systematic review Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
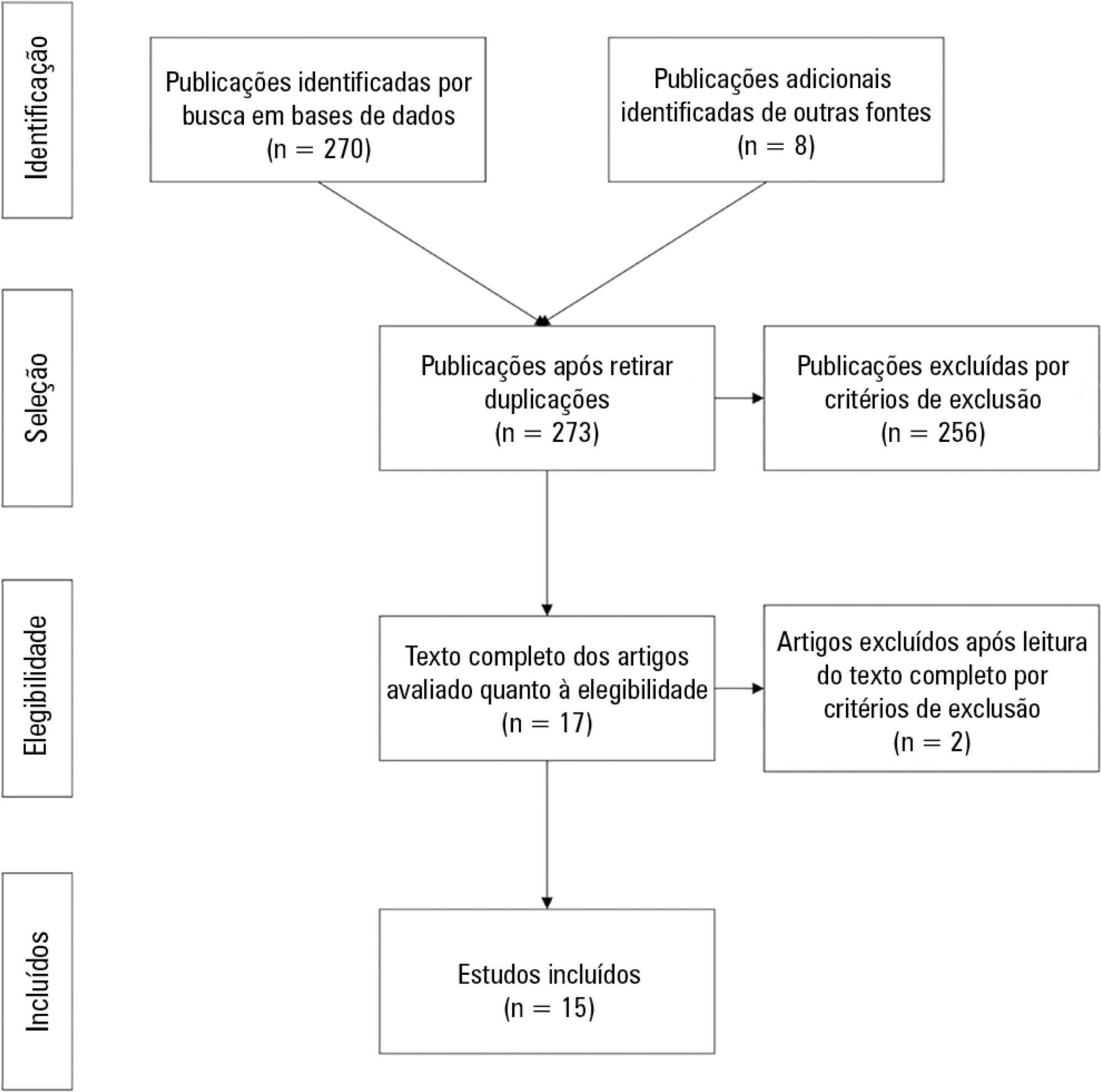
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 - 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 - 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 - 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 - 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
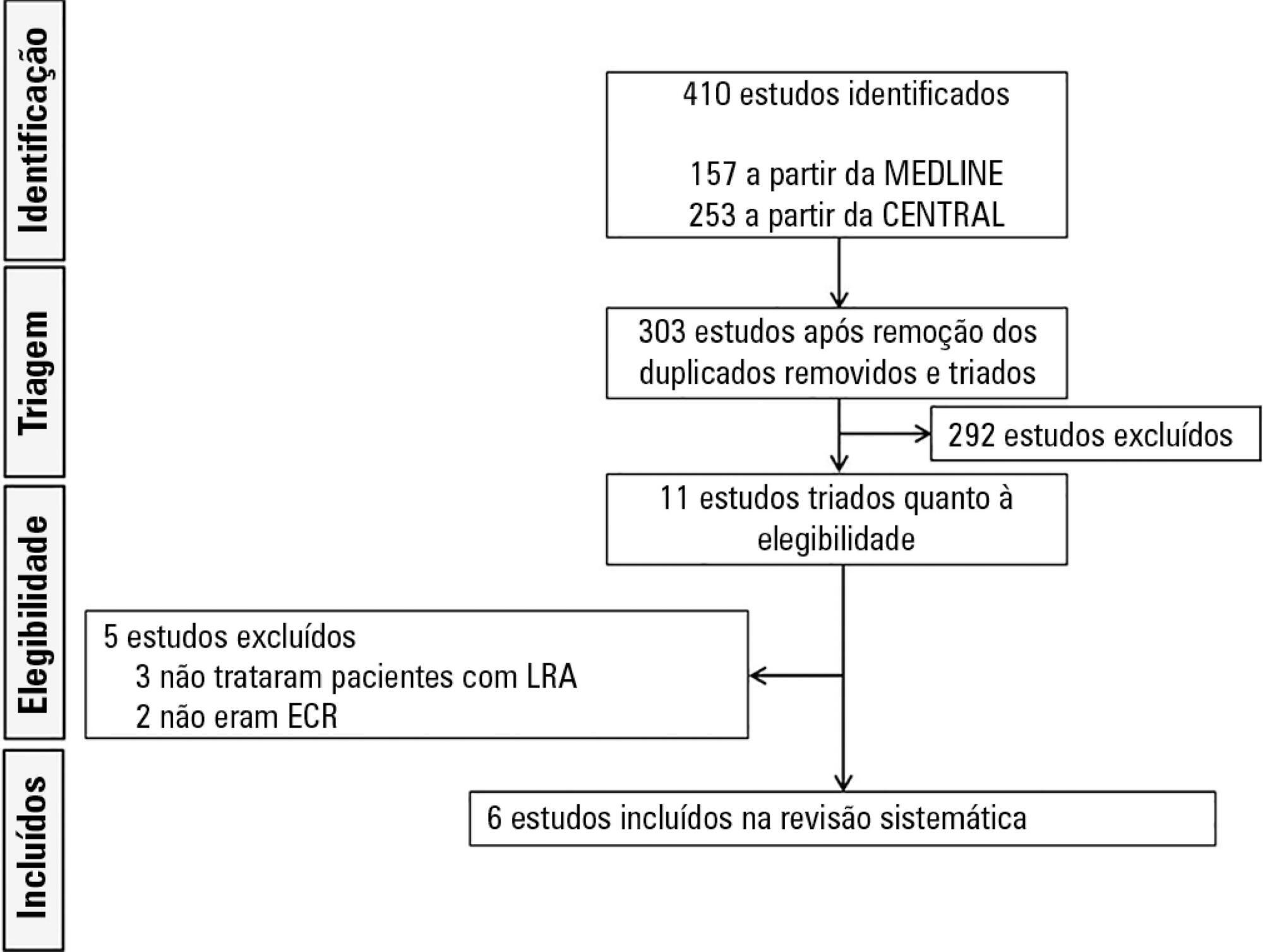
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 - 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 - 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 - 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 - 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
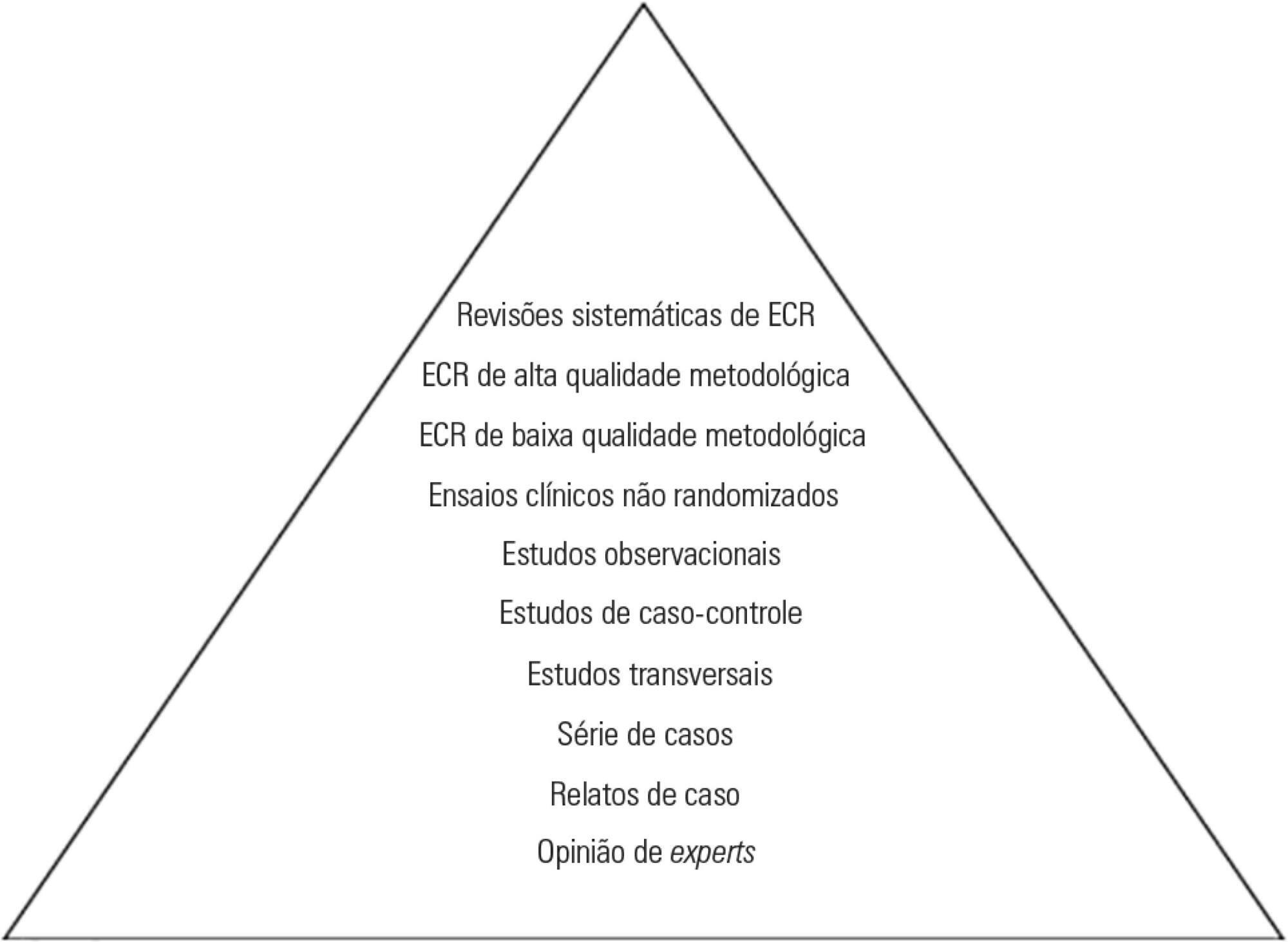
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):256-260
DOI 10.5935/0103-507X.20160050
Different research designs have various advantages and limitations inherent to their main characteristics. Knowledge of the proper use of each design is of great importance to understanding the applicability of research findings to clinical epidemiology.
In intensive care, a hierarchical classification of designs can often be misleading if the characteristics of the design in this context are not understood. One must therefore be alert to common problems in randomized clinical trials and systematic reviews/meta-analyses that address clinical issues related to the care of the critically ill patient.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):475-480
DOI 10.1590/S0103-507X2007000400012
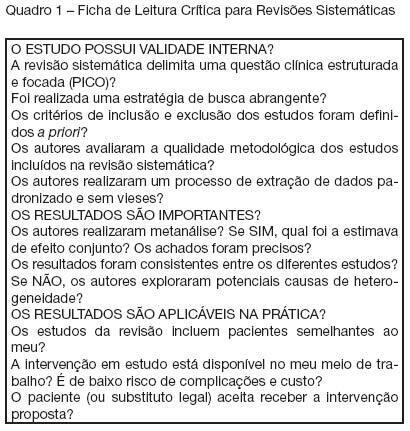
BACKGROUND AND OBJECTIVES: Systematic reviews are important knowledge generating tools to help the decision making process in the Critical Care Unit. This narrative aims to describe the important elements used to critically appraise intensive care-related systematic reviews. CONTENTS: When critically assessing systematic reviews, one should pay particular attention to the importance and appropriateness of the research question, the search strategy, the inclusion criteria and methodological quality of the studies included, and the methods of data extraction. In addition, a relevant systematic review must have consistent data (in case of a meta-analysis) or the cause of the heterogeneity must have been adequately explored, and results must be applicable in critical patients. CONCLUSIONS: To apply correctly the available scientific evidence, one should critically assess data quality of systematic reviews, selecting the relevant information to manage the critically ill patient.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):475-480
DOI 10.1590/S0103-507X2007000400012
BACKGROUND AND OBJECTIVES: Systematic reviews are important knowledge generating tools to help the decision making process in the Critical Care Unit. This narrative aims to describe the important elements used to critically appraise intensive care-related systematic reviews. CONTENTS: When critically assessing systematic reviews, one should pay particular attention to the importance and appropriateness of the research question, the search strategy, the inclusion criteria and methodological quality of the studies included, and the methods of data extraction. In addition, a relevant systematic review must have consistent data (in case of a meta-analysis) or the cause of the heterogeneity must have been adequately explored, and results must be applicable in critical patients. CONCLUSIONS: To apply correctly the available scientific evidence, one should critically assess data quality of systematic reviews, selecting the relevant information to manage the critically ill patient.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)