g, p = 0.0001), variation in mean dynamic compliance (-1.3 ± 2.3 versus -2.9 ± 2.3; p = 0.008), and expired tidal volume (-0.7 ± 0.0 versus -54.1 ± 38.8, p = 0.0001) as well as a significant decrease in peak inspiratory pressure (0.2 ± 0.1 versus 2.5 ± 0.1; p = 0.001).
In the studied sample, the MVH technique led to a greater amount of aspirated secretions, significant increases in dynamic compliance and expired tidal volume and a significant reduction in peak inspiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):27-32
DOI 10.5935/0103-507X.20160010
To determine the efficacy of lung hyperinflation maneuvers via a mechanical ventilator compared to isolated tracheal aspiration for removing secretions, normalizing hemodynamics and improving lung mechanics in patients on mechanical ventilation.
This was a randomized crossover clinical trial including patients admitted to the intensive care unit and on mechanical ventilation for more than 48 hours. Patients were randomized to receive either isolated tracheal aspiration (Control Group) or lung hyperinflation by mechanical ventilator (MVH Group). Hemodynamic and mechanical respiratory parameters were measured along with the amount of aspirated secretions.
A total of 50 patients were included. The mean age of the patients was 44.7 ± 21.6 years, and 31 were male. Compared to the Control Group, the MVH Group showed greater aspirated secretion amount (3.9g versus 6.4g, p = 0.0001), variation in mean dynamic compliance (-1.3 ± 2.3 versus -2.9 ± 2.3; p = 0.008), and expired tidal volume (-0.7 ± 0.0 versus -54.1 ± 38.8, p = 0.0001) as well as a significant decrease in peak inspiratory pressure (0.2 ± 0.1 versus 2.5 ± 0.1; p = 0.001).
In the studied sample, the MVH technique led to a greater amount of aspirated secretions, significant increases in dynamic compliance and expired tidal volume and a significant reduction in peak inspiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.

Abstract
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
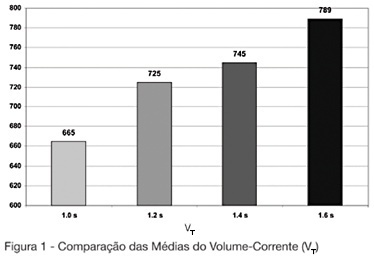
BACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
BACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.