
You searched for:"Sílvia Regina Rios Vieira"
We found (13) results for your search.-
Original Article
SAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
- Valeska Fernandes Pasinato
 ,
, - Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto, [ … ],
- Silvia Regina Rios Vieira
Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee moreViews2

Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee more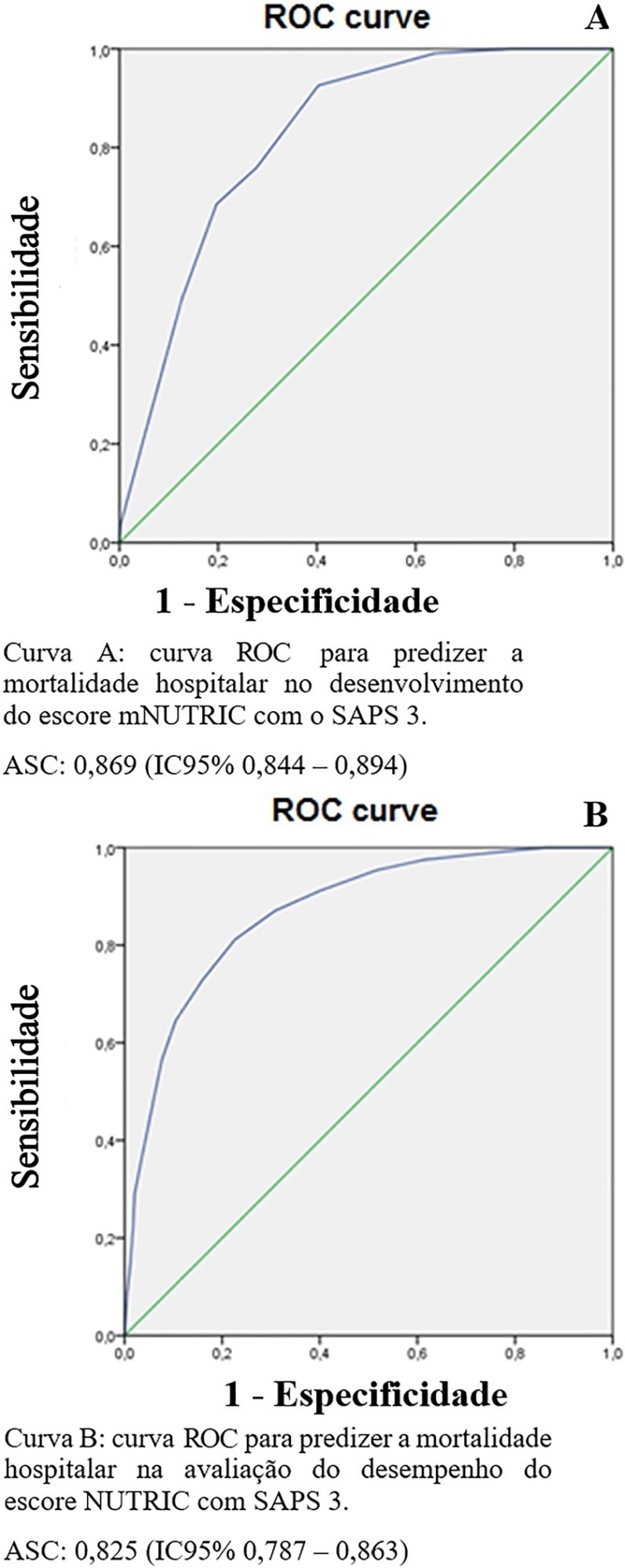
- Valeska Fernandes Pasinato
-
Original Article
Changes in cardiac arrest profiles after the implementation of a Rapid Response Team
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres, [ … ],
- Marcio Manozzo Boniatti
Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
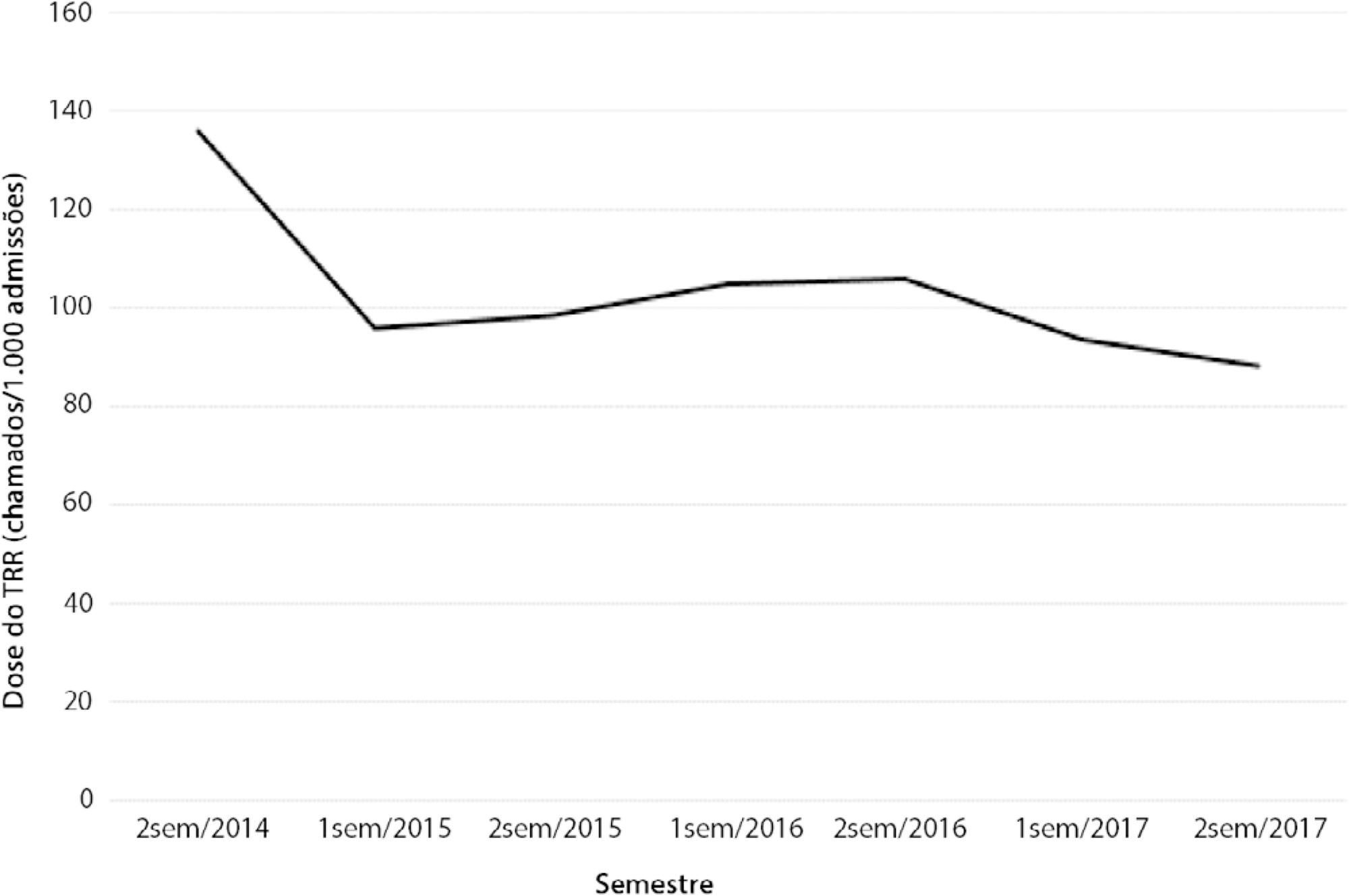
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Views1Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
- Marina Verçoza Viana
-
Original Article
Comparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
Abstract
Original ArticleComparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
DOI 10.5935/0103-507X.20190005
Views1ABSTRACT
Objective:
To compare the effects of vibrocompression and hyperinflation with mechanical ventilator techniques alone and in combination (hyperinflation with mechanical ventilator + vibrocompression) on the amount of aspirated secretion and the change in hemodynamic and pulmonary parameters.
Methods:
A randomized clinical trial with critically ill patients on mechanical ventilation conducted in the intensive care unit of a university hospital. The patients were randomly allocated to receive one of the bronchial hygiene techniques for 10 minutes (vibrocompression or hyperinflation with mechanical ventilator or hyperinflation with mechanical ventilator + vibrocompression). Afterwards, the patients were again randomly allocated to receive either the previous randomly allocated technique or only tracheal aspiration. The weight of aspirated secretions (in grams), ventilatory mechanics and cardiopulmonary data before and after the application of the techniques were analyzed. The tracheal reintubation frequency and time and mortality on mechanical ventilation were also evaluated.
Results:
A total of 93 patients (29 vibrocompression, 32 hyperinflation with mechanical ventilator and 32 hyperinflation with mechanical ventilator + vibrocompression) on mechanical ventilation for more than 24 hours were included. The hyperinflation with mechanical ventilator + vibrocompression group was the only one that presented a significant increase in aspirated secretions compared to tracheal aspiration alone [0.7g (0.1 – 2.5g) versus 0.2g (0.0 – 0.6g), p value = 0.006].
Conclusion:
Compared to tracheal aspiration alone, the combination of hyperinflation with mechanical ventilator + vibrocompression techniques was most efficient for increasing the amount of aspirated secretions.
Keywords:Bronchoalveolar lavageHygieneInsufflationPhysical therapy modalitiesRespiratory aspirationVentilators, mechanicalSee moreViews1Abstract
Original ArticleComparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
DOI 10.5935/0103-507X.20190005
Views1ABSTRACT
Objective:
To compare the effects of vibrocompression and hyperinflation with mechanical ventilator techniques alone and in combination (hyperinflation with mechanical ventilator + vibrocompression) on the amount of aspirated secretion and the change in hemodynamic and pulmonary parameters.
Methods:
A randomized clinical trial with critically ill patients on mechanical ventilation conducted in the intensive care unit of a university hospital. The patients were randomly allocated to receive one of the bronchial hygiene techniques for 10 minutes (vibrocompression or hyperinflation with mechanical ventilator or hyperinflation with mechanical ventilator + vibrocompression). Afterwards, the patients were again randomly allocated to receive either the previous randomly allocated technique or only tracheal aspiration. The weight of aspirated secretions (in grams), ventilatory mechanics and cardiopulmonary data before and after the application of the techniques were analyzed. The tracheal reintubation frequency and time and mortality on mechanical ventilation were also evaluated.
Results:
A total of 93 patients (29 vibrocompression, 32 hyperinflation with mechanical ventilator and 32 hyperinflation with mechanical ventilator + vibrocompression) on mechanical ventilation for more than 24 hours were included. The hyperinflation with mechanical ventilator + vibrocompression group was the only one that presented a significant increase in aspirated secretions compared to tracheal aspiration alone [0.7g (0.1 – 2.5g) versus 0.2g (0.0 – 0.6g), p value = 0.006].
Conclusion:
Compared to tracheal aspiration alone, the combination of hyperinflation with mechanical ventilator + vibrocompression techniques was most efficient for increasing the amount of aspirated secretions.
Keywords:Bronchoalveolar lavageHygieneInsufflationPhysical therapy modalitiesRespiratory aspirationVentilators, mechanicalSee more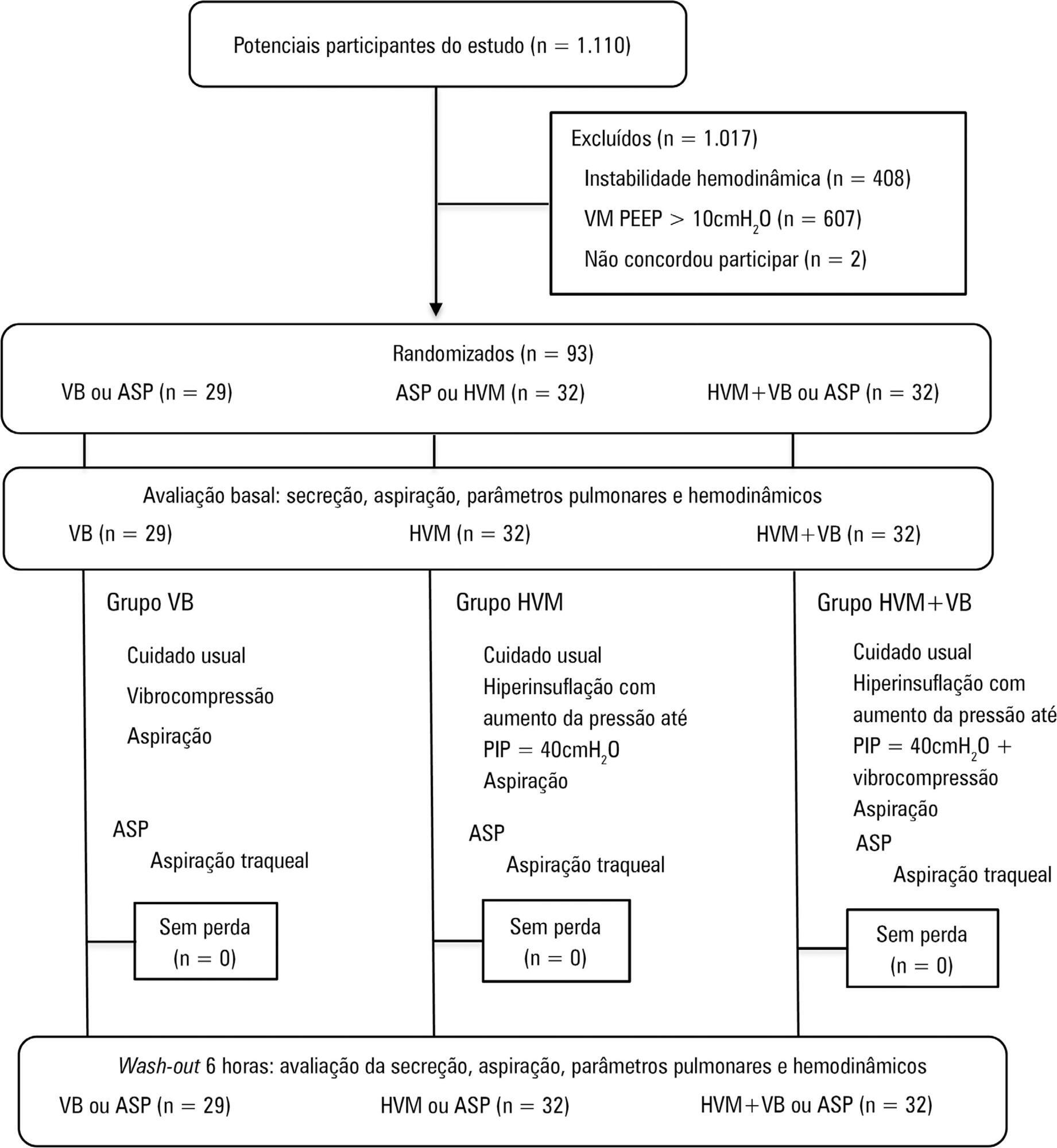
-
Original Article
Quality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
Abstract
Original ArticleQuality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
Views0ABSTRACT
Objective:
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
Methods:
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
Discussion:
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Keywords:AnxietyCognitive dysfunctionCritical care outcomesDepressionDisabled personsQuality of lifeStress disorders, PosttraumaticSee moreViews0Abstract
Original ArticleQuality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
Views0ABSTRACT
Objective:
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
Methods:
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
Discussion:
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Keywords:AnxietyCognitive dysfunctionCritical care outcomesDepressionDisabled personsQuality of lifeStress disorders, PosttraumaticSee more
-
Original Articles
Acute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
Abstract
Original ArticlesAcute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
DOI 10.5935/0103-507X.20170004
Views1See moreABSTRACT
Objective:
To evaluate the effects of bag-valve breathing maneuvers combined with standard manual chest compression techniques on safety, hemodynamics and oxygenation in stable septic shock patients.
Design:
A parallel, assessor-blinded, randomized trial of two groups. A computer-generated list of random numbers was prepared by an independent researcher to allocate treatments.
Setting:
The Intensive Care Unit at Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul.
Participants:
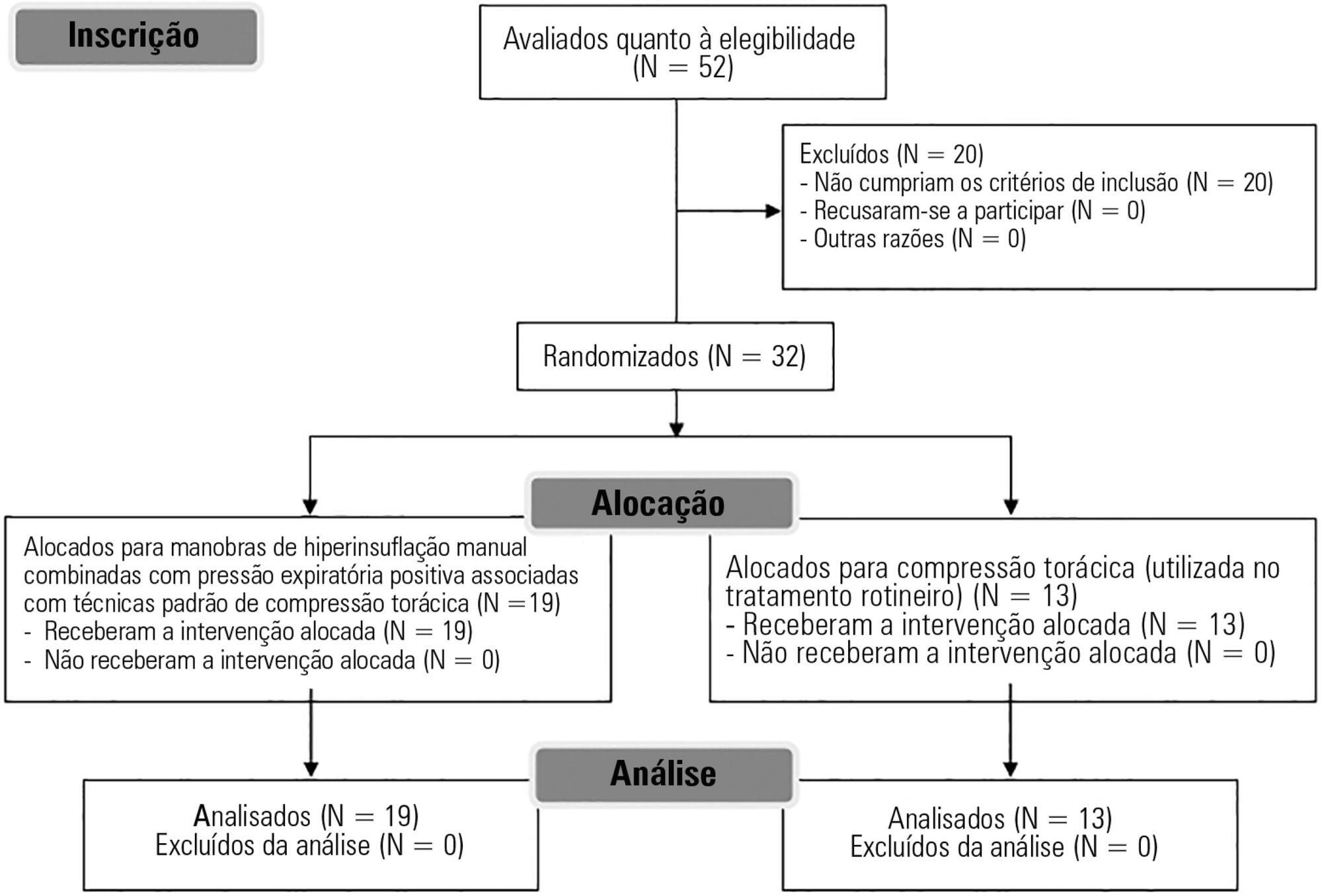
Fifty-two subjects were assessed for eligibility, and 32 were included. All included subjects (n = 32) received the allocated intervention (n = 19 for the Experimental Group and n = 13 for the Control Group).
Intervention:
Twenty minutes of bag-valve breathing maneuvers combined with manual chest compression techniques (Experimental Group) or chest compression, as routinely used at our intensive care unit (Control Group). Follow-up was performed immediately after and at 30 minutes after the intervention.
Main outcome measure:
Mean artery pressure.
Results:
All included subjects completed the trial (N = 32). We found no relevant effects on mean artery pressure (p = 0.17), heart rate (p = 0.50) or mean pulmonary artery pressure (p = 0.89) after adjusting for subject age and weight. Both groups were identical regarding oxygen consumption after the data adjustment (p = 0.84). Peripheral oxygen saturation tended to increase over time in both groups (p = 0.05), and there was no significant association between cardiac output and venous oxygen saturation (p = 0.813). No clinical deterioration was observed.
Conclusion:
A single session of bag-valve breathing maneuvers combined with manual chest compression is hemodynamically safe for stable septic-shocked subjects over the short-term.
Views1Abstract
Original ArticlesAcute bag-valve breathing maneuvers plus manual chest compression is safe during stable septic shock: a randomized clinical trial
Rev Bras Ter Intensiva. 2017;29(1):14-22
DOI 10.5935/0103-507X.20170004
Views1See moreABSTRACT
Objective:
To evaluate the effects of bag-valve breathing maneuvers combined with standard manual chest compression techniques on safety, hemodynamics and oxygenation in stable septic shock patients.
Design:
A parallel, assessor-blinded, randomized trial of two groups. A computer-generated list of random numbers was prepared by an independent researcher to allocate treatments.
Setting:
The Intensive Care Unit at Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul.
Participants:
Fifty-two subjects were assessed for eligibility, and 32 were included. All included subjects (n = 32) received the allocated intervention (n = 19 for the Experimental Group and n = 13 for the Control Group).
Intervention:
Twenty minutes of bag-valve breathing maneuvers combined with manual chest compression techniques (Experimental Group) or chest compression, as routinely used at our intensive care unit (Control Group). Follow-up was performed immediately after and at 30 minutes after the intervention.
Main outcome measure:
Mean artery pressure.
Results:
All included subjects completed the trial (N = 32). We found no relevant effects on mean artery pressure (p = 0.17), heart rate (p = 0.50) or mean pulmonary artery pressure (p = 0.89) after adjusting for subject age and weight. Both groups were identical regarding oxygen consumption after the data adjustment (p = 0.84). Peripheral oxygen saturation tended to increase over time in both groups (p = 0.05), and there was no significant association between cardiac output and venous oxygen saturation (p = 0.813). No clinical deterioration was observed.
Conclusion:
A single session of bag-valve breathing maneuvers combined with manual chest compression is hemodynamically safe for stable septic-shocked subjects over the short-term.
-
Special Article
Safe prone checklist: construction and implementation of a tool for performing the prone maneuver
Rev Bras Ter Intensiva. 2017;29(2):131-141
Abstract
Special ArticleSafe prone checklist: construction and implementation of a tool for performing the prone maneuver
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
Views0ABSTRACT
Objective:
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
Methods:
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
Results:
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
Conclusion:
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team’s understanding of the tool’s importance to patient safety and training in its use are necessary for its success.
Keywords:Check listInservice trainingPatient safetyPronation/methodsProne position/methodsRespiratory distress syndrome, adultrespiratory failureSee moreViews0Abstract
Special ArticleSafe prone checklist: construction and implementation of a tool for performing the prone maneuver
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
Views0ABSTRACT
Objective:
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
Methods:
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
Results:
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
Conclusion:
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team’s understanding of the tool’s importance to patient safety and training in its use are necessary for its success.
Keywords:Check listInservice trainingPatient safetyPronation/methodsProne position/methodsRespiratory distress syndrome, adultrespiratory failureSee more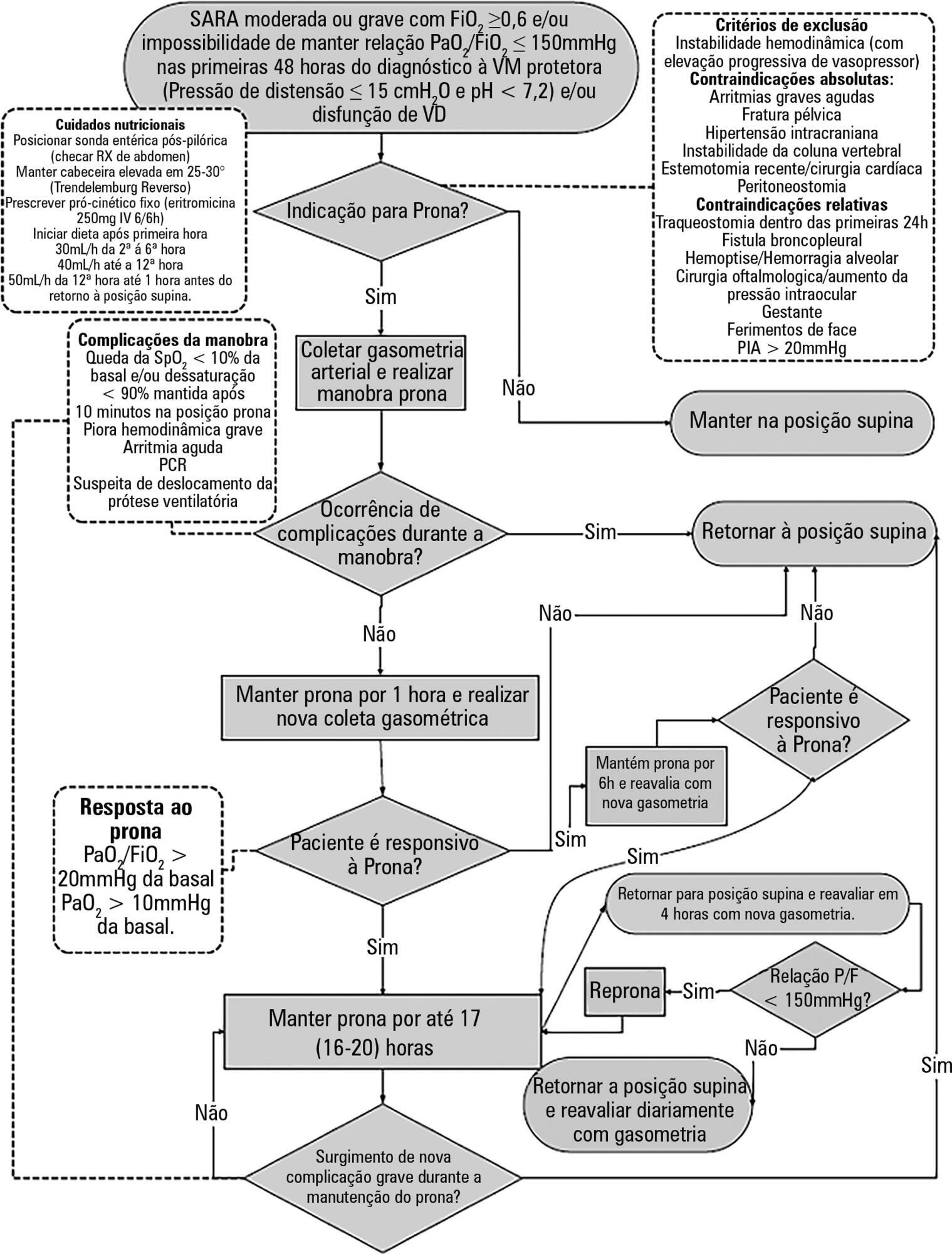
-
Review Articles
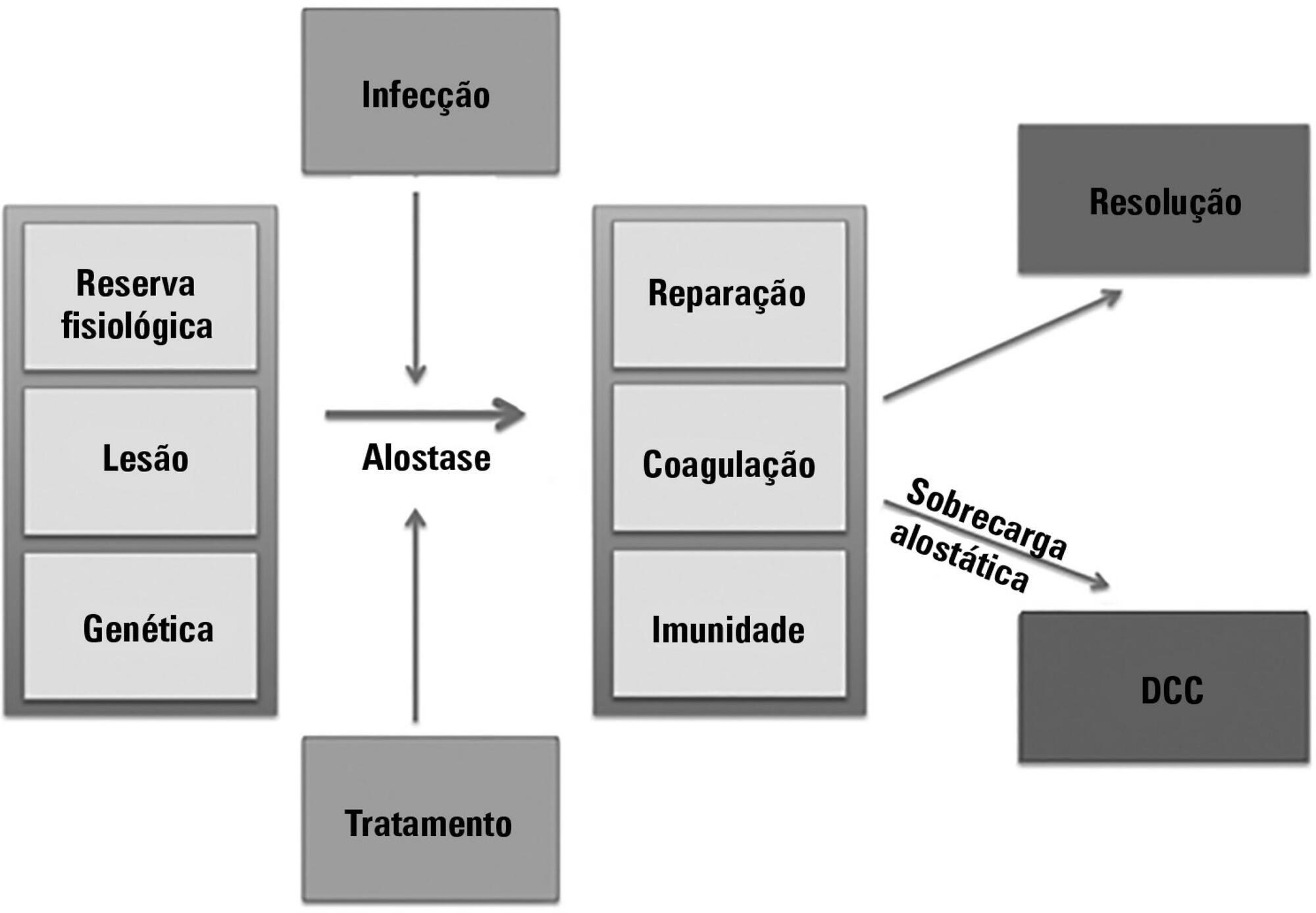
Chronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Views1Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis