
You searched for:"Regis Goulart Rosa"
We found (25) results for your search.-
Original Article
Impact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
- Douglas Neves
 ,
, - Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari , [ … ],
- Pedro Dal Lago
Abstract
Original ArticleImpact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
- Douglas Neves ,
- Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari ,
- Laura Cordeiro Madeira ,
- Mariana Fensterseifer Mattioni ,
- Márcio Luiz Ferreira de Camillis ,
- Clarissa Garcia Soares Leães ,
- Juliana Mara Stormovski de Andrade ,
- Caroline Cabral Robinson ,
- Daniel Sganzerla ,
- Laura Drehmer ,
- Denis Fernandes Madruga da Costa ,
- André Sant’Ana Machado ,
- Regis Goulart Rosa ,
- Pedro Dal Lago
Views12ABSTRACT
Objective:
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
Methods:
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
Results:
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
Conclusion:
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Keywords:AerationIntensive care unitslungRespiration, artificialSitting positionStanding positionUltrasonographySee moreViews12

Abstract
Original ArticleImpact of vertical positioning on lung aeration among mechanically ventilated intensive care unit patients: a randomized crossover clinical trial
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
- Douglas Neves ,
- Paulo Ricardo Marques Filho ,
- Raquel da Silva Townsend ,
- Cristiano dos Santos Rodrigues ,
- Luciana Tagliari ,
- Laura Cordeiro Madeira ,
- Mariana Fensterseifer Mattioni ,
- Márcio Luiz Ferreira de Camillis ,
- Clarissa Garcia Soares Leães ,
- Juliana Mara Stormovski de Andrade ,
- Caroline Cabral Robinson ,
- Daniel Sganzerla ,
- Laura Drehmer ,
- Denis Fernandes Madruga da Costa ,
- André Sant’Ana Machado ,
- Regis Goulart Rosa ,
- Pedro Dal Lago
Views12ABSTRACT
Objective:
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
Methods:
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
Results:
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
Conclusion:
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Keywords:AerationIntensive care unitslungRespiration, artificialSitting positionStanding positionUltrasonographySee more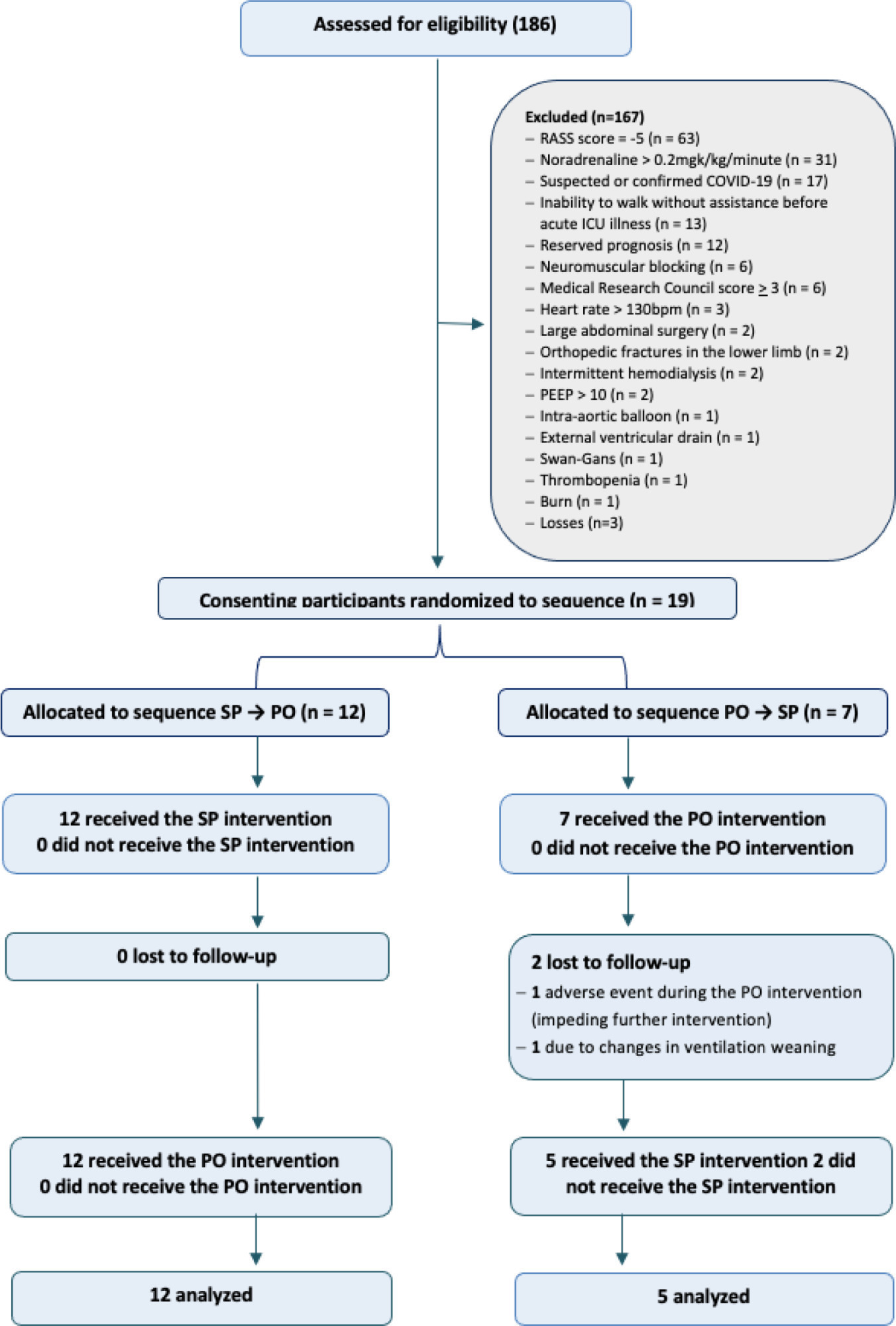
- Douglas Neves
-
Special Article
The II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
- Maicon Falavigna ,
- Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
Special ArticleThe II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
Crit Care Sci. 2023;35(3):243-255
DOI 10.5935/2965-2774.20230136-pt
- Maicon Falavigna ,
- Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Felipe Dal-Pizzol ,
- Rosemeri Maurici da Silva ,
- Luciano César Pontes de Azevedo ,
- Maria Beatriz Souza Dias,
- José Luiz Gomes do Amaral ,
- Gilson Pires Dorneles ,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- Flávia Ribeiro Machado ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Suena Medeiros Parahiba ,
- Regis Goulart Rosa ,
- Vania Cristina Canuto Santos ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Cinara Stein ,
- Carlos Roberto Ribeiro de Carvalho
Views22ABSTRACT
Objective:
To update the recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
Experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Twenty-one recommendations were generated, including strong recommendations for the use of corticosteroids in patients using supplemental oxygen and conditional recommendations for the use of tocilizumab and baricitinib for patients on supplemental oxygen or on noninvasive ventilation and anticoagulants to prevent thromboembolism. Due to suspension of use authorization, it was not possible to make recommendations regarding the use of casirivimab + imdevimab. Strong recommendations against the use of azithromycin in patients without suspected bacterial infection, hydroxychloroquine, convalescent plasma, colchicine, and lopinavir + ritonavir and conditional recommendations against the use of ivermectin and remdesivir were made.
Conclusion:
New recommendations for the treatment of hospitalized patients with COVID-19 were generated, such as those for tocilizumab and baricitinib. Corticosteroids and prophylaxis for thromboembolism are still recommended, the latter with conditional recommendation. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and to promote resource economy.
Keywords:BrazilCoronavirus infectionsCOVID-19COVID-19/drug therapyHealth planning guidelinesSARS-CoV-2See moreViews22Abstract
Special ArticleThe II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
Crit Care Sci. 2023;35(3):243-255
DOI 10.5935/2965-2774.20230136-pt
- Maicon Falavigna ,
- Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Felipe Dal-Pizzol ,
- Rosemeri Maurici da Silva ,
- Luciano César Pontes de Azevedo ,
- Maria Beatriz Souza Dias,
- José Luiz Gomes do Amaral ,
- Gilson Pires Dorneles ,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- Flávia Ribeiro Machado ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Suena Medeiros Parahiba ,
- Regis Goulart Rosa ,
- Vania Cristina Canuto Santos ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Cinara Stein ,
- Carlos Roberto Ribeiro de Carvalho
Views22ABSTRACT
Objective:
To update the recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
Experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Twenty-one recommendations were generated, including strong recommendations for the use of corticosteroids in patients using supplemental oxygen and conditional recommendations for the use of tocilizumab and baricitinib for patients on supplemental oxygen or on noninvasive ventilation and anticoagulants to prevent thromboembolism. Due to suspension of use authorization, it was not possible to make recommendations regarding the use of casirivimab + imdevimab. Strong recommendations against the use of azithromycin in patients without suspected bacterial infection, hydroxychloroquine, convalescent plasma, colchicine, and lopinavir + ritonavir and conditional recommendations against the use of ivermectin and remdesivir were made.
Conclusion:
New recommendations for the treatment of hospitalized patients with COVID-19 were generated, such as those for tocilizumab and baricitinib. Corticosteroids and prophylaxis for thromboembolism are still recommended, the latter with conditional recommendation. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and to promote resource economy.
Keywords:BrazilCoronavirus infectionsCOVID-19COVID-19/drug therapyHealth planning guidelinesSARS-CoV-2See more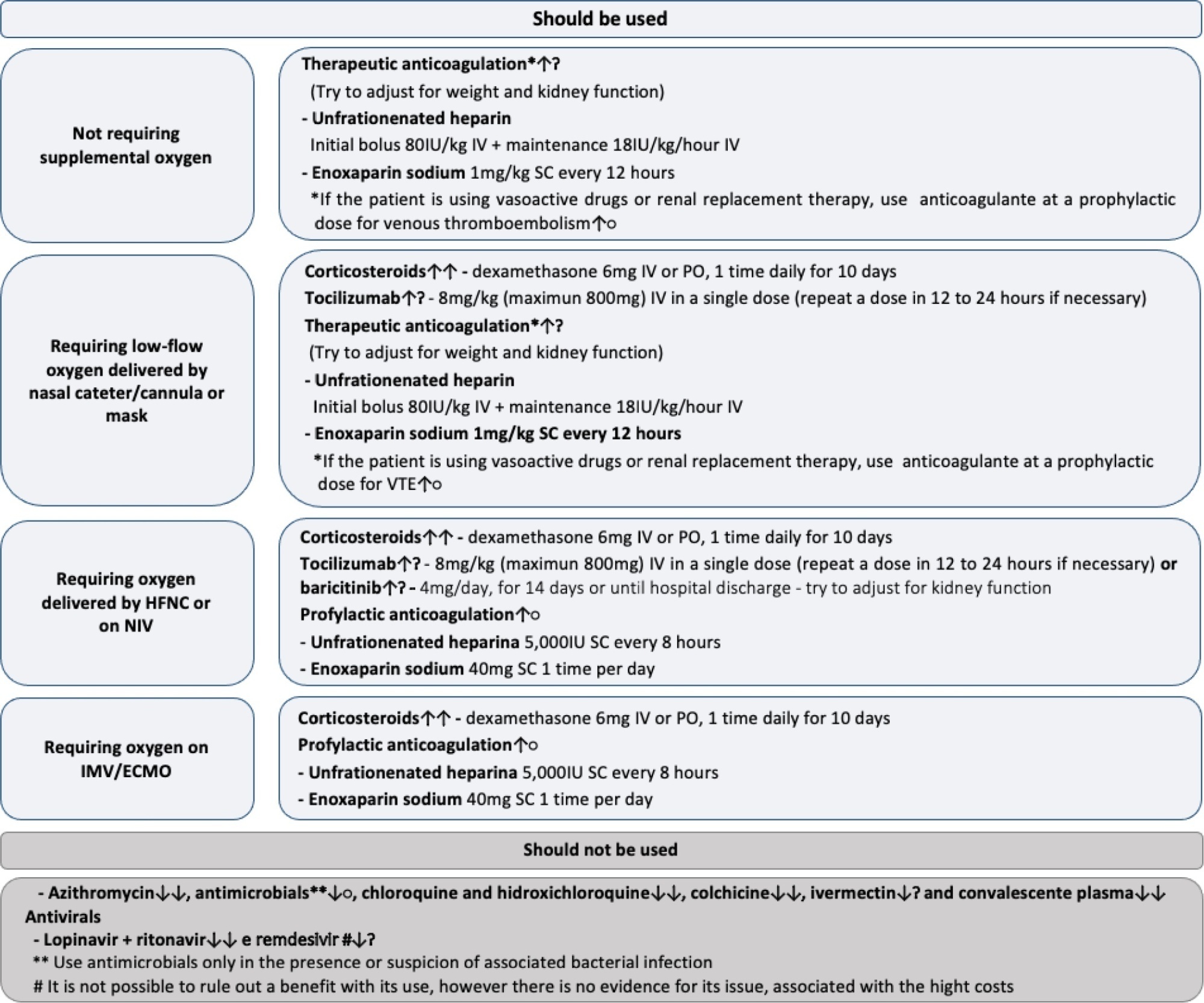
- Maicon Falavigna
-
Original Article
Effects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech , [ … ],
- Mellina da Silva Terres
Abstract
Original ArticleEffects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
Crit Care Sci. 2023;35(2):203-208
DOI 10.5935/2965-2774.20230274-pt
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech ,
- Daiana Barbosa da Silva ,
- Mellina da Silva Terres
Views4See moreABSTRACT
Objective:
To investigate whether family participation in intensive care unit interdisciplinary bedside rounds affects family satisfaction.
Methods:
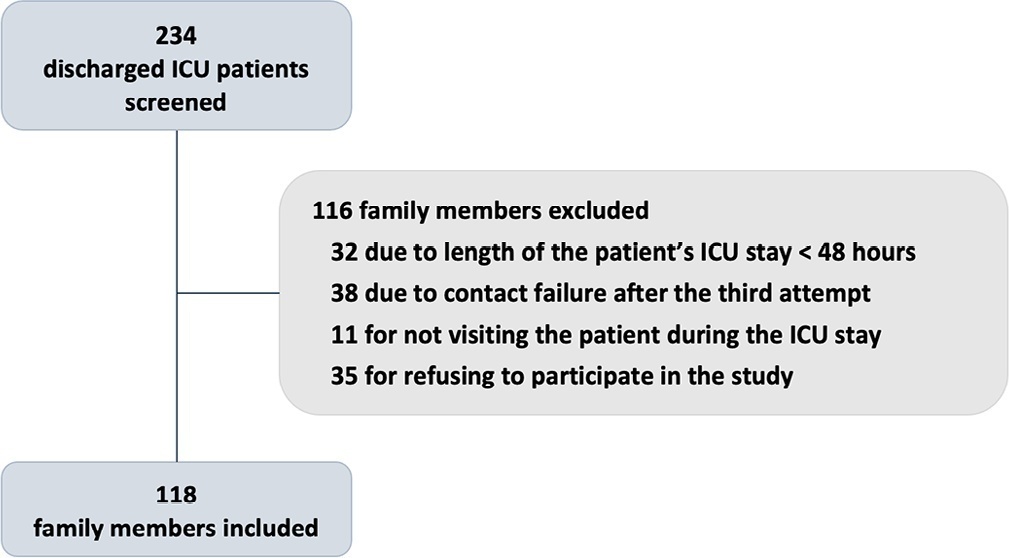
A cross-sectional study was conducted at a 56-bed, adult, mixed intensive care unit of a tertiary hospital in Southern Brazil. From May to June 2019, family members of patients who stayed in the intensive care unit for at least 48 hours were invited to participate in the study at the time of patient discharge. The main exposure variable was participation in intensive care unit bedside rounds during the intensive care unit stay. Family satisfaction was assessed by using the Brazilian version of the Family Satisfaction in the Intensive Care Unit questionnaire.
Results:
Of the 234 screened individuals, 118 were included. Eleven participants withdrew consent. A total of 107 individuals were assessed; 58 (54%) reported being present during bedside rounds, and 49 (46%) reported never being present. General satisfaction and satisfaction with the decision-making process were higher among families who were present during rounds than among families who were not (p = 0.01 and p = 0.007, respectively).
Conclusion:
The presence during interdisciplinary rounds was associated with improved general satisfaction and satisfaction with the decision-making aspect. This outcome indicates that efforts must be directed to conduct studies with more robust methodologies to confirm this association.
Views4Abstract
Original ArticleEffects of participation in interdisciplinary rounds in the intensive care unit on family satisfaction: A cross-sectional study
Crit Care Sci. 2023;35(2):203-208
DOI 10.5935/2965-2774.20230274-pt
- Daniel Schneider ,
- Regis Goulart Rosa ,
- Rosa da Rosa Minho dos Santos ,
- Débora Vaccaro Fogazzi ,
- Gabriela Soares Rech ,
- Daiana Barbosa da Silva ,
- Mellina da Silva Terres
Views4See moreABSTRACT
Objective:
To investigate whether family participation in intensive care unit interdisciplinary bedside rounds affects family satisfaction.
Methods:
A cross-sectional study was conducted at a 56-bed, adult, mixed intensive care unit of a tertiary hospital in Southern Brazil. From May to June 2019, family members of patients who stayed in the intensive care unit for at least 48 hours were invited to participate in the study at the time of patient discharge. The main exposure variable was participation in intensive care unit bedside rounds during the intensive care unit stay. Family satisfaction was assessed by using the Brazilian version of the Family Satisfaction in the Intensive Care Unit questionnaire.
Results:
Of the 234 screened individuals, 118 were included. Eleven participants withdrew consent. A total of 107 individuals were assessed; 58 (54%) reported being present during bedside rounds, and 49 (46%) reported never being present. General satisfaction and satisfaction with the decision-making process were higher among families who were present during rounds than among families who were not (p = 0.01 and p = 0.007, respectively).
Conclusion:
The presence during interdisciplinary rounds was associated with improved general satisfaction and satisfaction with the decision-making aspect. This outcome indicates that efforts must be directed to conduct studies with more robust methodologies to confirm this association.
- Daniel Schneider
-
Original Article
Does an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson, [ … ],
- Cleidilene Ramos Magalhães
Abstract
Original ArticleDoes an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson,
- Cláudia Severgnini Eugênio ,
- Cleidilene Ramos Magalhães
Views9ABSTRACT
Objective:
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
Methods:
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
Results:
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 – 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Conclusion:
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Keywords:AnxietyDepressionFamilyHealth information systemsIntensive care unitsInternetOutcome assessment, health carePersonal satisfactionSee moreViews9Abstract
Original ArticleDoes an educational website improve psychological outcomes and satisfaction among family members of intensive care unit patients?
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
- Tarissa da Silva Ribeiro Haack ,
- Regis Goulart Rosa ,
- Cassiano Teixeira ,
- Daniel Sganzerla ,
- Caroline Cabral Robinson,
- Cláudia Severgnini Eugênio ,
- Cleidilene Ramos Magalhães
Views9ABSTRACT
Objective:
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
Methods:
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
Results:
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 – 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Conclusion:
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Keywords:AnxietyDepressionFamilyHealth information systemsIntensive care unitsInternetOutcome assessment, health carePersonal satisfactionSee more
- Tarissa da Silva Ribeiro Haack
-
Original Article
Return to work after discharge from the intensive care unit: a Brazilian multicenter cohort
Rev Bras Ter Intensiva. 2022;34(4):492-498
Abstract
Original ArticleReturn to work after discharge from the intensive care unit: a Brazilian multicenter cohort
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
Views4See moreABSTRACT
Objective:
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
Methods:
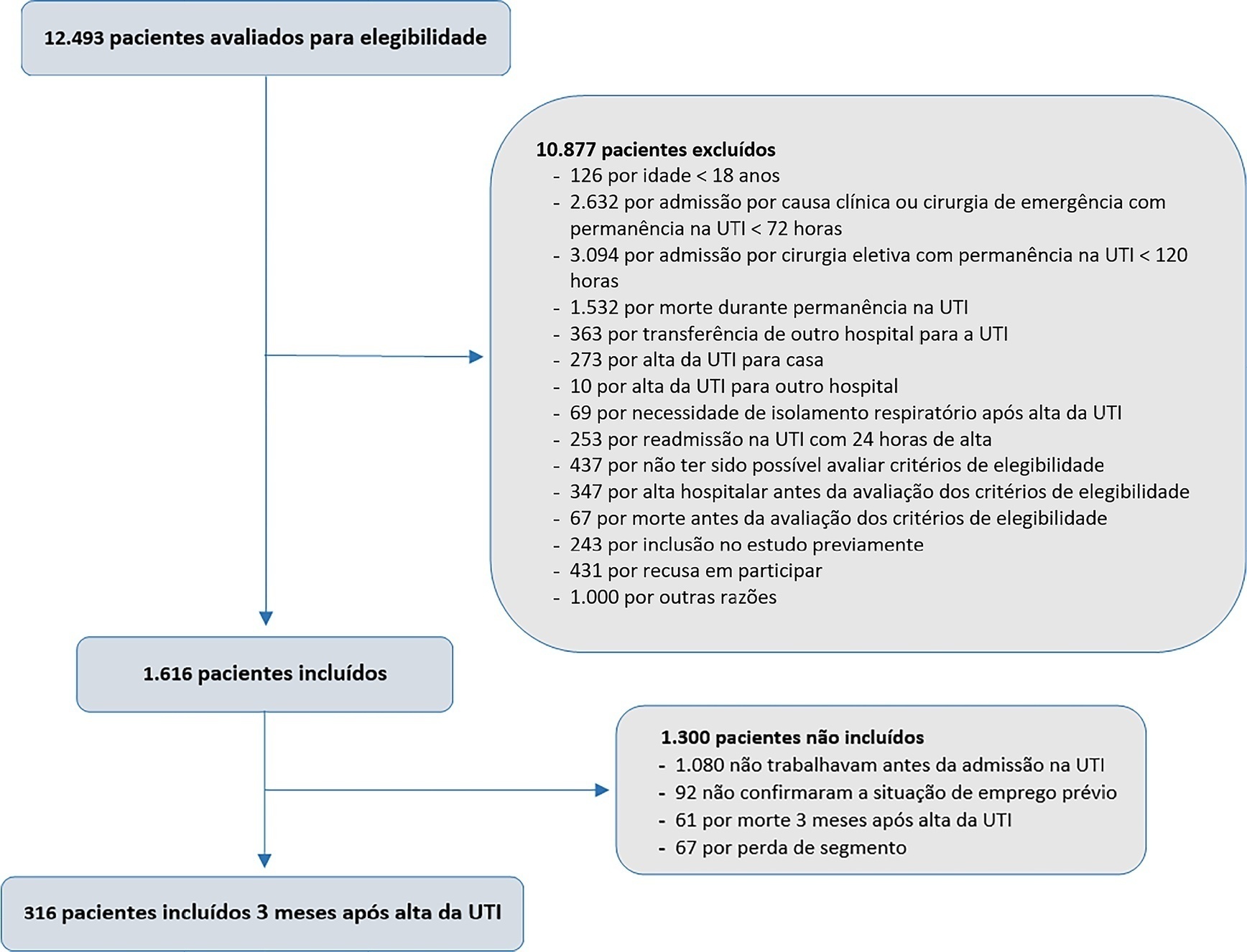
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Results:
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 – 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 – 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 – 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 – 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Conclusion:
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
Views4Abstract
Original ArticleReturn to work after discharge from the intensive care unit: a Brazilian multicenter cohort
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
Views4See moreABSTRACT
Objective:
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
Methods:
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Results:
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 – 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 – 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 – 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 – 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Conclusion:
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
-
Original Article
Clinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho , [ … ],
- Luciano César Pontes de Azevedo
Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee moreViews3Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee more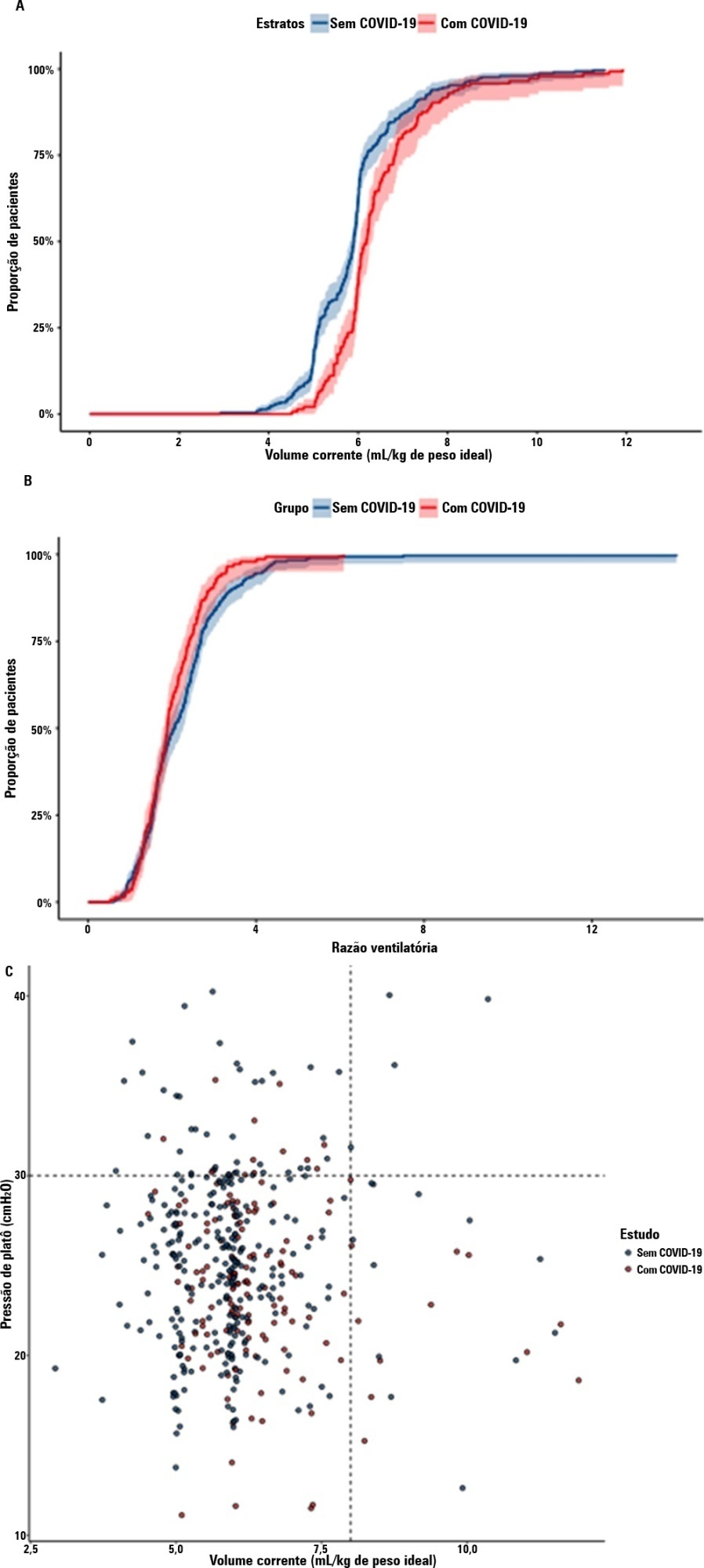
- Bruno Martins Tomazini
-
Original Article
Comparison between the perceptions of family members and health professionals regarding a flexible visitation model in an adult intensive care unit: a cross-sectional study
- Cláudia Severgnini Eugênio ,
- Tarissa da Silva Ribeiro Haack ,
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Emiliane Nogueira de Souza
Abstract
Original ArticleComparison between the perceptions of family members and health professionals regarding a flexible visitation model in an adult intensive care unit: a cross-sectional study
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
- Cláudia Severgnini Eugênio ,
- Tarissa da Silva Ribeiro Haack ,
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Emiliane Nogueira de Souza
Views3ABSTRACT
Objective:
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Methods:
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Results:
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Conclusion:
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Keywords:Critical careFamilyIntensive care units/organization & administrationPatient care teamPerceptionVisitors to patientsSee moreViews3Abstract
Original ArticleComparison between the perceptions of family members and health professionals regarding a flexible visitation model in an adult intensive care unit: a cross-sectional study
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
- Cláudia Severgnini Eugênio ,
- Tarissa da Silva Ribeiro Haack ,
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Emiliane Nogueira de Souza
Views3ABSTRACT
Objective:
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Methods:
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Results:
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Conclusion:
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Keywords:Critical careFamilyIntensive care units/organization & administrationPatient care teamPerceptionVisitors to patientsSee more - Cláudia Severgnini Eugênio
-
Special Article
Antivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Special ArticleAntivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos ,
- Karina Leal Negrelli ,
- Samara Pinheiro do Carmo Gomes ,
- Jaqueline Oliveira Gomes ,
- Mariana Barbosa dos Santos Carollo ,
- Tamiris Abait Miranda ,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira ,
- Glauco Adrieno Westphal ,
- Jacques Gabriel Alvares Horta ,
- Uri Adrian Prync Flato ,
- Camilo Fernandes ,
- Waldemar Carlos Barros ,
- Renata S Bolan ,
- Otávio Celso Eluf Gebara ,
- Meton Soares de Alencar Filho ,
- Victor Augusto Hamamoto ,
- Mauro Esteves Hernandes ,
- Nicole Alberti Golin ,
- Ronald Torres de Olinda ,
- Flávia Ribeiro Machado ,
- Régis Goulart Rosa ,
- Viviane Cordeiro Veiga ,
- Luciano César Pontes de Azevedo ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Tiago Moreno L Souza ,
- Otávio Berwanger ,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier:
Keywords:Antiviral agentsCoronavirus infectionsCOVID-19DaclatasvirprotocolRespiratory insufficiencySofosbuvirSee moreViews2Abstract
Special ArticleAntivirals for adult patients hospitalized with SARS-CoV-2 infection: A randomized, Phase II/III, multicenter, placebo-controlled, adaptive study, with multiple arms and stages. COALITION COVID-19 BRAZIL IX – REVOLUTIOn: protocol and statistical analysis plan
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
- Israel Silva Maia ,
- Aline Marcadenti ,
- Fernando Godinho Zampieri ,
- Lucas Petri Damiani ,
- Renato Hideo Nakagawa Santos ,
- Karina Leal Negrelli ,
- Samara Pinheiro do Carmo Gomes ,
- Jaqueline Oliveira Gomes ,
- Mariana Barbosa dos Santos Carollo ,
- Tamiris Abait Miranda ,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira ,
- Glauco Adrieno Westphal ,
- Jacques Gabriel Alvares Horta ,
- Uri Adrian Prync Flato ,
- Camilo Fernandes ,
- Waldemar Carlos Barros ,
- Renata S Bolan ,
- Otávio Celso Eluf Gebara ,
- Meton Soares de Alencar Filho ,
- Victor Augusto Hamamoto ,
- Mauro Esteves Hernandes ,
- Nicole Alberti Golin ,
- Ronald Torres de Olinda ,
- Flávia Ribeiro Machado ,
- Régis Goulart Rosa ,
- Viviane Cordeiro Veiga ,
- Luciano César Pontes de Azevedo ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Tiago Moreno L Souza ,
- Otávio Berwanger ,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier:
Keywords:Antiviral agentsCoronavirus infectionsCOVID-19DaclatasvirprotocolRespiratory insufficiencySofosbuvirSee more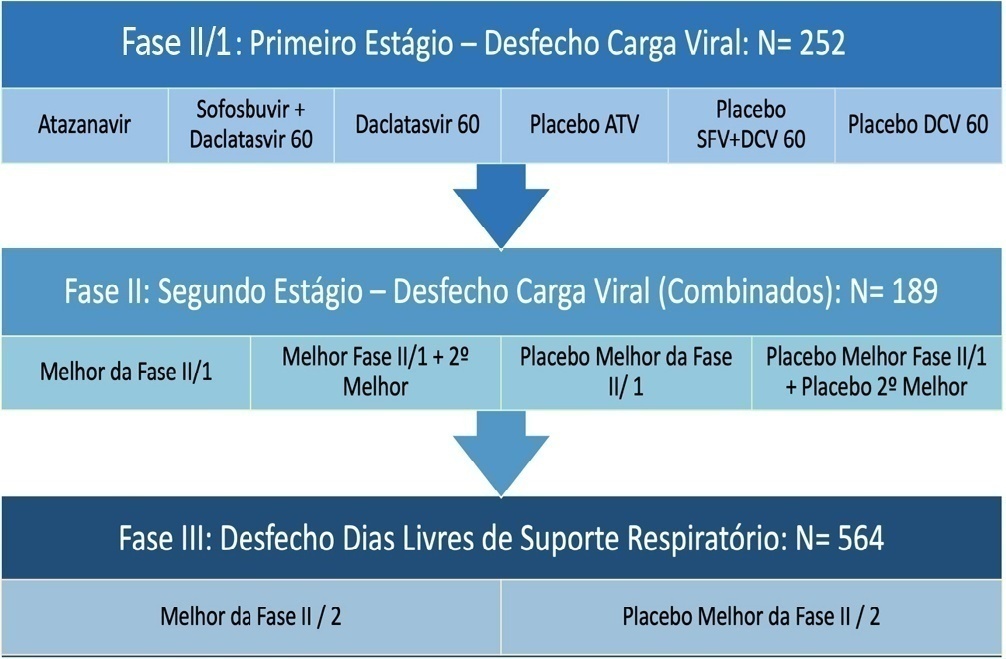
- Israel Silva Maia
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis