heart failure Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240196en
DOI 10.62675/2965-2774.20240196-en
To provide insights into the potential benefits of goal-directed therapy guided by FloTrac in reducing postoperative complications and improving outcomes.
We performed a systematic review and meta-analysis of randomized controlled trials to evaluate goal-directed therapy guided by FloTrac in major surgery, comparing goal-directed therapy with usual care or invasive monitoring in cardiac and noncardiac surgery subgroups. The quality of the articles and evidence were evaluated with a risk of bias tool and GRADE.
We included 29 randomized controlled trials with 3,468 patients. Goal-directed therapy significantly reduced the duration of hospital stay (mean difference -1.43 days; 95%CI 2.07 to -0.79; I2 81%), intensive care unit stay (mean difference -0.77 days; 95%CI -1.18 to -0.36; I2 93%), and mechanical ventilation (mean difference -2.48 hours, 95%CI -4.10 to -0.86, I2 63%). There was no statistically significant difference in mortality, myocardial infarction, acute kidney injury or hypotension, but goal-directed therapy significantly reduced the risk of heart failure or pulmonary edema (RR 0.46; 95%CI 0.23 - 0.92; I2 0%).
Goal-directed therapy guided by the FloTrac sensor improved clinical outcomes and shortened the length of stay in the hospital and intensive care unit in patients undergoing major surgery. Further research can validate these results using specific protocols and better understand the potential benefits of FloTrac beyond these outcomes.
Abstract
Crit Care Sci. 2024;36:e20240196en
DOI 10.62675/2965-2774.20240196-en
To provide insights into the potential benefits of goal-directed therapy guided by FloTrac in reducing postoperative complications and improving outcomes.
We performed a systematic review and meta-analysis of randomized controlled trials to evaluate goal-directed therapy guided by FloTrac in major surgery, comparing goal-directed therapy with usual care or invasive monitoring in cardiac and noncardiac surgery subgroups. The quality of the articles and evidence were evaluated with a risk of bias tool and GRADE.
We included 29 randomized controlled trials with 3,468 patients. Goal-directed therapy significantly reduced the duration of hospital stay (mean difference -1.43 days; 95%CI 2.07 to -0.79; I2 81%), intensive care unit stay (mean difference -0.77 days; 95%CI -1.18 to -0.36; I2 93%), and mechanical ventilation (mean difference -2.48 hours, 95%CI -4.10 to -0.86, I2 63%). There was no statistically significant difference in mortality, myocardial infarction, acute kidney injury or hypotension, but goal-directed therapy significantly reduced the risk of heart failure or pulmonary edema (RR 0.46; 95%CI 0.23 - 0.92; I2 0%).
Goal-directed therapy guided by the FloTrac sensor improved clinical outcomes and shortened the length of stay in the hospital and intensive care unit in patients undergoing major surgery. Further research can validate these results using specific protocols and better understand the potential benefits of FloTrac beyond these outcomes.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):340-346
DOI 10.5935/0103-507X.20190049
To identify the underlying factors that affect fluid resuscitation in septic patients.
The present study was a case-control study of 181 consecutive patients admitted to a Medical Intensive Care Unit between 2012 and 2016 with a diagnosis of sepsis. Demographic, clinical, radiological and laboratory data were analyzed.
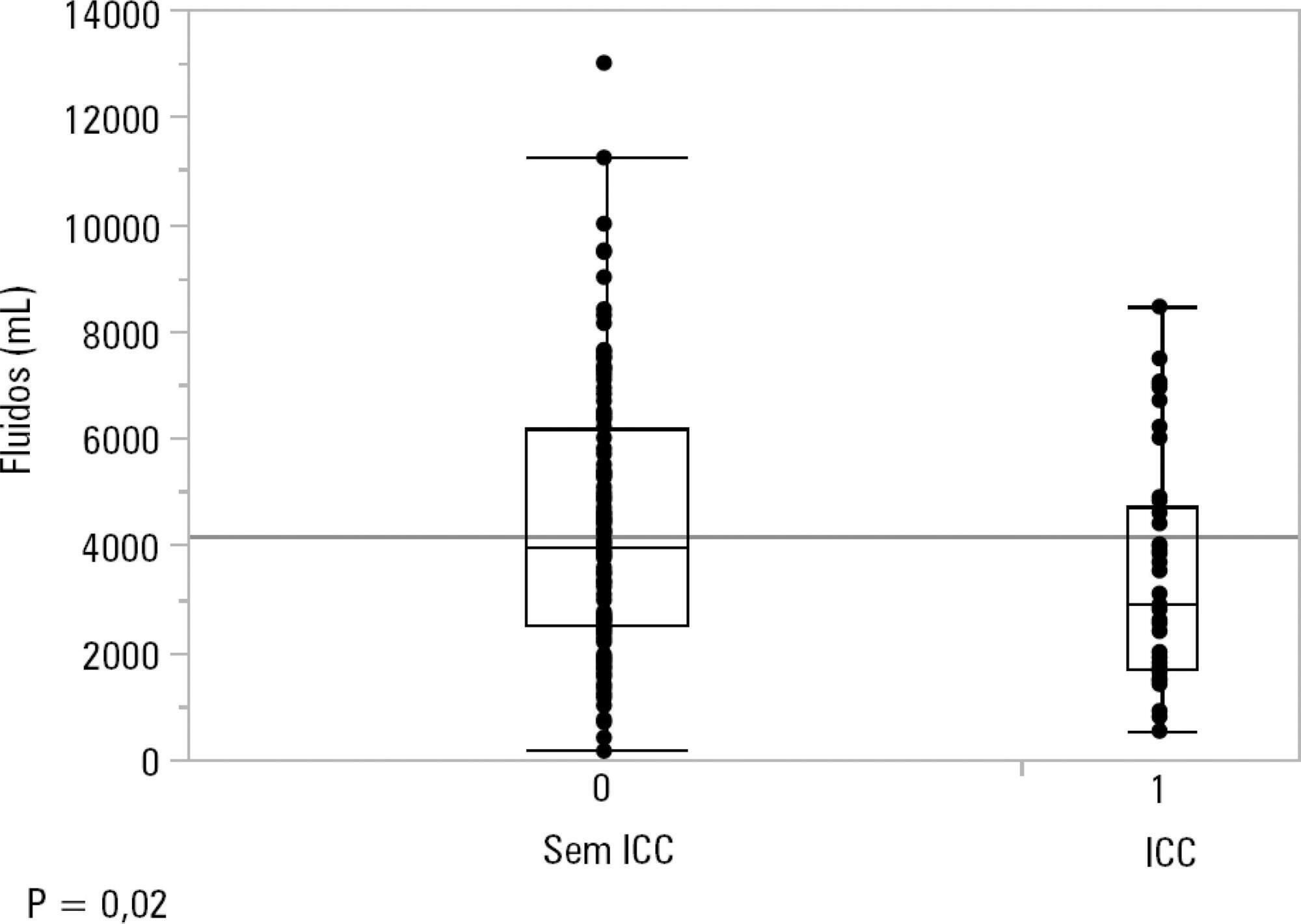
One hundred-thirty patients (72%) received ≥ 30mL/kg of IV fluids on admission. On univariate analyses, a past history of coronary artery disease and heart failure was associated with less fluid therapy. On multivariate analyses, a history of heart failure (OR = 2.31; 95%CI 1.04 - 5.14) remained significantly associated with receiving less IV fluids. Left ventricular ejection fraction, systolic/diastolic function, left ventricular hypertrophy and pulmonary hypertension were not associated with IV fluids. The amount of IV fluids was not associated with differences in mortality. During the first 24 hours, patients with a past history of heart failure received 2,900mLof IV fluids [1,688 - 4,714mL] versus 3,977mL [2,500 - 6,200mL] received by those without a history of heart failure, p = 0.02.
Septic patients with a past history of heart failure received 1L less IV fluids in the first 24 hours with no difference in mortality.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):340-346
DOI 10.5935/0103-507X.20190049
To identify the underlying factors that affect fluid resuscitation in septic patients.
The present study was a case-control study of 181 consecutive patients admitted to a Medical Intensive Care Unit between 2012 and 2016 with a diagnosis of sepsis. Demographic, clinical, radiological and laboratory data were analyzed.
One hundred-thirty patients (72%) received ≥ 30mL/kg of IV fluids on admission. On univariate analyses, a past history of coronary artery disease and heart failure was associated with less fluid therapy. On multivariate analyses, a history of heart failure (OR = 2.31; 95%CI 1.04 - 5.14) remained significantly associated with receiving less IV fluids. Left ventricular ejection fraction, systolic/diastolic function, left ventricular hypertrophy and pulmonary hypertension were not associated with IV fluids. The amount of IV fluids was not associated with differences in mortality. During the first 24 hours, patients with a past history of heart failure received 2,900mLof IV fluids [1,688 - 4,714mL] versus 3,977mL [2,500 - 6,200mL] received by those without a history of heart failure, p = 0.02.
Septic patients with a past history of heart failure received 1L less IV fluids in the first 24 hours with no difference in mortality.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
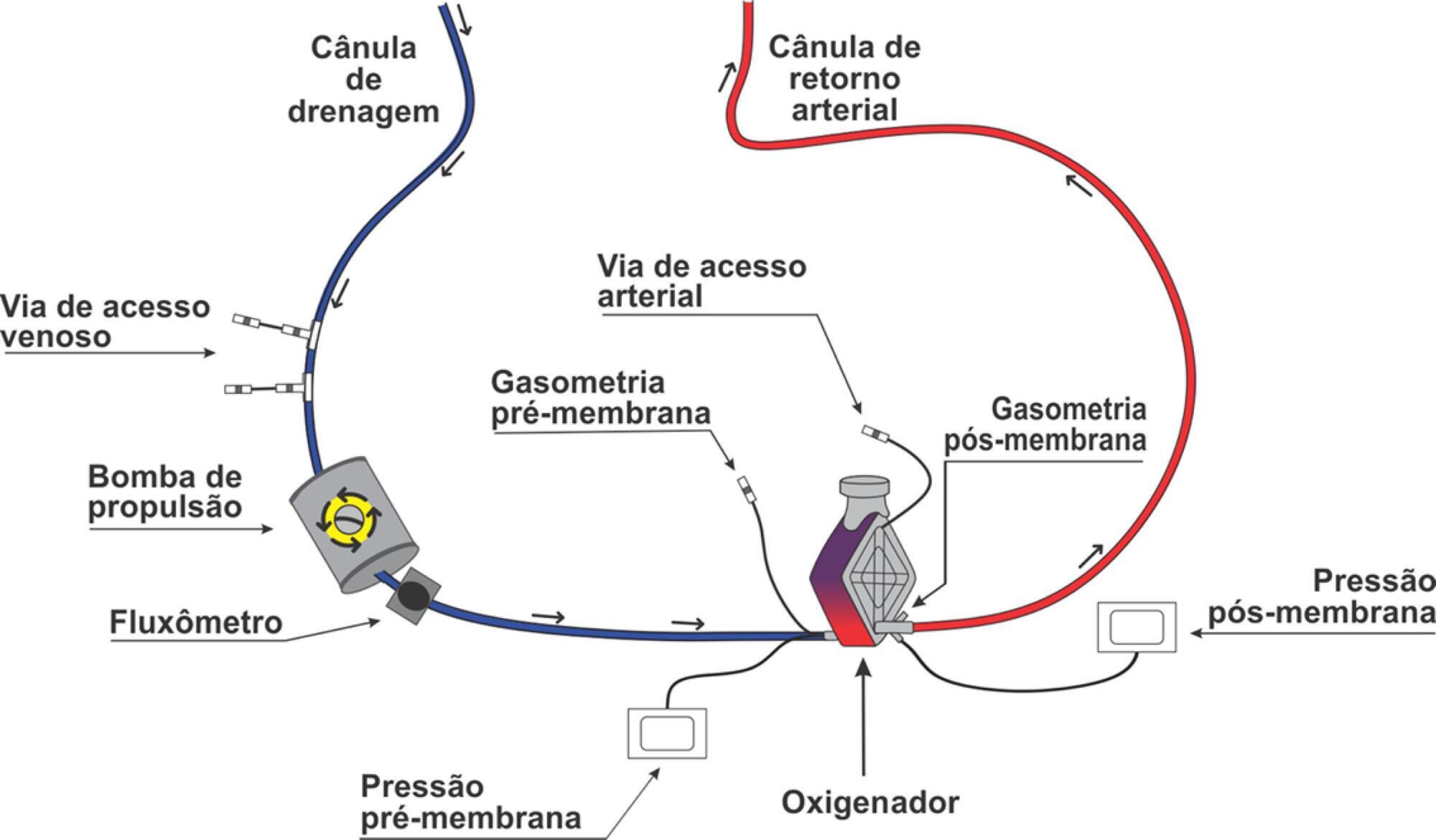
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.

Abstract
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
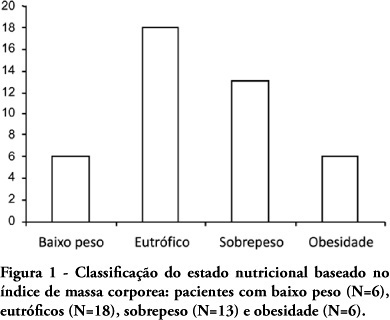
OBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
OBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
BACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
BACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)