Quality of life Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
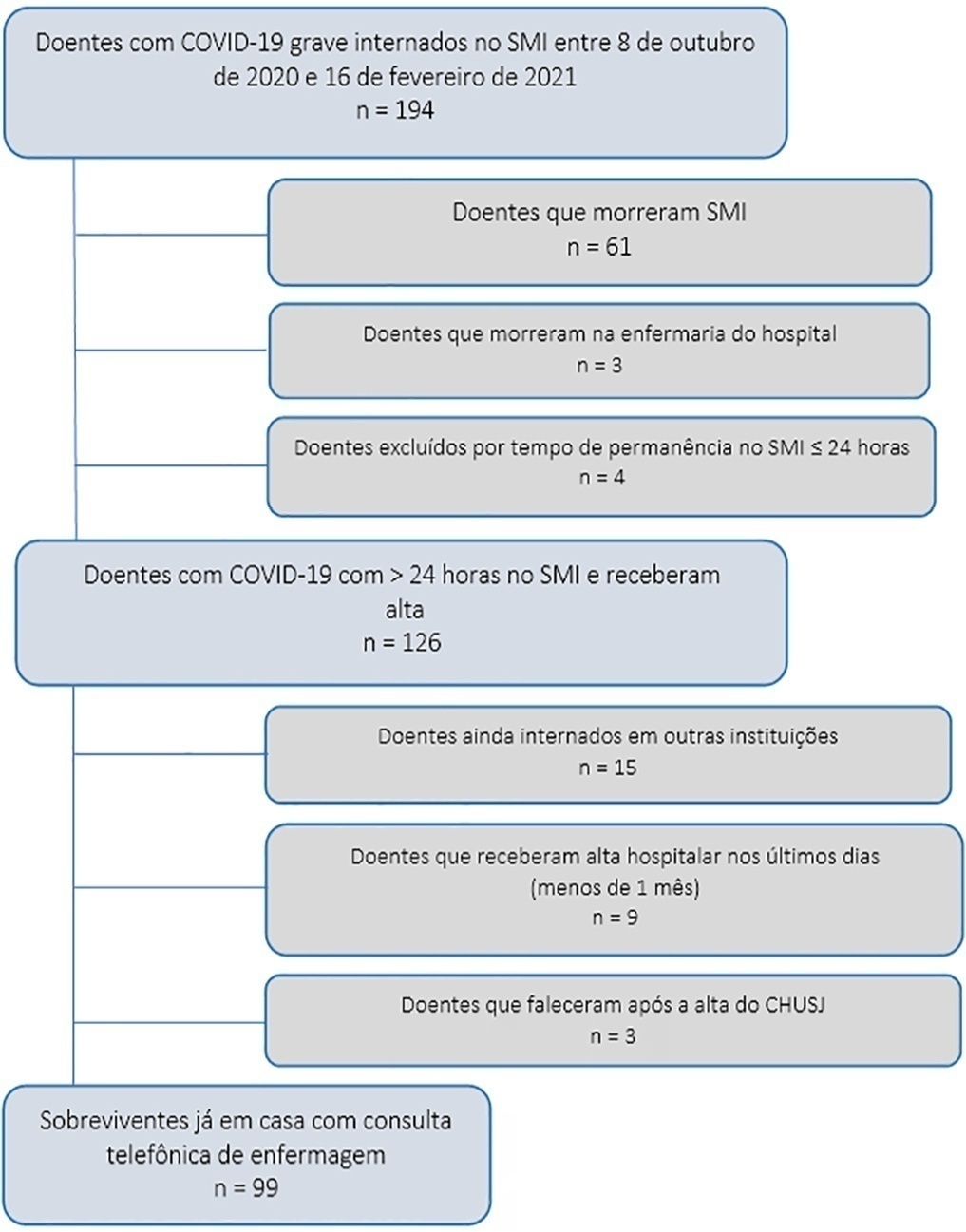
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):141-146
DOI 10.5935/0103-507X.20220008-en
To assess early postdischarge health-related quality of life and disability of all survivors of critical COVID-19 admitted for more than 24 hours to na intensive care unit..
Study carried out at the Intensive Care Medicine Department of Centro Hospitalar Universitário São João from 8th October 2020 to 16th February 2021. Approximately 1 month after hospital discharge, an intensive care-trained nurse performed a telephone consultation with 99 survivors already at home applying the EuroQol Five-Dimensional Five-Level questionnaire and the 12-item World Health Organization Disability Assessment Schedule 2.0.
The mean age of the population studied was 63 ± 12 years, and 32.5% were submitted to invasive mechanical ventilation. Their mean Simplified Acute Physiologic Score was 35 ± 14, and the Charlson Comorbidity Index was 3 ± 2. Intensive care medicine and hospital lengths of stay were 13 ± 22 and 22 ± 25 days, respectively. The mean EuroQol Visual Analog Scale was 65% (± 21), and only 35.3% had no or slight problems performing their usual activities, most having some degree of pain/discomfort and anxiety/depression. The 12-item World Health Organization Disability Assessment Schedule 2.0 showed marked impairments in terms of reassuring usual work or community activities and mobility. The use of both tools suggested that their health status was worse than their perception of it.
This early identification of sequelae may help define flows and priorities for rehabilitation and reinsertion after critical COVID-19.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
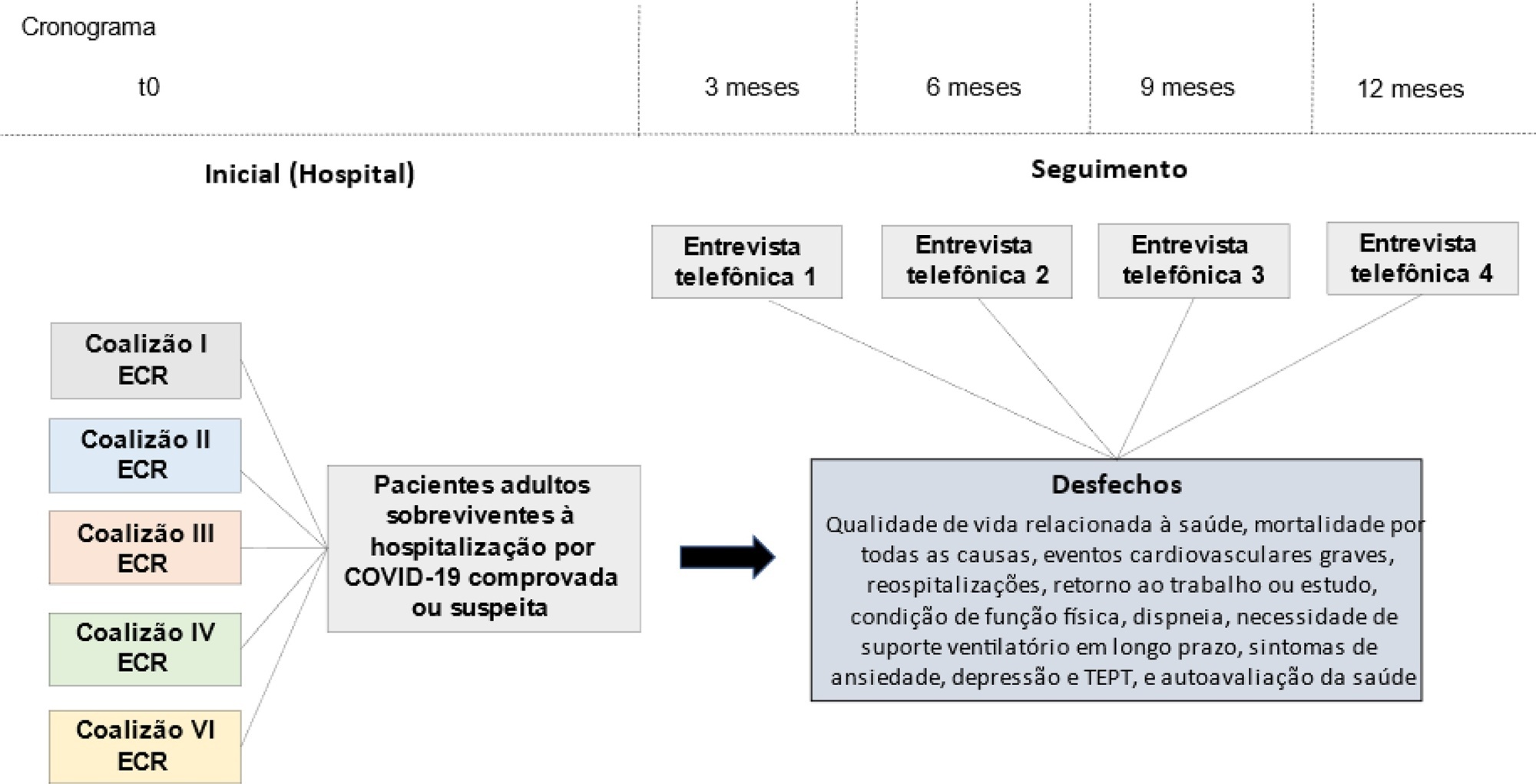
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):426-432
DOI 10.5935/0103-507X.20200072
To evaluate the association between the incidence of delirium in the intensive care unit and quality of life 1 month after hospital discharge.
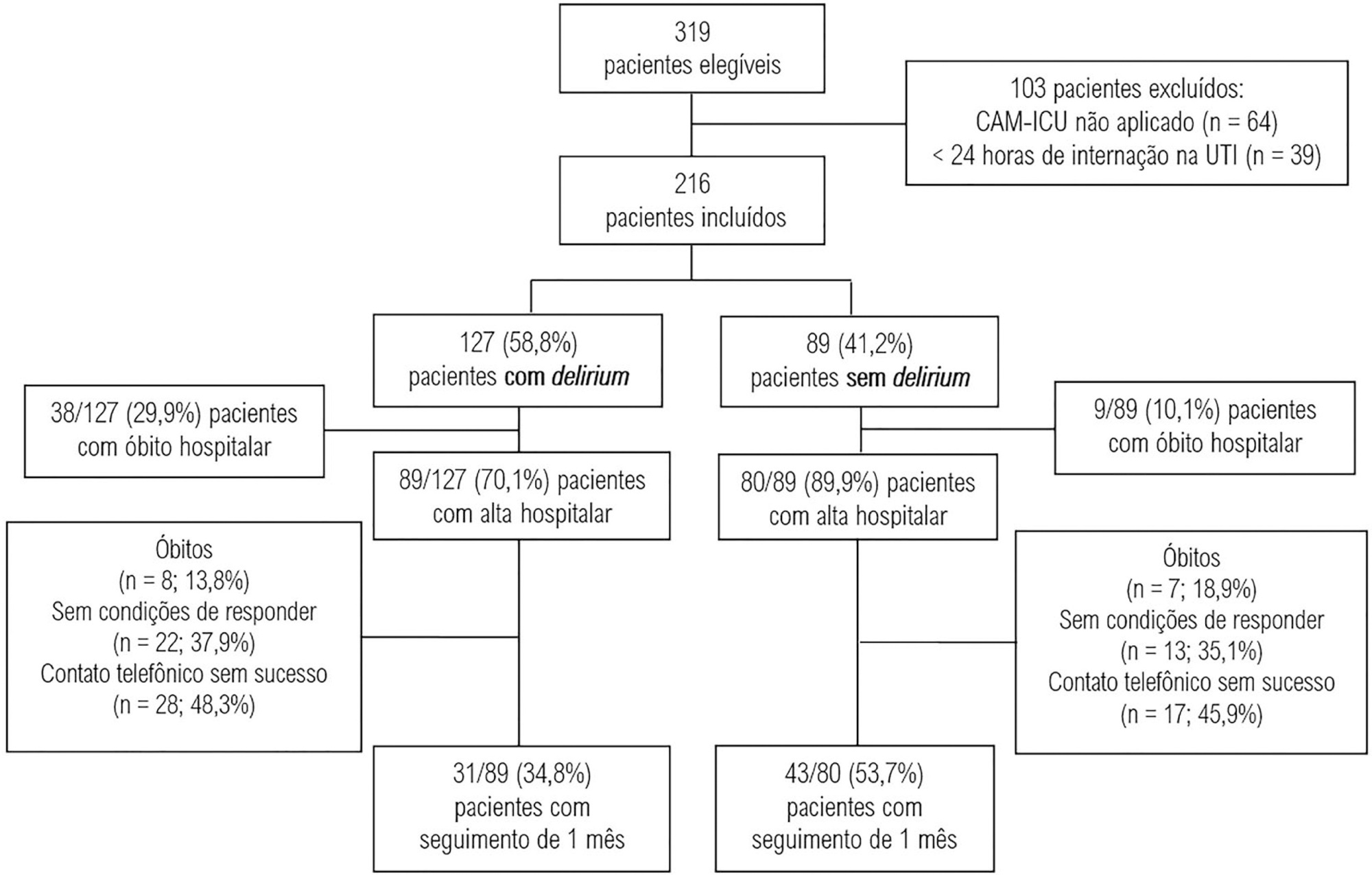
This was a prospective cohort study conducted in the intensive care units of two medium-complexity hospitals from December 2015 to December 2016. Delirium was identified using the Confusion Assessment Method for the Intensive Care Unit scale. At the time of hospital discharge, functional capacity and cognition were assessed with the Barthel index and the Mini Mental State Examination, respectively. Thirty days after patient discharge, the World Health Organization Quality of Life-BREF questionnaire was administered by telephone.
A total of 216 patients were included. Delirium was identified in 127 (58.8%) of them. Patients with delirium exhibited greater functional dependence (median Barthel index 50.0 [21.2 - 70.0] versus 80.0 [60.0 - 95.0]; p < 0.001) and lower cognition (Mini Mental State Examination score 12.9 ± 7.5 versus 20.7 ± 9.8; p < 0.001) at hospital discharge. There was no difference in any of the quality-of-life domains evaluated 1 month after hospital discharge between patients with and without delirium.
Our findings suggest that patients with delirium in the intensive care unit do not have worse quality of life 1 month after hospital discharge, despite presenting greater cognitive impairment and functional disability at the time of hospital discharge.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):426-432
DOI 10.5935/0103-507X.20200072
To evaluate the association between the incidence of delirium in the intensive care unit and quality of life 1 month after hospital discharge.
This was a prospective cohort study conducted in the intensive care units of two medium-complexity hospitals from December 2015 to December 2016. Delirium was identified using the Confusion Assessment Method for the Intensive Care Unit scale. At the time of hospital discharge, functional capacity and cognition were assessed with the Barthel index and the Mini Mental State Examination, respectively. Thirty days after patient discharge, the World Health Organization Quality of Life-BREF questionnaire was administered by telephone.
A total of 216 patients were included. Delirium was identified in 127 (58.8%) of them. Patients with delirium exhibited greater functional dependence (median Barthel index 50.0 [21.2 - 70.0] versus 80.0 [60.0 - 95.0]; p < 0.001) and lower cognition (Mini Mental State Examination score 12.9 ± 7.5 versus 20.7 ± 9.8; p < 0.001) at hospital discharge. There was no difference in any of the quality-of-life domains evaluated 1 month after hospital discharge between patients with and without delirium.
Our findings suggest that patients with delirium in the intensive care unit do not have worse quality of life 1 month after hospital discharge, despite presenting greater cognitive impairment and functional disability at the time of hospital discharge.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.

Abstract
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
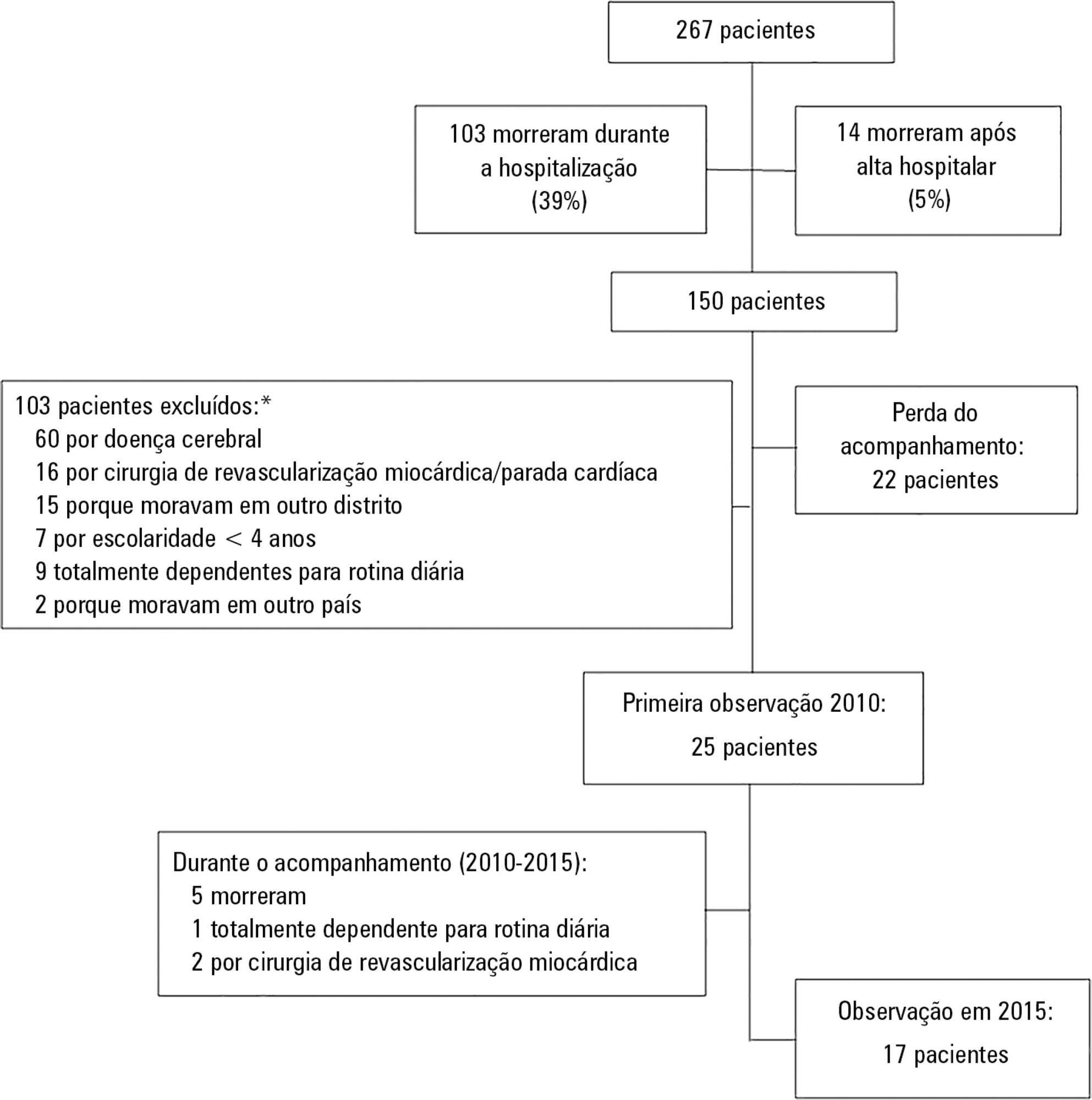
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):496-507
DOI 10.5935/0103-507X.20180071
To assess the long-term, health-related quality of life of intensive care unit survivors by systematic review.
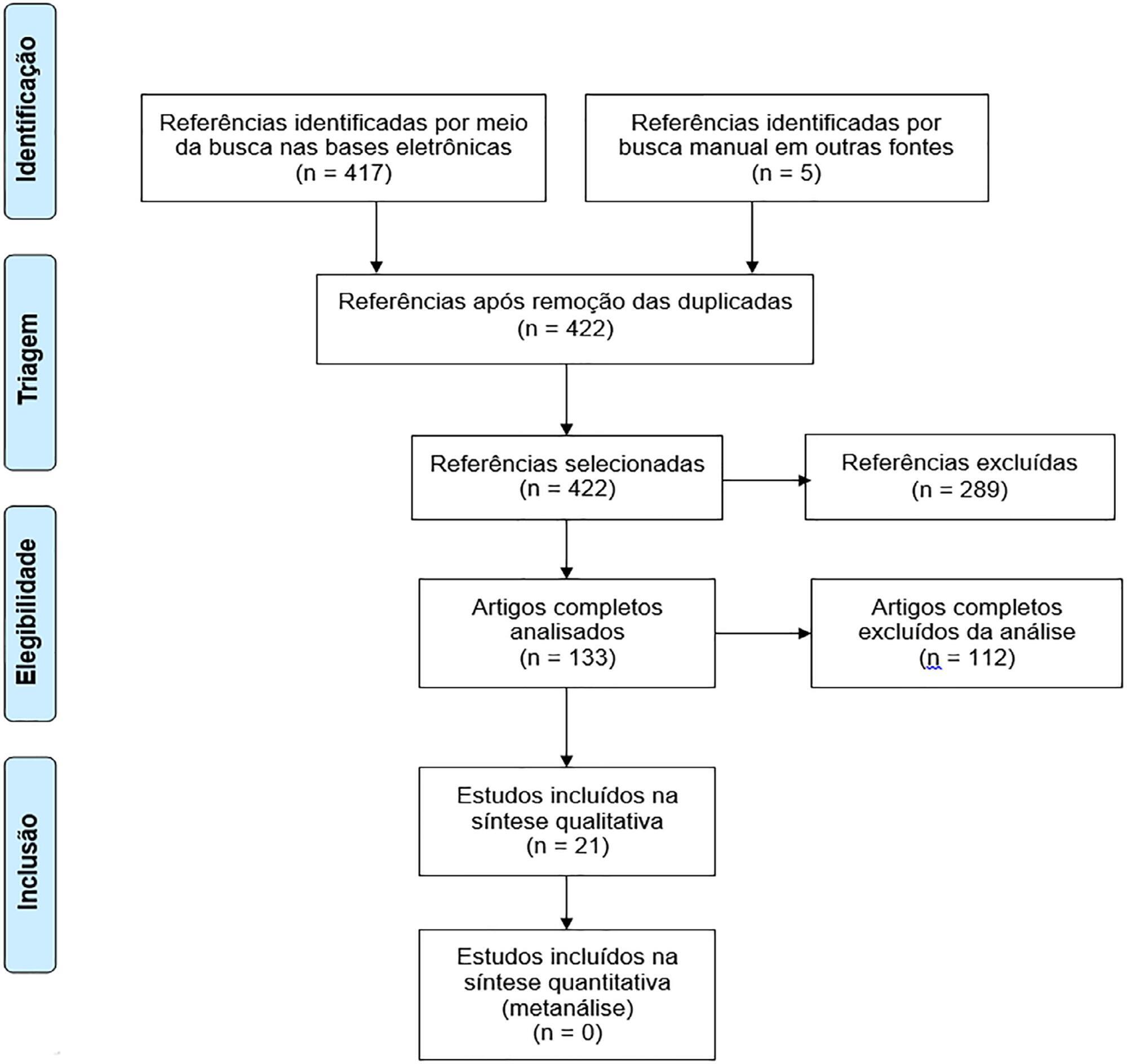
The search for, and selection and analysis of, observational studies that assessed the health-related quality of life of intensive care unit survivors in the electronic databases LILACS and MEDLINE® (accessed through PubMed) was performed using the indexed MESH terms "quality of life [MeSH Terms]" AND "critically illness [MeSH Terms]". Studies on adult patients without specific prior diseases published in English in the last 5 years were included in this systematic review. The citations were independently selected by three reviewers. Data were standardly and independently retrieved by two reviewers, and the quality of the studies was assessed using the Newcastle-Ottawa scale.
In total, 19 observational cohort and 2 case-control studies of 57,712 critically ill patients were included. The follow-up time of the studies ranged from 6 months to 6 years, and most studies had a 6-month or 1-year follow up. The health-related quality of life was assessed using two generic tools, the EuroQol and the Short Form Health Survey. The overall quality of the studies was low.
Long-term, health-related quality of life is compromised among intensive care unit survivors compared with the corresponding general population. However, it is not significantly affected by the occurrence of sepsis, delirium, and acute kidney injury during intensive care unit admission when compared with that of critically ill patient control groups. High-quality studies are necessary to quantify the health-related quality of life among intensive care unit survivors.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):496-507
DOI 10.5935/0103-507X.20180071
To assess the long-term, health-related quality of life of intensive care unit survivors by systematic review.
The search for, and selection and analysis of, observational studies that assessed the health-related quality of life of intensive care unit survivors in the electronic databases LILACS and MEDLINE® (accessed through PubMed) was performed using the indexed MESH terms "quality of life [MeSH Terms]" AND "critically illness [MeSH Terms]". Studies on adult patients without specific prior diseases published in English in the last 5 years were included in this systematic review. The citations were independently selected by three reviewers. Data were standardly and independently retrieved by two reviewers, and the quality of the studies was assessed using the Newcastle-Ottawa scale.
In total, 19 observational cohort and 2 case-control studies of 57,712 critically ill patients were included. The follow-up time of the studies ranged from 6 months to 6 years, and most studies had a 6-month or 1-year follow up. The health-related quality of life was assessed using two generic tools, the EuroQol and the Short Form Health Survey. The overall quality of the studies was low.
Long-term, health-related quality of life is compromised among intensive care unit survivors compared with the corresponding general population. However, it is not significantly affected by the occurrence of sepsis, delirium, and acute kidney injury during intensive care unit admission when compared with that of critically ill patient control groups. High-quality studies are necessary to quantify the health-related quality of life among intensive care unit survivors.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):47-54
DOI 10.5935/0103-507X.20170008
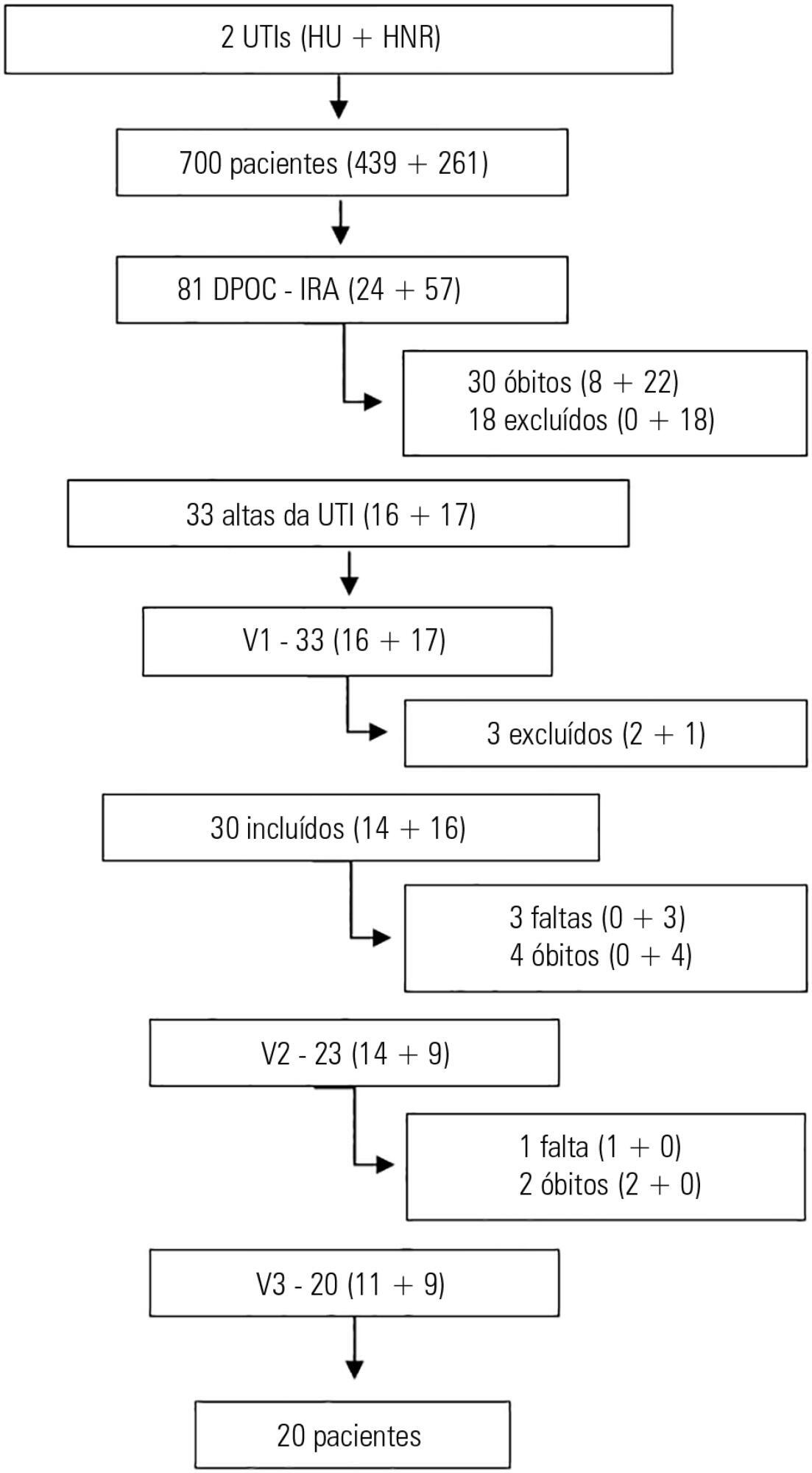
The purpose of this study was to evaluate the clinical/functional aspects and quality of life of chronic obstructive pulmonary disease patients who were discharged after an intensive care unit admission for acute respiratory failure.
This prospective study included chronic obstructive pulmonary disease patients who were admitted to two intensive care units between December of 2010 and August of 2011 and evaluated over three visits after discharge. Thirty patients were included, and 20 patients completed the three-month follow up.
There was a significant improvement in the following: forced expiratory flow in one second (L) (1.1/1.4/1.4; p = 0.019), six-minute walk test (m) (- /232.8 /272.6; p = 0.04), BODE score (7.5/5.0/3.8; p = 0.001), cognition measured by the Mini Mental State Examination (21/23.5/23.5; p = 0.008) and quality of life measured by the total Saint George Respiratory Questionnaire score (63.3/56.8/51, p = 0.02). The mean difference in the total score was 12.3 (between visits 1 and three). Important clinical differences were observed for the symptom score (18.8), activities score (5.2) and impact score (14.3). The majority of participants (80%) reported they would be willing to undergo a new intensive care unit admission.
Despite the disease severity, there was a significant clinical, functional and quality of life improvement at the end of the third month. Most patients would be willing to undergo a new intensive care unit admission.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):47-54
DOI 10.5935/0103-507X.20170008
The purpose of this study was to evaluate the clinical/functional aspects and quality of life of chronic obstructive pulmonary disease patients who were discharged after an intensive care unit admission for acute respiratory failure.
This prospective study included chronic obstructive pulmonary disease patients who were admitted to two intensive care units between December of 2010 and August of 2011 and evaluated over three visits after discharge. Thirty patients were included, and 20 patients completed the three-month follow up.
There was a significant improvement in the following: forced expiratory flow in one second (L) (1.1/1.4/1.4; p = 0.019), six-minute walk test (m) (- /232.8 /272.6; p = 0.04), BODE score (7.5/5.0/3.8; p = 0.001), cognition measured by the Mini Mental State Examination (21/23.5/23.5; p = 0.008) and quality of life measured by the total Saint George Respiratory Questionnaire score (63.3/56.8/51, p = 0.02). The mean difference in the total score was 12.3 (between visits 1 and three). Important clinical differences were observed for the symptom score (18.8), activities score (5.2) and impact score (14.3). The majority of participants (80%) reported they would be willing to undergo a new intensive care unit admission.
Despite the disease severity, there was a significant clinical, functional and quality of life improvement at the end of the third month. Most patients would be willing to undergo a new intensive care unit admission.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)