Cardiac output Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(1):107-111
DOI 10.5935/2965-2774.20230305-pt
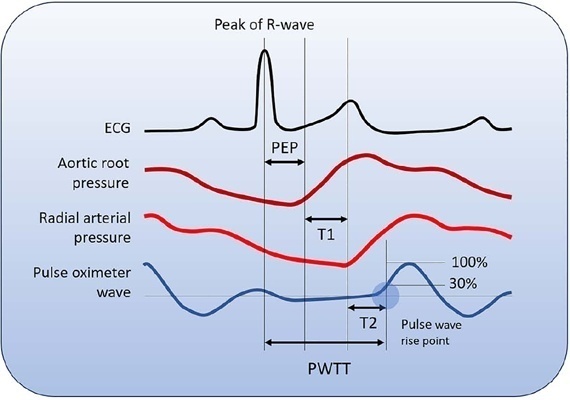
Cardiac output is an essential determinant of oxygen delivery, although unreliably measured on clinical examination and routine monitoring. Unfortunately, cardiac output monitoring is rarely performed in pediatric critical care medicine, with a limited availability of accurate methods for children. Herein, we report two pediatric cases in which noninvasive pulse-wave transit time-based cardiac output monitoring (esCCO, Nihon Kohden, Tokyo, Japan) was used. The esCCO system calculates cardiac output continuously by using the negative correlation between stroke volume and pulse wave transit time and requires only electrocardiogram monitoring, noninvasive blood pressure, and pulse oximetry signals. Before starting its use, esCCO should be calibrated, which can be done using patient information (gender, age, height, and body weight) or entering cardiac output values obtained by other methods. In both cases, when calibrations were performed using patient information, the agreement between esCCO and echocardiographic measurements was poor. However, after calibration with transthoracic echocardiography, the cardiac output values obtained by both methods remained similar after 2 hours and 18 hours. The results indicate that the esCCO system is suitable for use in children; however, further studies are needed to optimize its algorithm and determine its accuracy, precision, and trend in children.
Abstract
Crit Care Sci. 2023;35(1):107-111
DOI 10.5935/2965-2774.20230305-pt
Cardiac output is an essential determinant of oxygen delivery, although unreliably measured on clinical examination and routine monitoring. Unfortunately, cardiac output monitoring is rarely performed in pediatric critical care medicine, with a limited availability of accurate methods for children. Herein, we report two pediatric cases in which noninvasive pulse-wave transit time-based cardiac output monitoring (esCCO, Nihon Kohden, Tokyo, Japan) was used. The esCCO system calculates cardiac output continuously by using the negative correlation between stroke volume and pulse wave transit time and requires only electrocardiogram monitoring, noninvasive blood pressure, and pulse oximetry signals. Before starting its use, esCCO should be calibrated, which can be done using patient information (gender, age, height, and body weight) or entering cardiac output values obtained by other methods. In both cases, when calibrations were performed using patient information, the agreement between esCCO and echocardiographic measurements was poor. However, after calibration with transthoracic echocardiography, the cardiac output values obtained by both methods remained similar after 2 hours and 18 hours. The results indicate that the esCCO system is suitable for use in children; however, further studies are needed to optimize its algorithm and determine its accuracy, precision, and trend in children.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
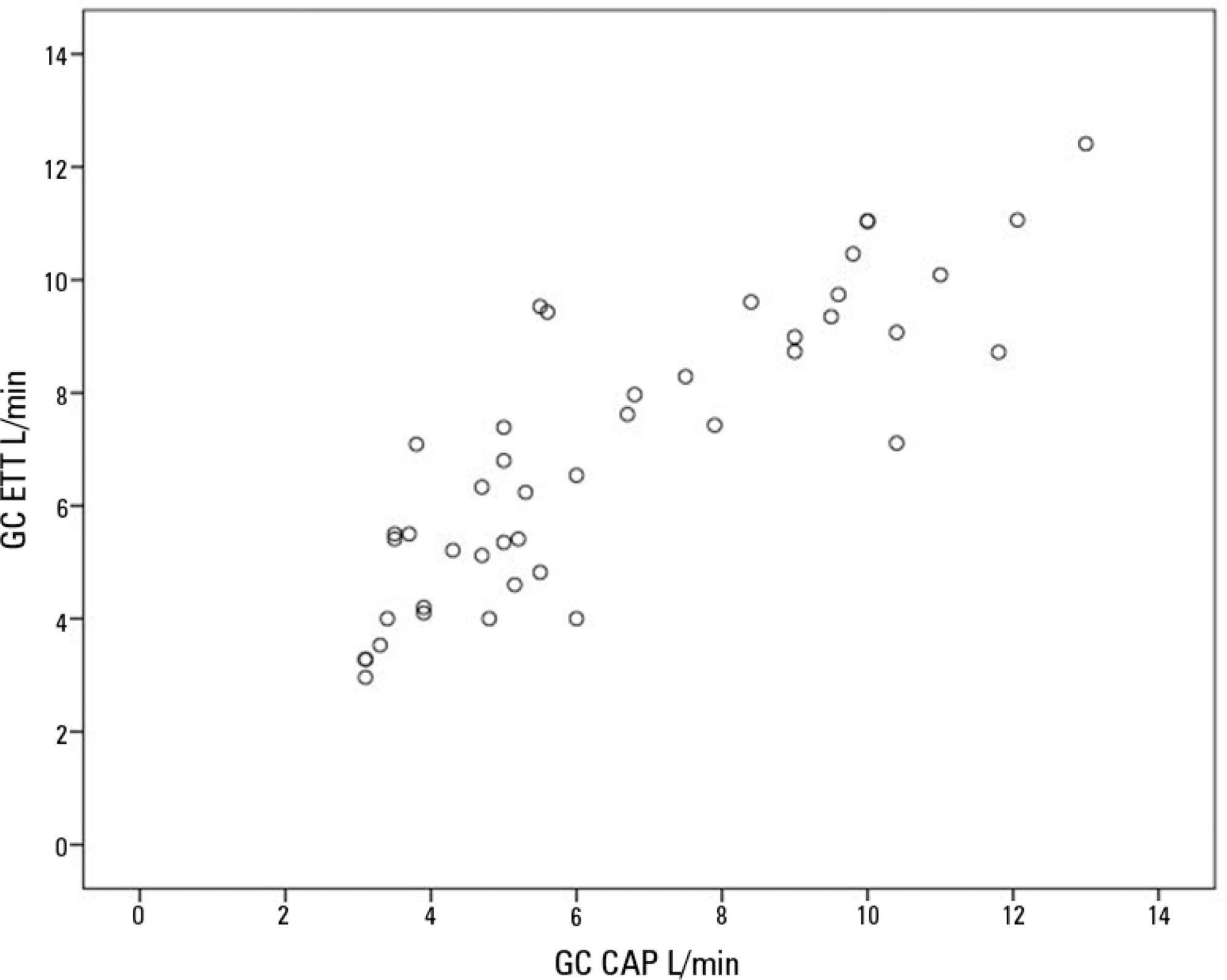
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
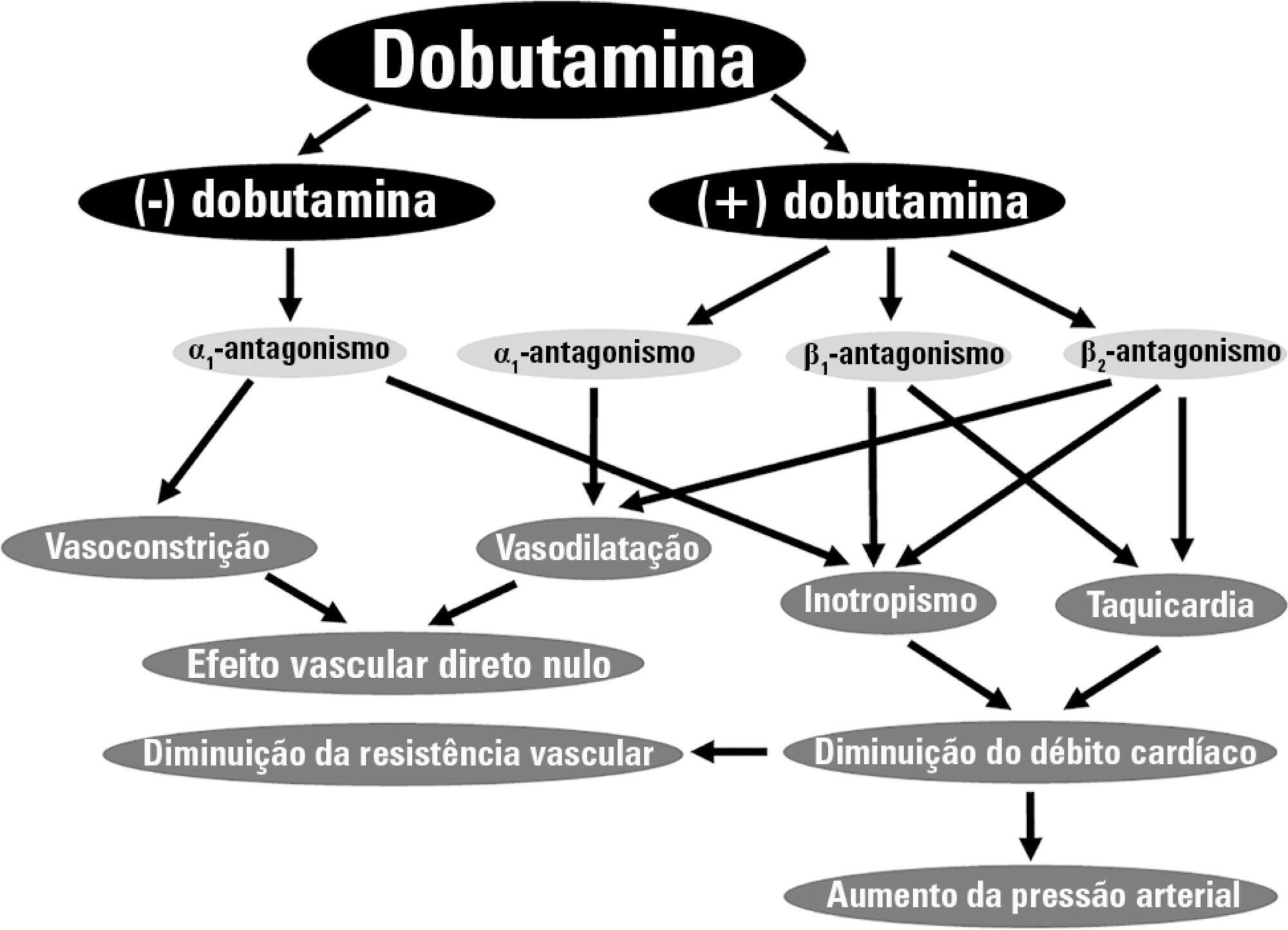
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):360-366
DOI 10.5935/0103-507X.20140055
In Brazil, there are no data on the preferences of intensivists regarding hemodynamic monitoring methods. The present study aimed to identify the methods used by national intensivists, the hemodynamic variables they consider important, the regional differences, the reasons for choosing a particular method, and the use of protocols and continued training.
National intensivists were invited to answer an electronic questionnaire during three intensive care events and later, through the Associação de Medicina Intensiva Brasileira portal, between March and October 2009. Demographic data and aspects related to the respondent preferences regarding hemodynamic monitoring were researched.
In total, 211 professionals answered the questionnaire. Private hospitals showed higher availability of resources for hemodynamic monitoring than did public institutions. The pulmonary artery catheter was considered the most trusted by 56.9% of the respondents, followed by echocardiograms, at 22.3%. Cardiac output was considered the most important variable. Other variables also considered relevant were mixed/central venous oxygen saturation, pulmonary artery occlusion pressure, and right ventricular end-diastolic volume. Echocardiography was the most used method (64.5%), followed by pulmonary artery catheter (49.3%). Only half of respondents used treatment protocols, and 25% worked in continuing education programs in hemodynamic monitoring.
Hemodynamic monitoring has a greater availability in intensive care units of private institutions in Brazil. Echocardiography was the most used monitoring method, but the pulmonary artery catheter remains the most reliable. The implementation of treatment protocols and continuing education programs in hemodynamic monitoring in Brazil is still insufficient.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):360-366
DOI 10.5935/0103-507X.20140055
In Brazil, there are no data on the preferences of intensivists regarding hemodynamic monitoring methods. The present study aimed to identify the methods used by national intensivists, the hemodynamic variables they consider important, the regional differences, the reasons for choosing a particular method, and the use of protocols and continued training.
National intensivists were invited to answer an electronic questionnaire during three intensive care events and later, through the Associação de Medicina Intensiva Brasileira portal, between March and October 2009. Demographic data and aspects related to the respondent preferences regarding hemodynamic monitoring were researched.
In total, 211 professionals answered the questionnaire. Private hospitals showed higher availability of resources for hemodynamic monitoring than did public institutions. The pulmonary artery catheter was considered the most trusted by 56.9% of the respondents, followed by echocardiograms, at 22.3%. Cardiac output was considered the most important variable. Other variables also considered relevant were mixed/central venous oxygen saturation, pulmonary artery occlusion pressure, and right ventricular end-diastolic volume. Echocardiography was the most used method (64.5%), followed by pulmonary artery catheter (49.3%). Only half of respondents used treatment protocols, and 25% worked in continuing education programs in hemodynamic monitoring.
Hemodynamic monitoring has a greater availability in intensive care units of private institutions in Brazil. Echocardiography was the most used monitoring method, but the pulmonary artery catheter remains the most reliable. The implementation of treatment protocols and continuing education programs in hemodynamic monitoring in Brazil is still insufficient.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)