Physical functional performance Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 - 1.78] and 1.34 [1.0 - 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 - 154.43] and 47.79 [11.41 - 200.25], respectively); with a p < 0.05 for all results.
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 - 1.78] and 1.34 [1.0 - 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 - 154.43] and 47.79 [11.41 - 200.25], respectively); with a p < 0.05 for all results.
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):565-571
DOI 10.5935/0103-507X.20210073
To identify the factors associated with functional status decline in intensive care unit patients.
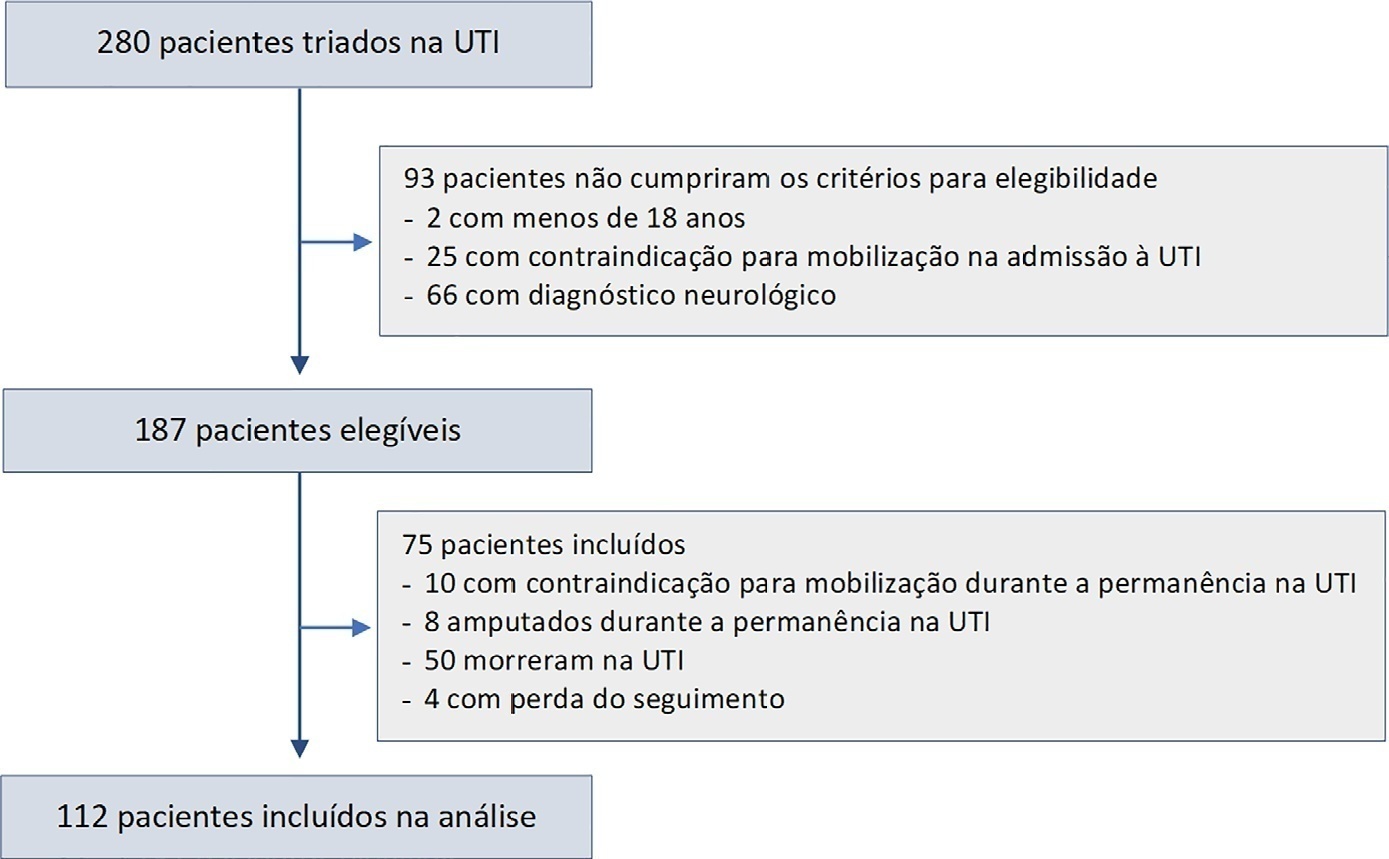
In this prospective study, patients in an intensive care unit aged 18 years or older without neurological disease or contraindications to mobilization were included. The exclusion criteria were patients who spent fewer than 4 days in the intensive care unit or died during the study period. Accelerometry was used to assess the physical activity level of patients. We recorded age, SAPS 3, days on mechanical ventilation, drugs used, comorbidities, and functional status after intensive care unit discharge. After intensive care unit discharge, the patients were assigned to a dependent group or an independent group according to their Barthel index. Logistic regression and the odds ratio were used in the analyses.
Sixty-three out of 112 included patients were assigned to the dependent group. The median Charlson comorbidity index was 3 (2 - 4). The mean SAPS 3 score was 53 ± 11. The patients spent 94 ± 4% of the time spent in inactivity and 4.8 ± 3.7% in light activities. The odds ratio showed that age (OR = 1.08; 95%CI 1.04 - 1.13) and time spent in inactivity (OR = 1.38; 95%CI 1.14 - 1.67) were factors associated with functional status decline. Time spent in light activity was associated with a better functional status (OR = 0.73; 95%CI 0.60 - 0.89).
Age and time spent in inactivity during intensive care unit stay are associated with functional status decline. On the other hand, performing light activities seems to preserve the functional status of patients.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):565-571
DOI 10.5935/0103-507X.20210073
To identify the factors associated with functional status decline in intensive care unit patients.
In this prospective study, patients in an intensive care unit aged 18 years or older without neurological disease or contraindications to mobilization were included. The exclusion criteria were patients who spent fewer than 4 days in the intensive care unit or died during the study period. Accelerometry was used to assess the physical activity level of patients. We recorded age, SAPS 3, days on mechanical ventilation, drugs used, comorbidities, and functional status after intensive care unit discharge. After intensive care unit discharge, the patients were assigned to a dependent group or an independent group according to their Barthel index. Logistic regression and the odds ratio were used in the analyses.
Sixty-three out of 112 included patients were assigned to the dependent group. The median Charlson comorbidity index was 3 (2 - 4). The mean SAPS 3 score was 53 ± 11. The patients spent 94 ± 4% of the time spent in inactivity and 4.8 ± 3.7% in light activities. The odds ratio showed that age (OR = 1.08; 95%CI 1.04 - 1.13) and time spent in inactivity (OR = 1.38; 95%CI 1.14 - 1.67) were factors associated with functional status decline. Time spent in light activity was associated with a better functional status (OR = 0.73; 95%CI 0.60 - 0.89).
Age and time spent in inactivity during intensive care unit stay are associated with functional status decline. On the other hand, performing light activities seems to preserve the functional status of patients.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
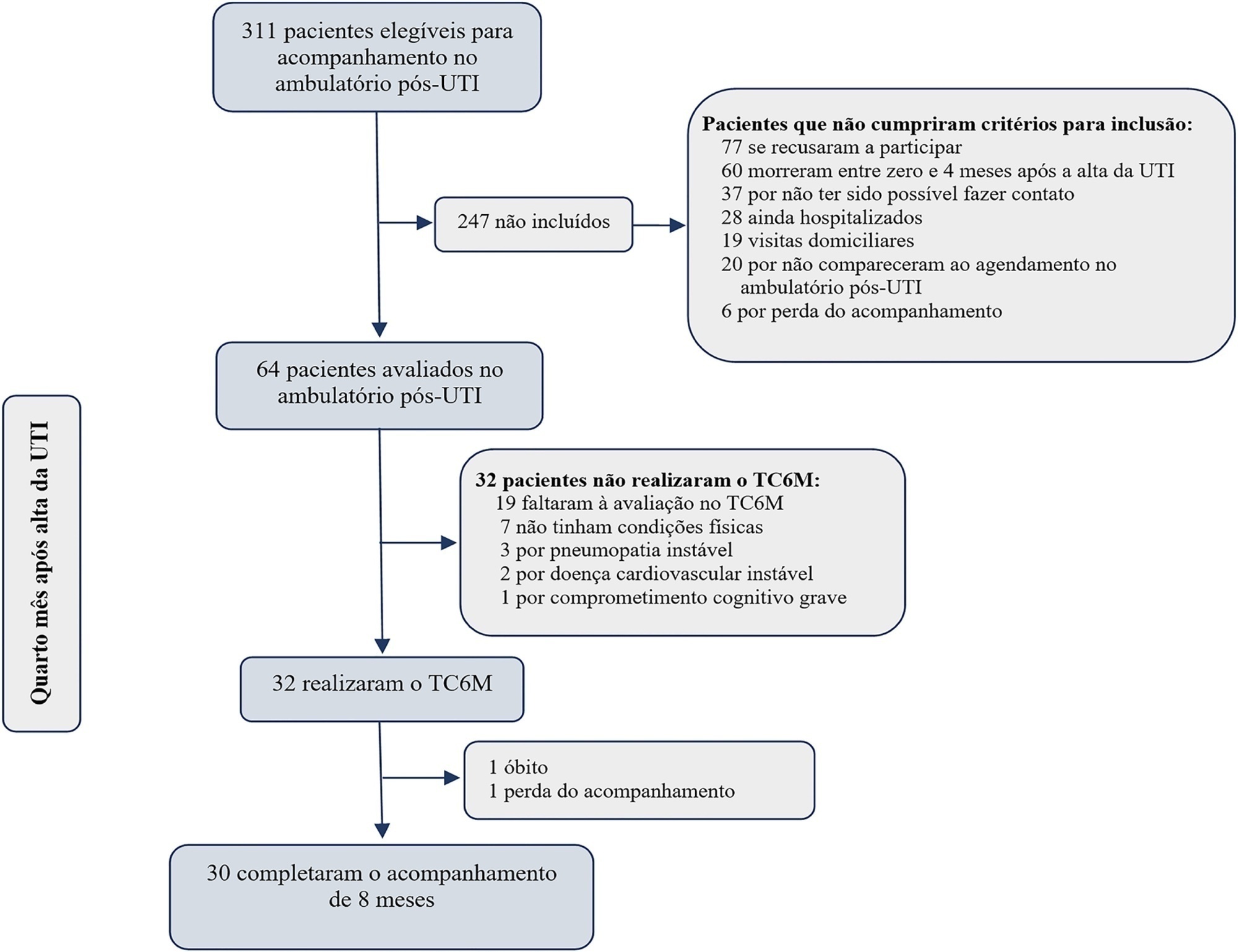
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):426-432
DOI 10.5935/0103-507X.20200072
To evaluate the association between the incidence of delirium in the intensive care unit and quality of life 1 month after hospital discharge.
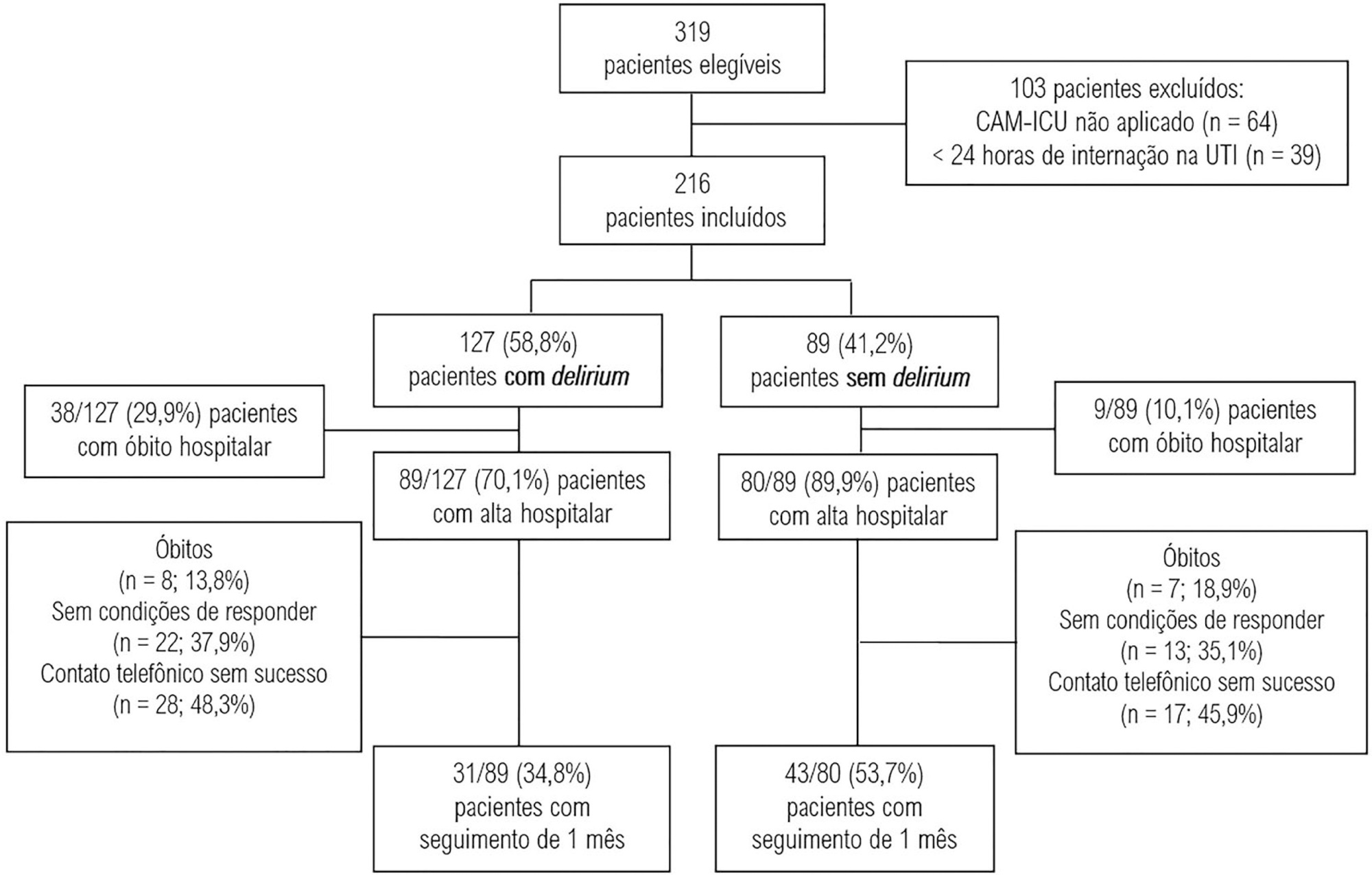
This was a prospective cohort study conducted in the intensive care units of two medium-complexity hospitals from December 2015 to December 2016. Delirium was identified using the Confusion Assessment Method for the Intensive Care Unit scale. At the time of hospital discharge, functional capacity and cognition were assessed with the Barthel index and the Mini Mental State Examination, respectively. Thirty days after patient discharge, the World Health Organization Quality of Life-BREF questionnaire was administered by telephone.
A total of 216 patients were included. Delirium was identified in 127 (58.8%) of them. Patients with delirium exhibited greater functional dependence (median Barthel index 50.0 [21.2 - 70.0] versus 80.0 [60.0 - 95.0]; p < 0.001) and lower cognition (Mini Mental State Examination score 12.9 ± 7.5 versus 20.7 ± 9.8; p < 0.001) at hospital discharge. There was no difference in any of the quality-of-life domains evaluated 1 month after hospital discharge between patients with and without delirium.
Our findings suggest that patients with delirium in the intensive care unit do not have worse quality of life 1 month after hospital discharge, despite presenting greater cognitive impairment and functional disability at the time of hospital discharge.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):426-432
DOI 10.5935/0103-507X.20200072
To evaluate the association between the incidence of delirium in the intensive care unit and quality of life 1 month after hospital discharge.
This was a prospective cohort study conducted in the intensive care units of two medium-complexity hospitals from December 2015 to December 2016. Delirium was identified using the Confusion Assessment Method for the Intensive Care Unit scale. At the time of hospital discharge, functional capacity and cognition were assessed with the Barthel index and the Mini Mental State Examination, respectively. Thirty days after patient discharge, the World Health Organization Quality of Life-BREF questionnaire was administered by telephone.
A total of 216 patients were included. Delirium was identified in 127 (58.8%) of them. Patients with delirium exhibited greater functional dependence (median Barthel index 50.0 [21.2 - 70.0] versus 80.0 [60.0 - 95.0]; p < 0.001) and lower cognition (Mini Mental State Examination score 12.9 ± 7.5 versus 20.7 ± 9.8; p < 0.001) at hospital discharge. There was no difference in any of the quality-of-life domains evaluated 1 month after hospital discharge between patients with and without delirium.
Our findings suggest that patients with delirium in the intensive care unit do not have worse quality of life 1 month after hospital discharge, despite presenting greater cognitive impairment and functional disability at the time of hospital discharge.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)