
You searched for:"Guilherme Schettino"
We found (7) results for your search.-
Special Article
Statistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
- Otavio Ranzani
 ,
, - Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz , [ … ],
- Danilo Teixeira Noritomi
Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee moreViews2

Abstract
Special ArticleStatistical analysis of a cluster-randomized clinical trial on adult general intensive care units in Brazil: TELE-critical care verSus usual Care On ICU PErformance (TELESCOPE) trial
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
- Otavio Ranzani ,
- Adriano José Pereira ,
- Maura Cristina dos Santos ,
- Thiago Domingos Corrêa ,
- Leonardo Jose Rolim Ferraz ,
- Eduardo Cordioli ,
- Renata Albaladejo Morbeck ,
- Otávio Berwanger ,
- Lúbia Caus de Morais ,
- Guilherme Schettino ,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa ,
- Rodrigo Santos Biondi ,
- Jorge Ibrain Figueira Salluh ,
- Luciano César Pontes de Azevedo ,
- Ary Serpa Neto ,
- Danilo Teixeira Noritomi
Views2ABSTRACT
Objective:
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
Methods:
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
Conclusion:
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Keywords:BrazilCritical careData interpretation, statisticalHospital mortalityIntensive care unitsLength of stayPatient care teamResearch designTelemedicineSee more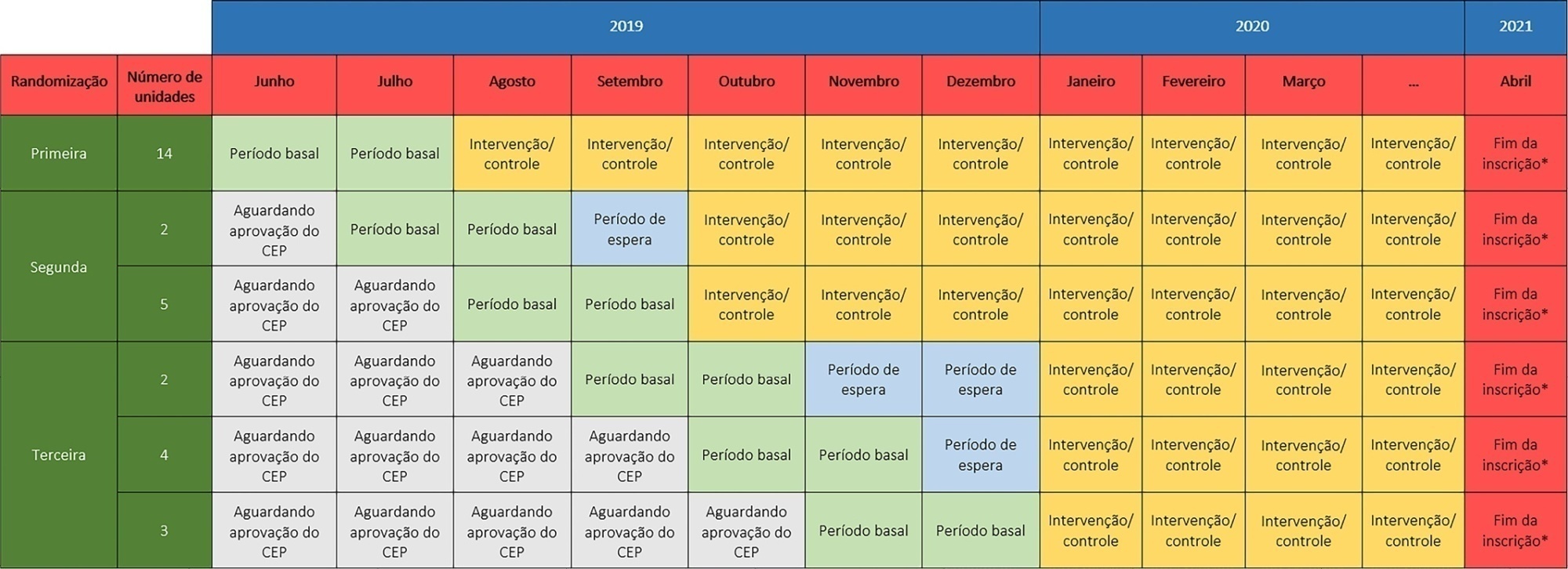
- Otavio Ranzani
-
Original Articles
Intensive care unit visitation policies in Brazil: a multicenter survey
Rev Bras Ter Intensiva. 2014;26(4):339-346
Abstract
Original ArticlesIntensive care unit visitation policies in Brazil: a multicenter survey
Rev Bras Ter Intensiva. 2014;26(4):339-346
DOI 10.5935/0103-507X.20140052
Views0Objective:
This study aimed to determine which visitation policy was the most predominant in Brazilian intensive care units and what amenities were provided to visitors.
Methods:
Eight hundred invitations were sent to the e-mail addresses of intensivist physicians and nurses who were listed in the research groups of the Brazilian Association of Intensive Care Network and the Brazilian Research in Intensive Care Network. The e-mail contained a link to a 33-item questionnaire about the profile of their intensive care unit.
Results:
One hundred sixty-two questionnaires from intensive care units located in all regions of the country, but predominantly in the Southeast and South (58% and 16%), were included in the study. Only 2.6% of the intensive care units reported having liberal visitation policies, while 45.1% of the intensive care units allowed 2 visitation periods and 69.1% allowed 31-60 minutes of visitation per period. In special situations, such as end-of-life cases, 98.7% of them allowed flexible visitation. About half of them (50.8%) did not offer any bedside amenities for visitors. Only 46.9% of the intensive care units had a family meeting room, and 37% did not have a waiting room.
Conclusion:
Restrictive visitation policies are predominant in Brazilian intensive care units, with most of them allowing just two periods of visitation per day. There is also a lack of amenities for visitors.
Keywords:Intensive care units/standardsPatient-centered-care/standardsProfessional-family relationsProfessional-patient relationsQuestionnairesVisitors to patientsSee moreViews0Abstract
Original ArticlesIntensive care unit visitation policies in Brazil: a multicenter survey
Rev Bras Ter Intensiva. 2014;26(4):339-346
DOI 10.5935/0103-507X.20140052
Views0Objective:
This study aimed to determine which visitation policy was the most predominant in Brazilian intensive care units and what amenities were provided to visitors.
Methods:
Eight hundred invitations were sent to the e-mail addresses of intensivist physicians and nurses who were listed in the research groups of the Brazilian Association of Intensive Care Network and the Brazilian Research in Intensive Care Network. The e-mail contained a link to a 33-item questionnaire about the profile of their intensive care unit.
Results:
One hundred sixty-two questionnaires from intensive care units located in all regions of the country, but predominantly in the Southeast and South (58% and 16%), were included in the study. Only 2.6% of the intensive care units reported having liberal visitation policies, while 45.1% of the intensive care units allowed 2 visitation periods and 69.1% allowed 31-60 minutes of visitation per period. In special situations, such as end-of-life cases, 98.7% of them allowed flexible visitation. About half of them (50.8%) did not offer any bedside amenities for visitors. Only 46.9% of the intensive care units had a family meeting room, and 37% did not have a waiting room.
Conclusion:
Restrictive visitation policies are predominant in Brazilian intensive care units, with most of them allowing just two periods of visitation per day. There is also a lack of amenities for visitors.
Keywords:Intensive care units/standardsPatient-centered-care/standardsProfessional-family relationsProfessional-patient relationsQuestionnairesVisitors to patientsSee more
-
Original Article
In vitro and in vivo validation of stored swine erythrocyte viability to establish an experimental model of homologous red blood cell transfusion: a pilot study
Rev Bras Ter Intensiva. 2014;26(3):287-291
Abstract
Original ArticleIn vitro and in vivo validation of stored swine erythrocyte viability to establish an experimental model of homologous red blood cell transfusion: a pilot study
Rev Bras Ter Intensiva. 2014;26(3):287-291
DOI 10.5935/0103-507X.20140040
Views0See moreObjective:
To develop experimental models of erythrocyte transfusion, the first step is to ensure the viability of the red blood cells transfused. In this pilot study, we assessed the viability of transfused red blood cells with validation in vitro and in vivo of homologous swine erythrocytes stored for 14 days.
Methods:
Blood collected from one Agroceres® swine was stored in two red blood cell units. In vivo validation was performed by labeling the red blood cells with Na2 51CrO4 and recovering the viable erythrocytes after 24 hours of infusion in one autologous and four homologous animals. In vitro validation was performed at baseline and after 14 days in sixteen red blood cell units by measuring hemoglobin, hematocrit, hemolysis index and free hemoglobin. A post-mortem splenectomy was performed to evaluate the splenic sequestration of erythrocytes, and the radioactivity of the supernatant samples was counted to evaluate intravascular hemolysis.
Results:
After 14 days of storage, the red blood cell units had lower volumes and equivalent total concentrations of hemoglobin and hematocrit compared to human standards. The free hemoglobin concentration increased from 31.0±9.3 to 112.4±31.4mg/dL (p<0.001), and the hemolysis index increased from 0.1±0.1 to 0.5±0.1% (p<0.001). However, these tests were within the acceptable range for human standards. The percentage of radioactivity in supernatant samples was similar at baseline and after 24 hours, thus excluding significant hemolysis. No evidence of splenic sequestration of radioactive erythrocytes was found.
Conclusion:
Swine red blood cells stored for 14 days are viable and can be used in experimental studies of transfusion. These validation experiments are important to aid investigators in establishing experimental models of transfusion.
Views0Abstract
Original ArticleIn vitro and in vivo validation of stored swine erythrocyte viability to establish an experimental model of homologous red blood cell transfusion: a pilot study
Rev Bras Ter Intensiva. 2014;26(3):287-291
DOI 10.5935/0103-507X.20140040
Views0See moreObjective:
To develop experimental models of erythrocyte transfusion, the first step is to ensure the viability of the red blood cells transfused. In this pilot study, we assessed the viability of transfused red blood cells with validation in vitro and in vivo of homologous swine erythrocytes stored for 14 days.
Methods:
Blood collected from one Agroceres® swine was stored in two red blood cell units. In vivo validation was performed by labeling the red blood cells with Na2 51CrO4 and recovering the viable erythrocytes after 24 hours of infusion in one autologous and four homologous animals. In vitro validation was performed at baseline and after 14 days in sixteen red blood cell units by measuring hemoglobin, hematocrit, hemolysis index and free hemoglobin. A post-mortem splenectomy was performed to evaluate the splenic sequestration of erythrocytes, and the radioactivity of the supernatant samples was counted to evaluate intravascular hemolysis.
Results:
After 14 days of storage, the red blood cell units had lower volumes and equivalent total concentrations of hemoglobin and hematocrit compared to human standards. The free hemoglobin concentration increased from 31.0±9.3 to 112.4±31.4mg/dL (p<0.001), and the hemolysis index increased from 0.1±0.1 to 0.5±0.1% (p<0.001). However, these tests were within the acceptable range for human standards. The percentage of radioactivity in supernatant samples was similar at baseline and after 24 hours, thus excluding significant hemolysis. No evidence of splenic sequestration of radioactive erythrocytes was found.
Conclusion:
Swine red blood cells stored for 14 days are viable and can be used in experimental studies of transfusion. These validation experiments are important to aid investigators in establishing experimental models of transfusion.

-
Consenso Brasileiro de Monitorização e Suporte Hemodinâmico
Part II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoPart II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
Views1See moreBACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Views1Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoPart II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
Views1See moreBACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
-
Consenso Brasileiro de Monitorização e Suporte Hemodinâmico
Brazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoBrazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
Views0See moreBACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the ” gold standard” to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Views0Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoBrazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
Views0See moreBACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the ” gold standard” to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
-
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
Abstract
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
DOI 10.1590/S0103-507X2006000200009
Views0See moreBACKGROUND AND OBJECTIVES: The main cardiovascular function is to maintain the adequate perfusion e oxygen delivery to the cells. Physiologically, this is controlled by the cellular metabolic rate. The critically ill patients are in high danger of tissue hipoperfusion and this is directly related to cellular injury and organ dysfunction. Therefore, the tissue perfusion monitoring makes part and is indissociated of hemodynamic evaluation of the critically ill patient and is indicated to all this patients. The objective was to define recommendations about clinical utility of different tolls to bedside perfusion monitoring. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MedLine in the period from 1996 to 2004. RESULTS: Recommendations were done about the utility of clinical monitoring of tissue perfusion, temperature gradient and transcutaneous oxygen monitoring, serum lactate, base excess, SvO² and ScvO², gastric and sublingual capnometry, CO² venous-arterial gradient and Orthogonal Polarization Spectral (OPS). CONCLUSIONS: The homodynamic compensation of a critically ill patient isn’t complete unless the tissue perfusion is corrected. Many different methods of monitoring is available and are useful in clinical practice, however, none has accuracy and effectiveness characteristics to be used independently of clinical context.
Views0Abstract
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
DOI 10.1590/S0103-507X2006000200009
Views0See moreBACKGROUND AND OBJECTIVES: The main cardiovascular function is to maintain the adequate perfusion e oxygen delivery to the cells. Physiologically, this is controlled by the cellular metabolic rate. The critically ill patients are in high danger of tissue hipoperfusion and this is directly related to cellular injury and organ dysfunction. Therefore, the tissue perfusion monitoring makes part and is indissociated of hemodynamic evaluation of the critically ill patient and is indicated to all this patients. The objective was to define recommendations about clinical utility of different tolls to bedside perfusion monitoring. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MedLine in the period from 1996 to 2004. RESULTS: Recommendations were done about the utility of clinical monitoring of tissue perfusion, temperature gradient and transcutaneous oxygen monitoring, serum lactate, base excess, SvO² and ScvO², gastric and sublingual capnometry, CO² venous-arterial gradient and Orthogonal Polarization Spectral (OPS). CONCLUSIONS: The homodynamic compensation of a critically ill patient isn’t complete unless the tissue perfusion is corrected. Many different methods of monitoring is available and are useful in clinical practice, however, none has accuracy and effectiveness characteristics to be used independently of clinical context.
-
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
Abstract
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
Views0See moreBACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
Views0Abstract
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
Views0See moreBACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis