Renal failure Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2010;22(2):206-211
DOI 10.1590/S0103-507X2010000200016
In patients with renal failure, encephalopathy is a common problem that may be caused by uremia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolyte disturbances or drug toxicity. In general, encephalopathy presents with a symptom complex progressing from mild sensorial clouding to delirium and coma. This review discusses important issues regarding the mechanisms underlying the pathophysiology of uremic encephalopathy. The pathophysiology of uremic encephalopathy up to now is uncertain, but several factors have been postulated to be involved; it is a complex and probably multifactorial process. Hormonal disturbances, oxidative stress, accumulation of metabolites, imbalance in excitatory and inhibitory neurotransmitters, and disturbance of the intermediary metabolism have been identified as contributing factors. Despite continuous therapeutic progress, most neurological complications of uremia, like uremic encephalopathy, fail to fully respond to dialysis and many are elicited or aggravated by dialysis or renal transplantation. On the other hand, previous studies showed that antioxidant therapy could be used as an adjuvant therapy for the treatment of these neurological complications.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):206-211
DOI 10.1590/S0103-507X2010000200016
In patients with renal failure, encephalopathy is a common problem that may be caused by uremia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolyte disturbances or drug toxicity. In general, encephalopathy presents with a symptom complex progressing from mild sensorial clouding to delirium and coma. This review discusses important issues regarding the mechanisms underlying the pathophysiology of uremic encephalopathy. The pathophysiology of uremic encephalopathy up to now is uncertain, but several factors have been postulated to be involved; it is a complex and probably multifactorial process. Hormonal disturbances, oxidative stress, accumulation of metabolites, imbalance in excitatory and inhibitory neurotransmitters, and disturbance of the intermediary metabolism have been identified as contributing factors. Despite continuous therapeutic progress, most neurological complications of uremia, like uremic encephalopathy, fail to fully respond to dialysis and many are elicited or aggravated by dialysis or renal transplantation. On the other hand, previous studies showed that antioxidant therapy could be used as an adjuvant therapy for the treatment of these neurological complications.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
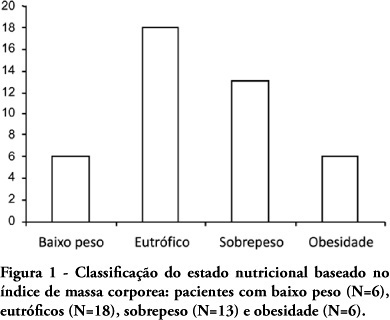
OBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):124-128
DOI 10.1590/S0103-507X2009000200002
OBJECTIVE: Evaluate the nutritional status of patients with cardiac disease and concomitant renal dysfunction requiring renal replacement therapy. METHODS: Patients with cardiac disease and renal failure receiving renal replacement therapy, admitted to an intensive care unit, were submitted to nutritional evaluation, by use of anthropometric measurements and laboratory data. RESULTS: We studied 43 patients, mean age 64±15 years, 26 were men. The mean left ventricular ejection fraction was 0.36±0.16. Analysis of anthropometric measurements, based on body mass index disclosed that, 18 patients were normal, 6 were underweight and 19 were overweight or obese. Based on measurement of triceps skinfold thickness, 16 patients were considered normal and 27 had some degree of depletion. Measurements of midarm circumference and midarm muscular circumference showed 41 patients with some degree of depletion. Laboratory data revealed 28 patients with depletion based on albumin levels and 27 with depletion based on lymphocyte count. CONCLUSIONS: Malnutrition is common in critically ill patients with cardiac disease and renal failure receiving renal replacement therapy. Nutritional assessment based on body mass index did not prove to be a good index for diagnosis of nutritional disorders. The nutritional evaluation must be complemented in order to identify malnutrition and introduce early nutritional support.