Patient care team Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
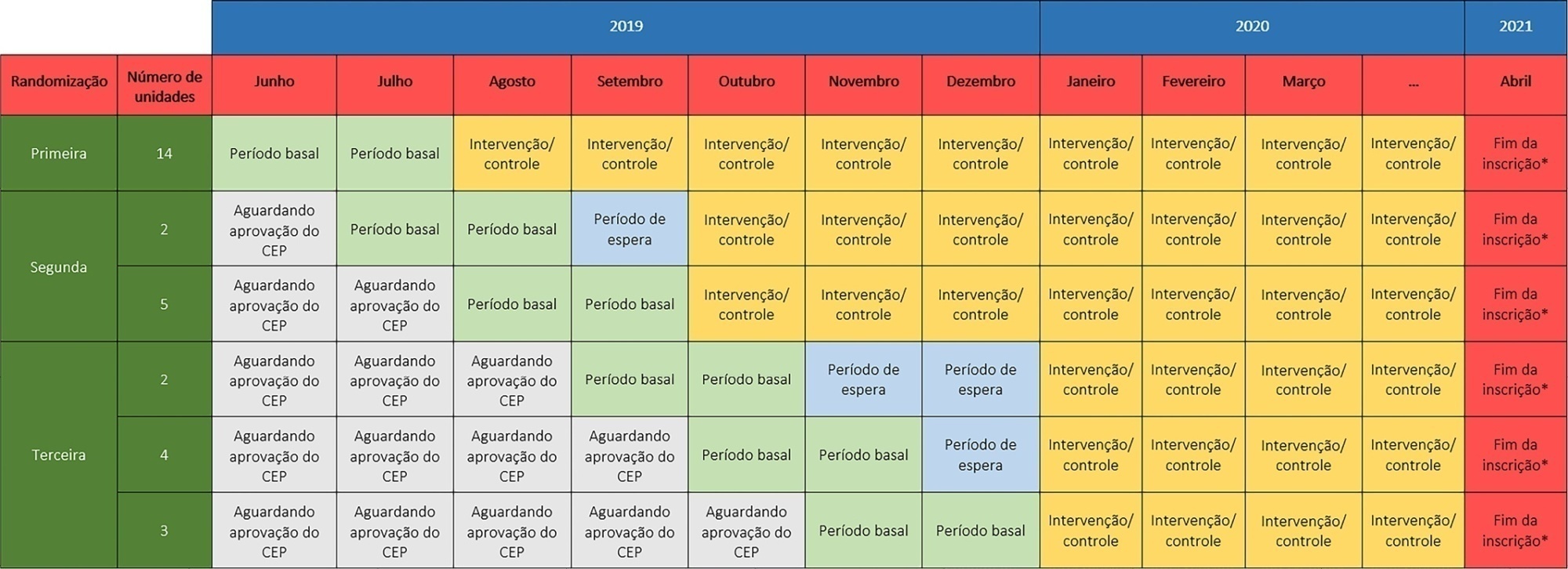
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
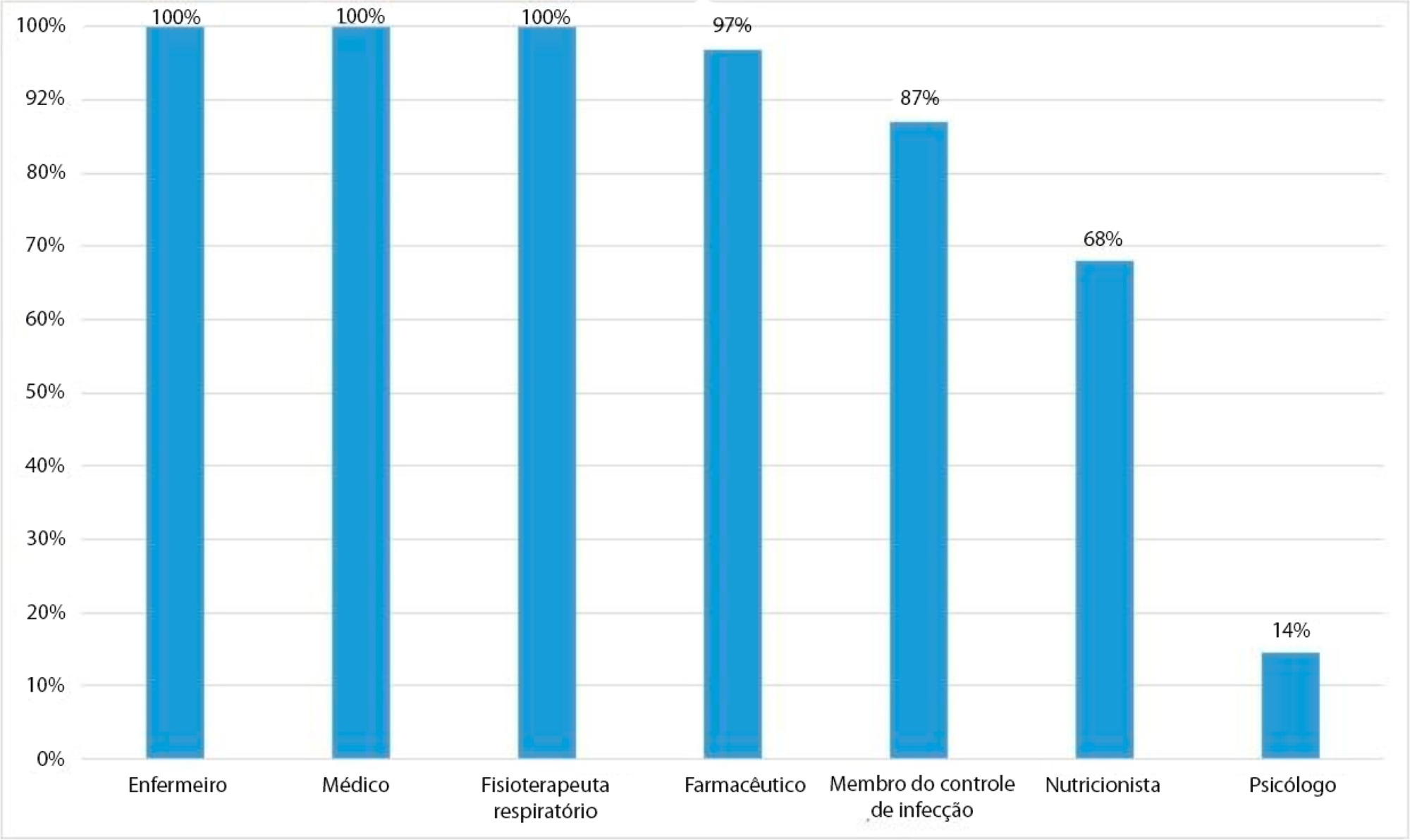
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 - 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 - 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
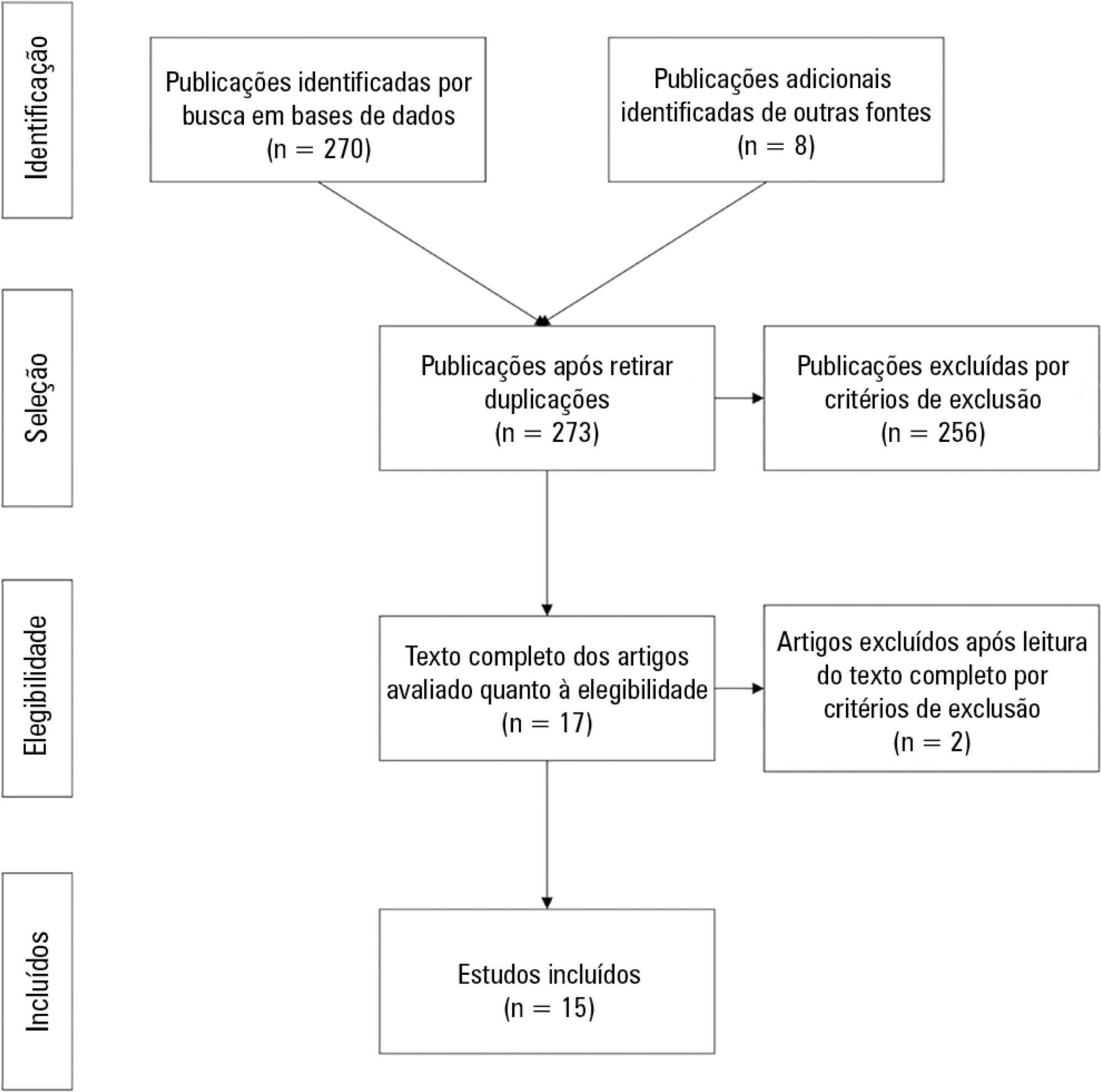
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 - 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 - 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 - 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 - 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher's exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
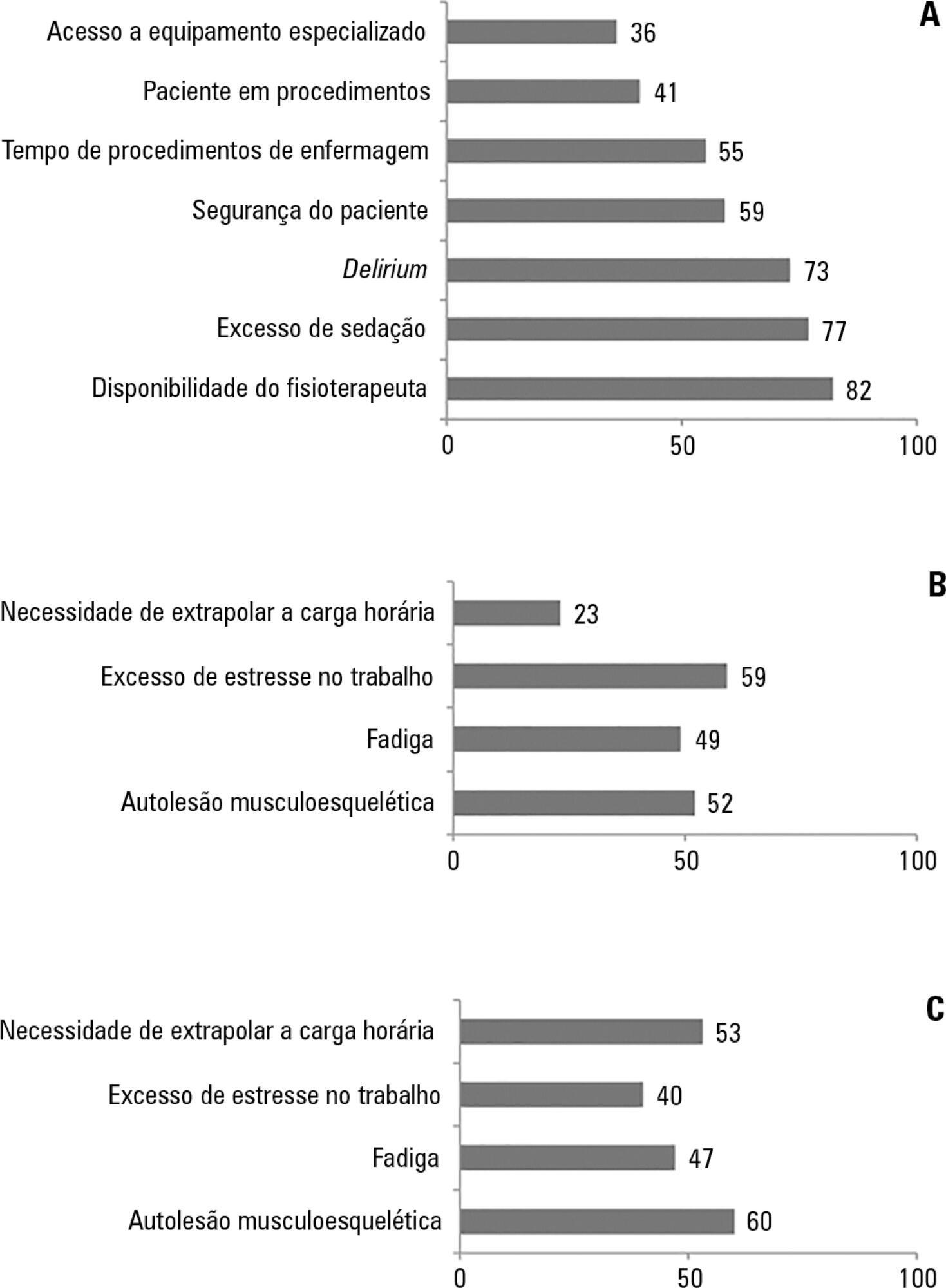
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher's exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):38-44
DOI 10.1590/S0103-507X2009000100006
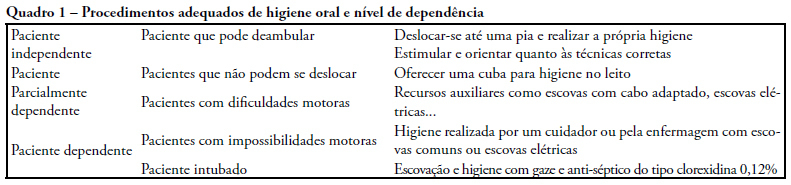
OBJECTIVES: A study was carried out, by means of a questionnaire for guided interviews seeking to establish a profile of perceptions and oral care given by ICU nursing team to patients in intensive care units. METHODS: The target population consisted of nursing practitioners divided in three education categories: nurses, nursing technicians and auxiliary nurses working at public and private hospital institutions providing for intensive care unit patients in Belem-PA. Dentistry experience has developed in this field reporting scientific findings and practical applications on prevention and reestablishment of the oral health in question. RESULTS: This survey disclosed results suggesting that oral hygiene care given to intensive care units patients is insufficient and inadequate requiring changes be made in the care now provided in the nosocomial environment by the nursing team. CONCLUSION: Presence of a dentist, knowledge of preventive dentistry, dissemination and use of oral hygiene specific resources are means suggested in an attempt to resolve difficulties found in oral health maintenance and treatment of oral diseases that affect the general health of hospitalized individuals. Interdisciplinary action for these individuals is advocated to achieve a better quality of life by preventing or minimizing oral pathologies.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):38-44
DOI 10.1590/S0103-507X2009000100006
OBJECTIVES: A study was carried out, by means of a questionnaire for guided interviews seeking to establish a profile of perceptions and oral care given by ICU nursing team to patients in intensive care units. METHODS: The target population consisted of nursing practitioners divided in three education categories: nurses, nursing technicians and auxiliary nurses working at public and private hospital institutions providing for intensive care unit patients in Belem-PA. Dentistry experience has developed in this field reporting scientific findings and practical applications on prevention and reestablishment of the oral health in question. RESULTS: This survey disclosed results suggesting that oral hygiene care given to intensive care units patients is insufficient and inadequate requiring changes be made in the care now provided in the nosocomial environment by the nursing team. CONCLUSION: Presence of a dentist, knowledge of preventive dentistry, dissemination and use of oral hygiene specific resources are means suggested in an attempt to resolve difficulties found in oral health maintenance and treatment of oral diseases that affect the general health of hospitalized individuals. Interdisciplinary action for these individuals is advocated to achieve a better quality of life by preventing or minimizing oral pathologies.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)