
You searched for:"Ary Serpa Neto"
We found (11) results for your search.-
Special Article
Statistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
- Otavio Ranzani
 ,
, - Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz , [ … ],
- Danilo Teixeira Noritomi
Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee moreViews2

Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee more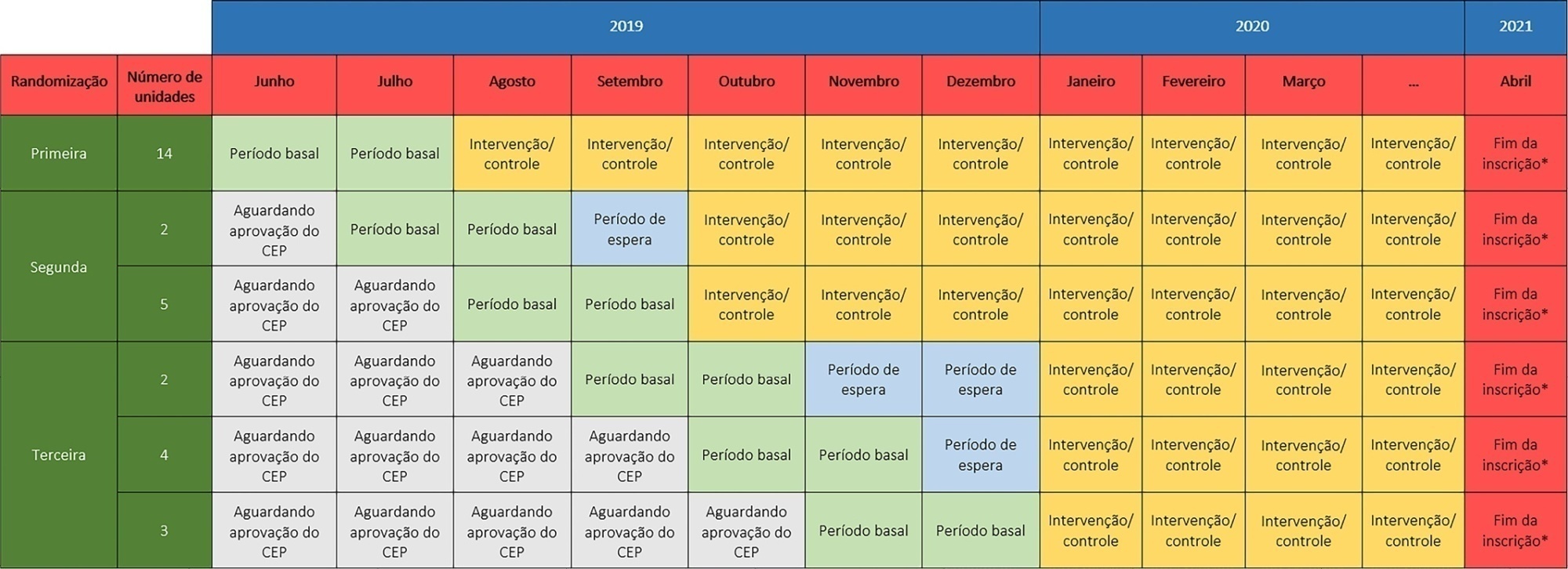
- Otavio Ranzani
-
Original Article
Statistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo, [ … ],
- Fernando Godinho Zampieri
Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
Views1Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
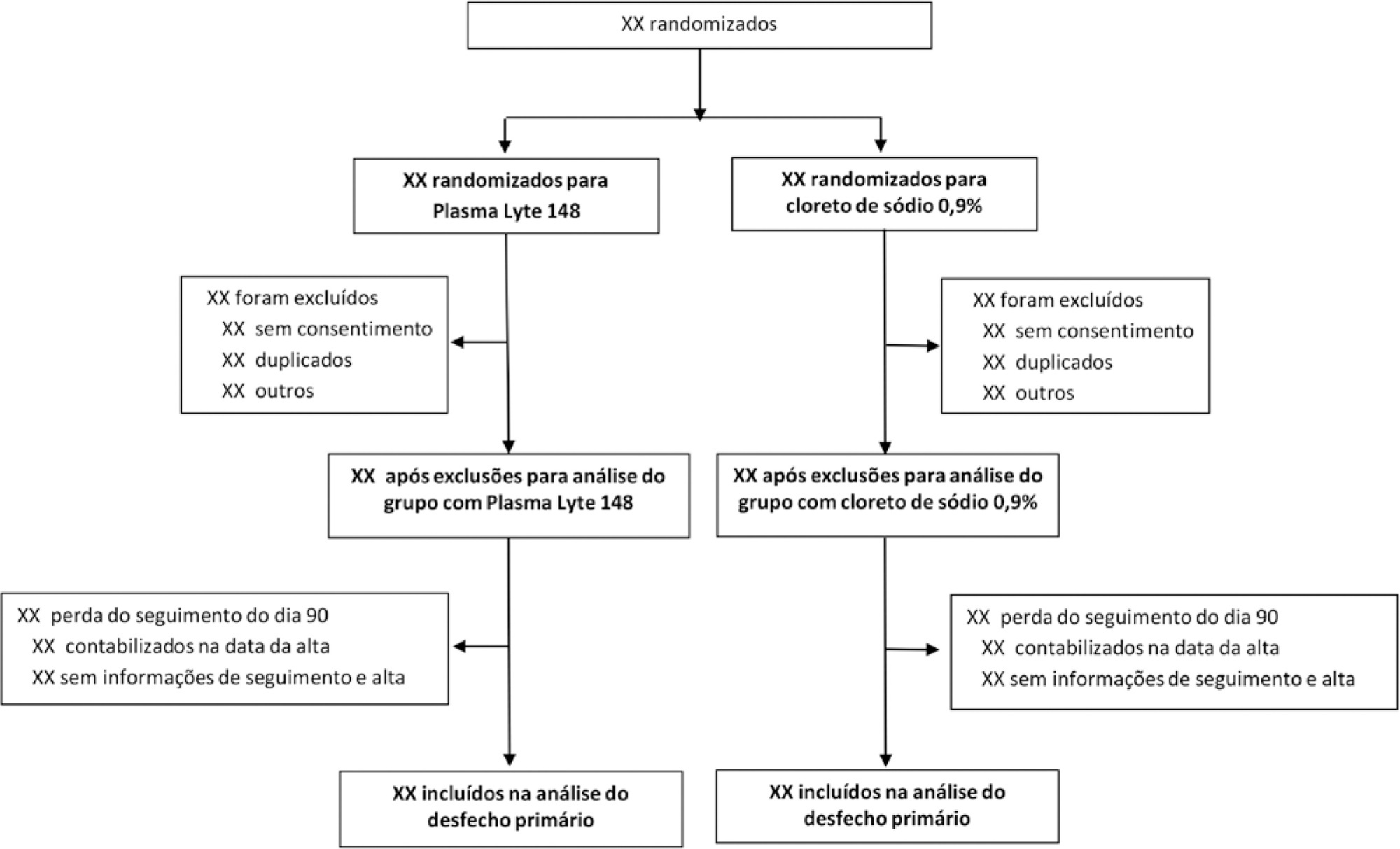
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
-
Original Article
Burnout syndrome and engagement among critical care providers: a cross-sectional study
- Carolina Sant’Anna Antunes Azevedo Castro,
- Karina Tavares Timenetsky,
- Marcelo Katz,
- Thiago Domingos Corrêa ,
- Andre Carvalho Felício, [ … ],
- Ary Serpa Neto
Abstract
Original ArticleBurnout syndrome and engagement among critical care providers: a cross-sectional study
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
- Carolina Sant’Anna Antunes Azevedo Castro,
- Karina Tavares Timenetsky,
- Marcelo Katz,
- Thiago Domingos Corrêa ,
- Andre Carvalho Felício,
- Tais Moriyama,
- Ana Merzel Kernkraut,
- Leonardo José Rolim Ferraz,
- Ary Serpa Neto
Views1ABSTRACT
Objective:
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
Methods:
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Results:
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 – 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 – 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
Conclusion:
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.
Keywords:Acute stress disordersBurnout, psychologicalDepressionIntensive care unitsStep-down unitWork engagementSee moreViews1Abstract
Original ArticleBurnout syndrome and engagement among critical care providers: a cross-sectional study
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
- Carolina Sant’Anna Antunes Azevedo Castro,
- Karina Tavares Timenetsky,
- Marcelo Katz,
- Thiago Domingos Corrêa ,
- Andre Carvalho Felício,
- Tais Moriyama,
- Ana Merzel Kernkraut,
- Leonardo José Rolim Ferraz,
- Ary Serpa Neto
Views1ABSTRACT
Objective:
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
Methods:
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Results:
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 – 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 – 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
Conclusion:
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.
Keywords:Acute stress disordersBurnout, psychologicalDepressionIntensive care unitsStep-down unitWork engagementSee more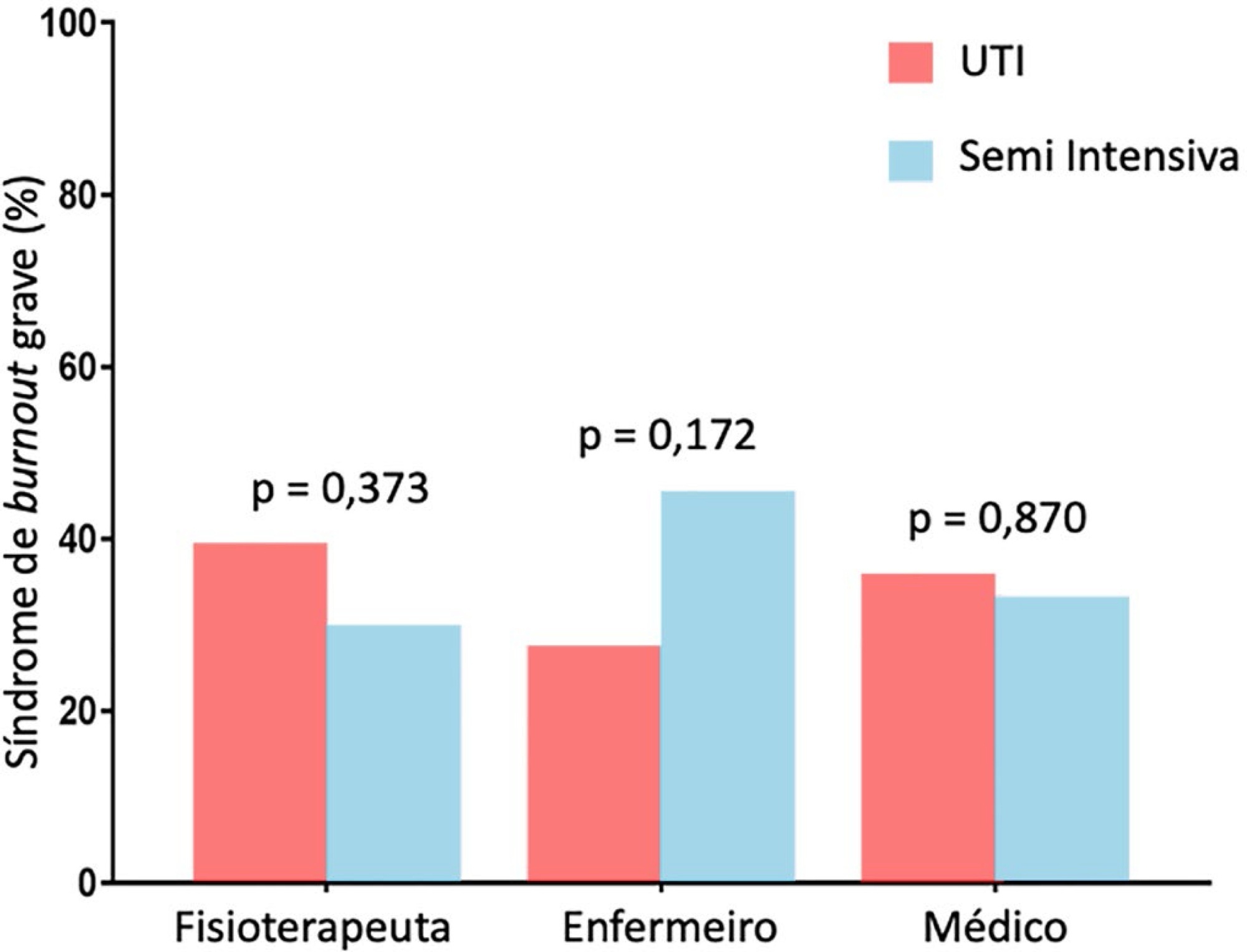
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more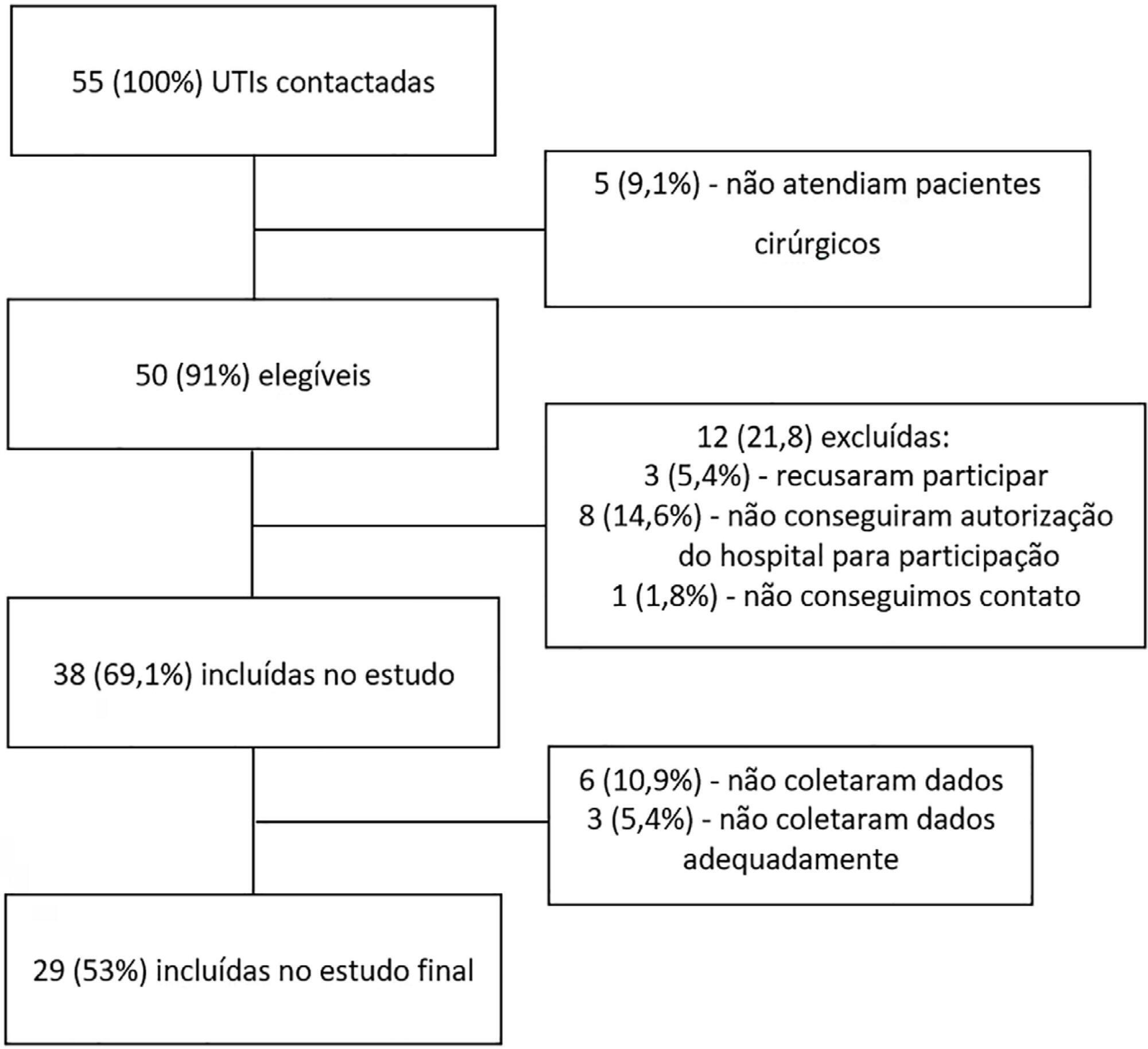
- João Manoel Silva Júnior
-
Review Articles
Extracorporeal membrane oxygenation: a literature review
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova, [ … ],
- Thiago Domingos Corrêa
Abstract
Review ArticlesExtracorporeal membrane oxygenation: a literature review
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova,
- Bruno de Arruda Bravim,
- Ary Serpa Neto,
- Thiago Domingos Corrêa
Views1ABSTRACT
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Keywords:Critical careExtracorporeal membrane oxygenationheart failureRespiration, artificialRespiratory insufficiencySee moreViews1Abstract
Review ArticlesExtracorporeal membrane oxygenation: a literature review
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
- Renato Carneiro de Freitas Chaves ,
- Roberto Rabello Filho,
- Karina Tavares Timenetsky,
- Fabio Tanzillo Moreira,
- Luiz Carlos da Silva Vilanova,
- Bruno de Arruda Bravim,
- Ary Serpa Neto,
- Thiago Domingos Corrêa
Views1ABSTRACT
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Keywords:Critical careExtracorporeal membrane oxygenationheart failureRespiration, artificialRespiratory insufficiencySee more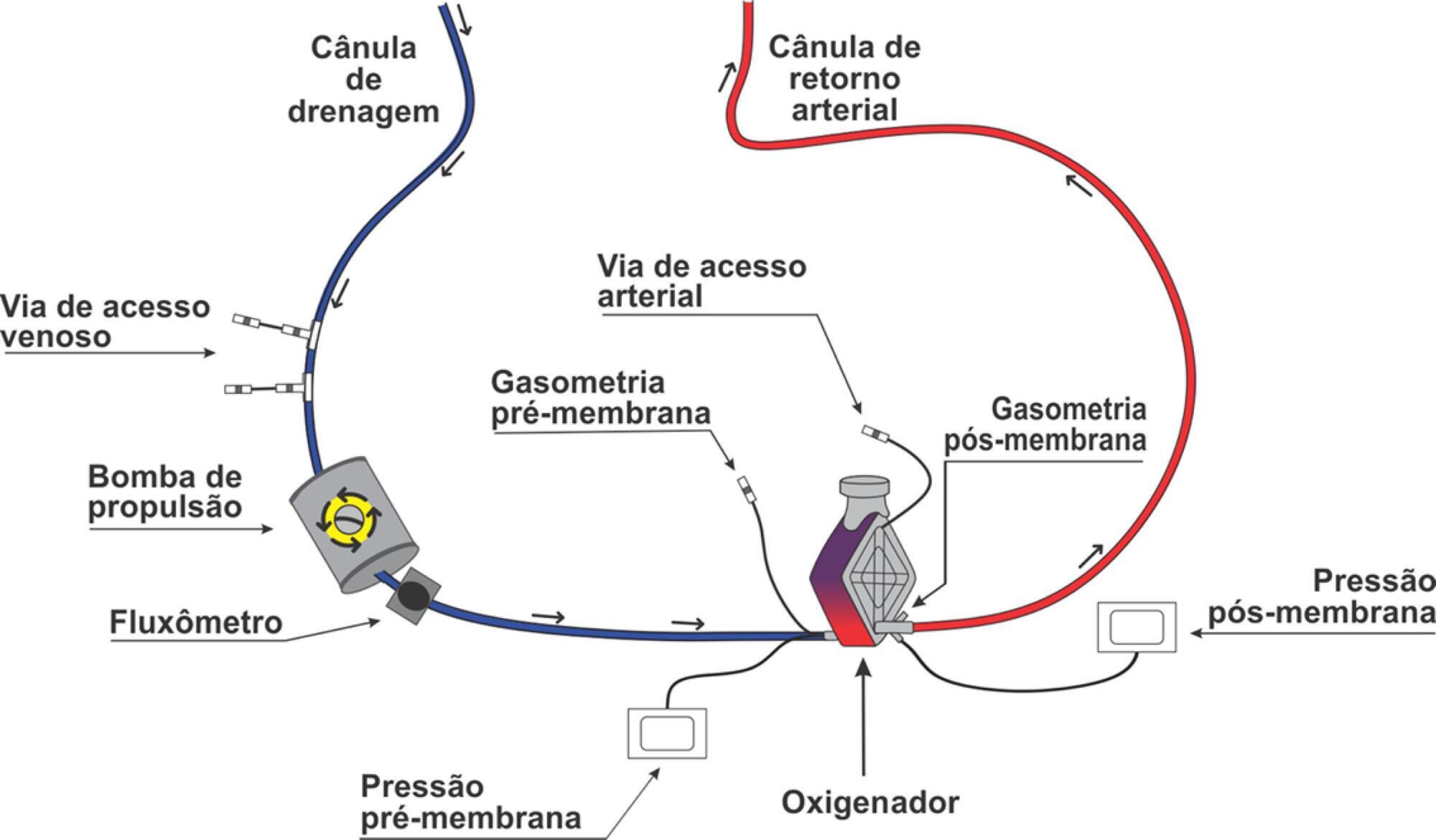
- Renato Carneiro de Freitas Chaves
-
Commentaries
First Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
Abstract
CommentariesFirst Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
DOI 10.5935/0103-507X.20180006
Views1“Health is a right of all and an obligation of the State, guaranteed by socioeconomic policies that seek reduction of the risk of disease and of other grievances and universal and equal access to the actions and services in its promotion, protection and recuperation.” Constitution of the Federative Republic of Brazil, 1988[…]See moreViews1Abstract
CommentariesFirst Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
DOI 10.5935/0103-507X.20180006
Views1“Health is a right of all and an obligation of the State, guaranteed by socioeconomic policies that seek reduction of the risk of disease and of other grievances and universal and equal access to the actions and services in its promotion, protection and recuperation.” Constitution of the Federative Republic of Brazil, 1988[…]See more -
Review Article
Early versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
Abstract
Review ArticleEarly versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
Views0ABSTRACT
Objective:
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
Methods:
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
Results:
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 – 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 – 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Conclusion:
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Keywords:Acute kidney injuryCritically illMeta-analysisRandomized controlled trialRenal replacement therapysystematic reviewSee moreViews0Abstract
Review ArticleEarly versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
Views0ABSTRACT
Objective:
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
Methods:
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
Results:
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 – 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 – 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Conclusion:
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Keywords:Acute kidney injuryCritically illMeta-analysisRandomized controlled trialRenal replacement therapysystematic reviewSee more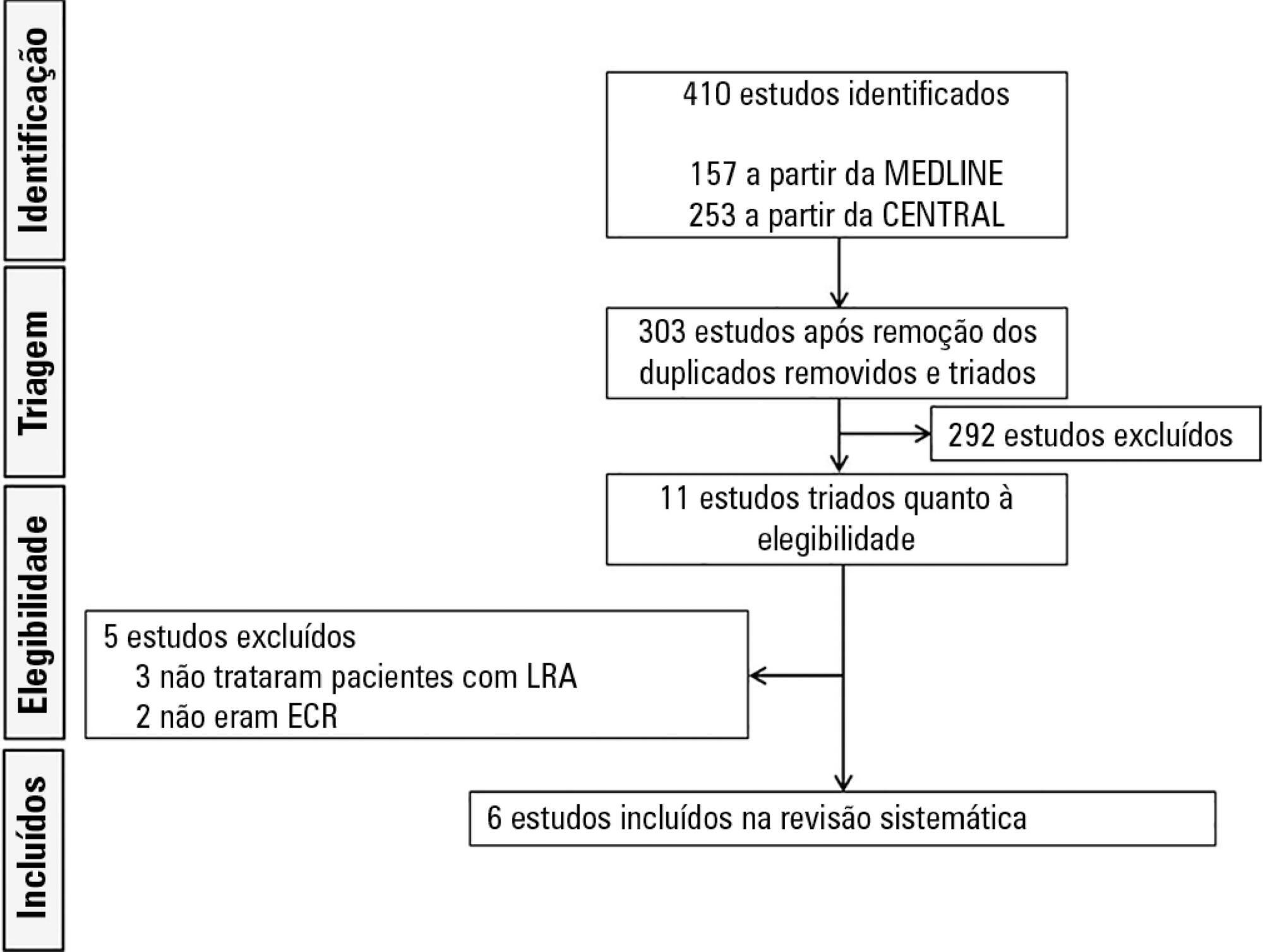
-
Review Article
The effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
Abstract
Review ArticleThe effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
DOI 10.5935/0103-507X.20180070
Views0See moreABSTRACT
Objective:
To evaluate the efficacy of high-flow nasal cannula in the prevention of intubation and re-intubation in critically ill patients compared to conventional oxygen therapy or noninvasive ventilation.
Methods:
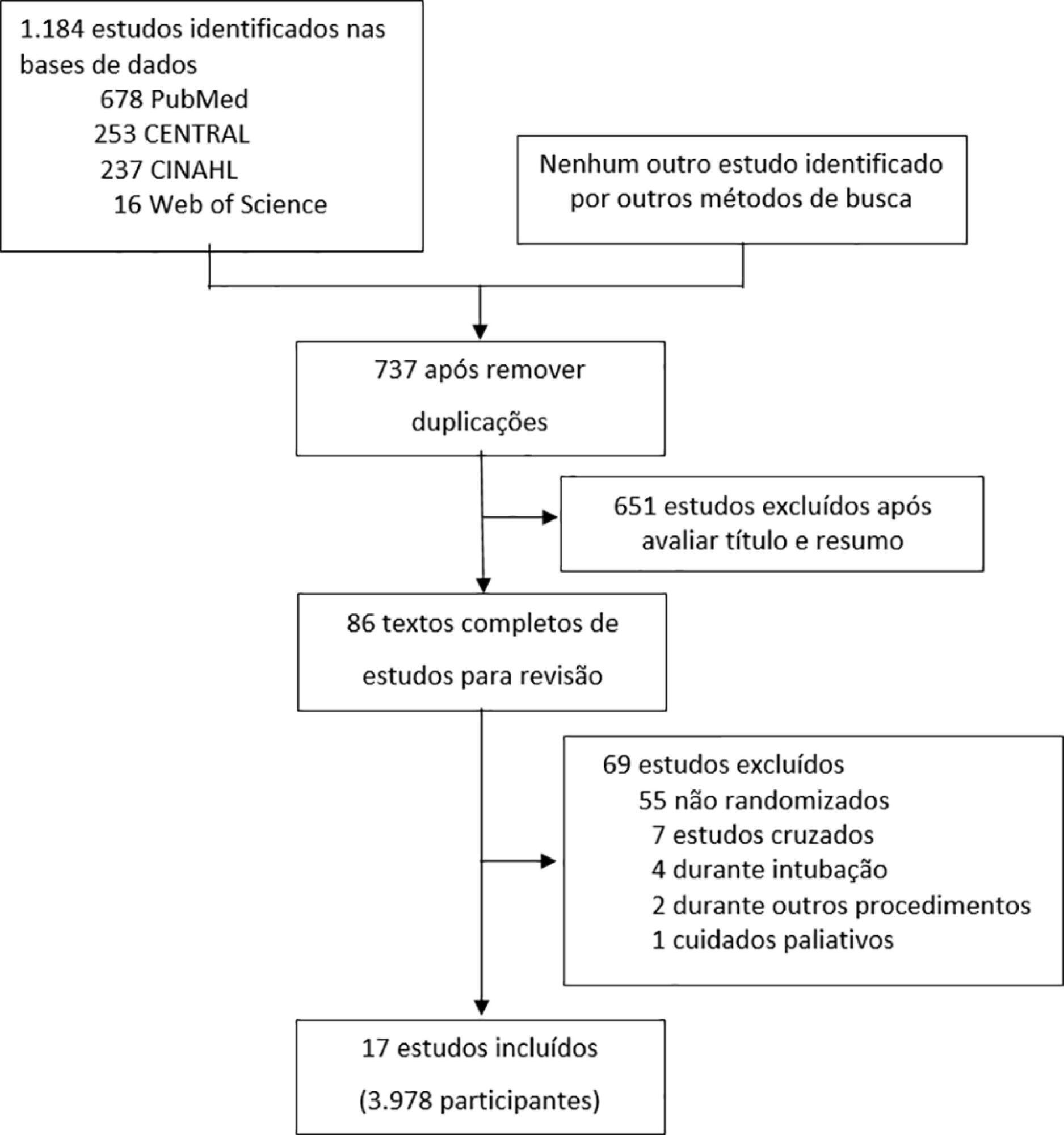
This systematic review was performed through an electronic database search of articles published from 1966 to April 2018. The primary outcome was the need for intubation or re-intubation. The secondary outcomes were therapy escalation, mortality at the longest follow-up, hospital mortality and the need for noninvasive ventilation.
Results:
Seventeen studies involving 3,978 patients were included. There was no reduction in the need for intubation or re-intubation with high-flow nasal cannula (OR 0.72; 95%CI 0.52 – 1.01; p = 0.056). There was no difference in the need for therapy escalation (OR 0.80, 95% CI 0.59 – 1.08, p = 0.144), mortality at the longest follow-up (OR 0.94; 95%CI 0.70 – 1.25; p = 0.667), hospital mortality (OR 0.84; 95%CI 0.56 – 1.26; p = 0.391) or noninvasive ventilation (OR 0.64, 95%CI 0.39 – 1.05, p = 0.075). In the trial sequential analysis, the number of events included was lower than the optimal information size with a global type I error > 0.05.
Conclusion:
In the present study and setting, high-flow nasal cannula was not associated with a reduction of the need for intubation or re-intubation in critically ill patients.
Views0Abstract
Review ArticleThe effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
DOI 10.5935/0103-507X.20180070
Views0See moreABSTRACT
Objective:
To evaluate the efficacy of high-flow nasal cannula in the prevention of intubation and re-intubation in critically ill patients compared to conventional oxygen therapy or noninvasive ventilation.
Methods:
This systematic review was performed through an electronic database search of articles published from 1966 to April 2018. The primary outcome was the need for intubation or re-intubation. The secondary outcomes were therapy escalation, mortality at the longest follow-up, hospital mortality and the need for noninvasive ventilation.
Results:
Seventeen studies involving 3,978 patients were included. There was no reduction in the need for intubation or re-intubation with high-flow nasal cannula (OR 0.72; 95%CI 0.52 – 1.01; p = 0.056). There was no difference in the need for therapy escalation (OR 0.80, 95% CI 0.59 – 1.08, p = 0.144), mortality at the longest follow-up (OR 0.94; 95%CI 0.70 – 1.25; p = 0.667), hospital mortality (OR 0.84; 95%CI 0.56 – 1.26; p = 0.391) or noninvasive ventilation (OR 0.64, 95%CI 0.39 – 1.05, p = 0.075). In the trial sequential analysis, the number of events included was lower than the optimal information size with a global type I error > 0.05.
Conclusion:
In the present study and setting, high-flow nasal cannula was not associated with a reduction of the need for intubation or re-intubation in critically ill patients.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness ICU Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis