
You searched for:"Sebastião Araújo"
We found (10) results for your search.-
Original Article
Atrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
Abstract
Original ArticleAtrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
Views0See moreABSTRACT
Objective:
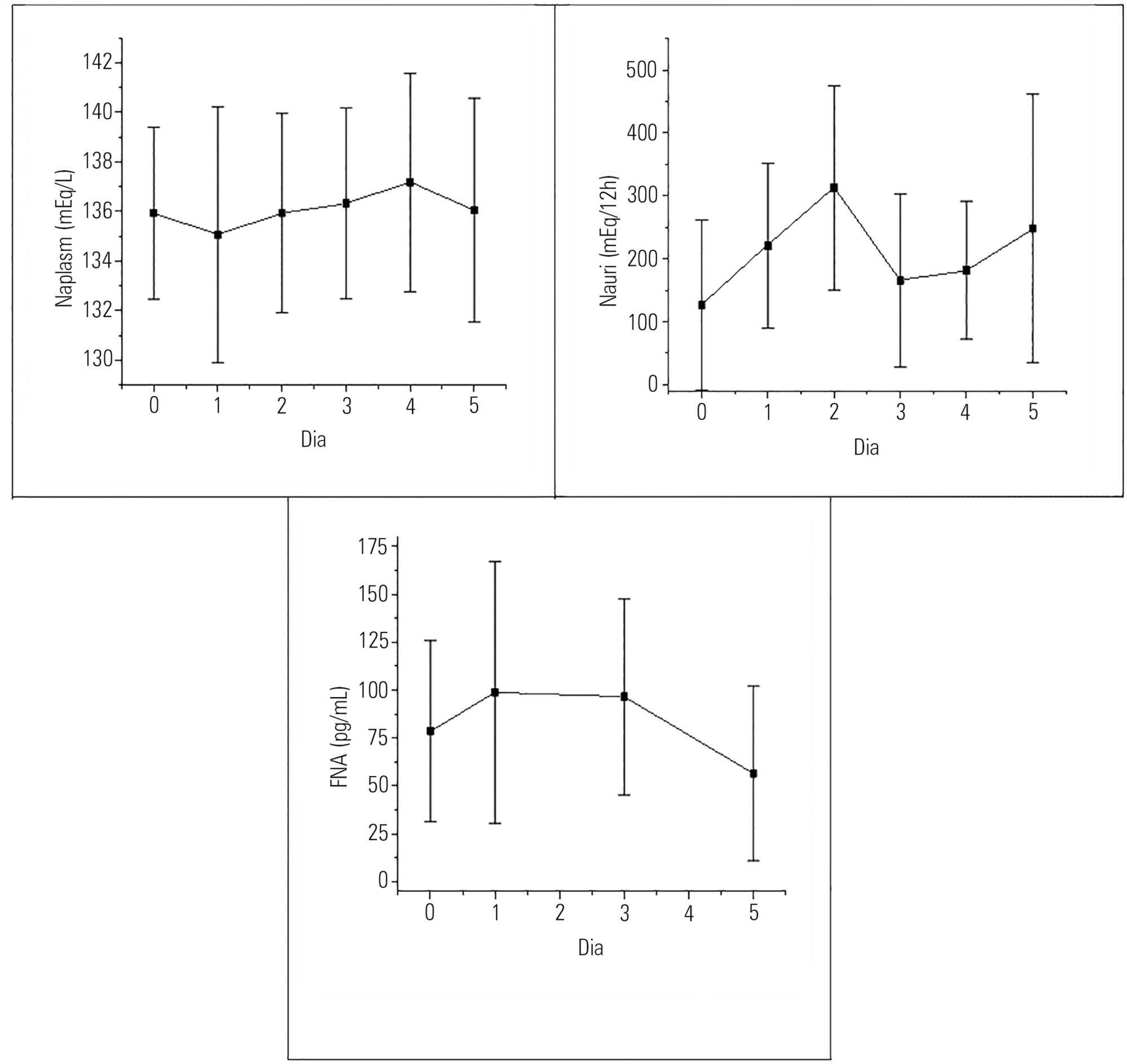
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
Methods:
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Results:
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Conclusion:
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
Views0

Abstract
Original ArticleAtrial natriuretic factor: is it responsible for hyponatremia and natriuresis in neurosurgery?
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
Views0See moreABSTRACT
Objective:
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
Methods:
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Results:
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Conclusion:
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
-
Original Articles
Profile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
Abstract
Original ArticlesProfile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
DOI 10.5935/0103-507X.20140004
Views0See moreObjective:
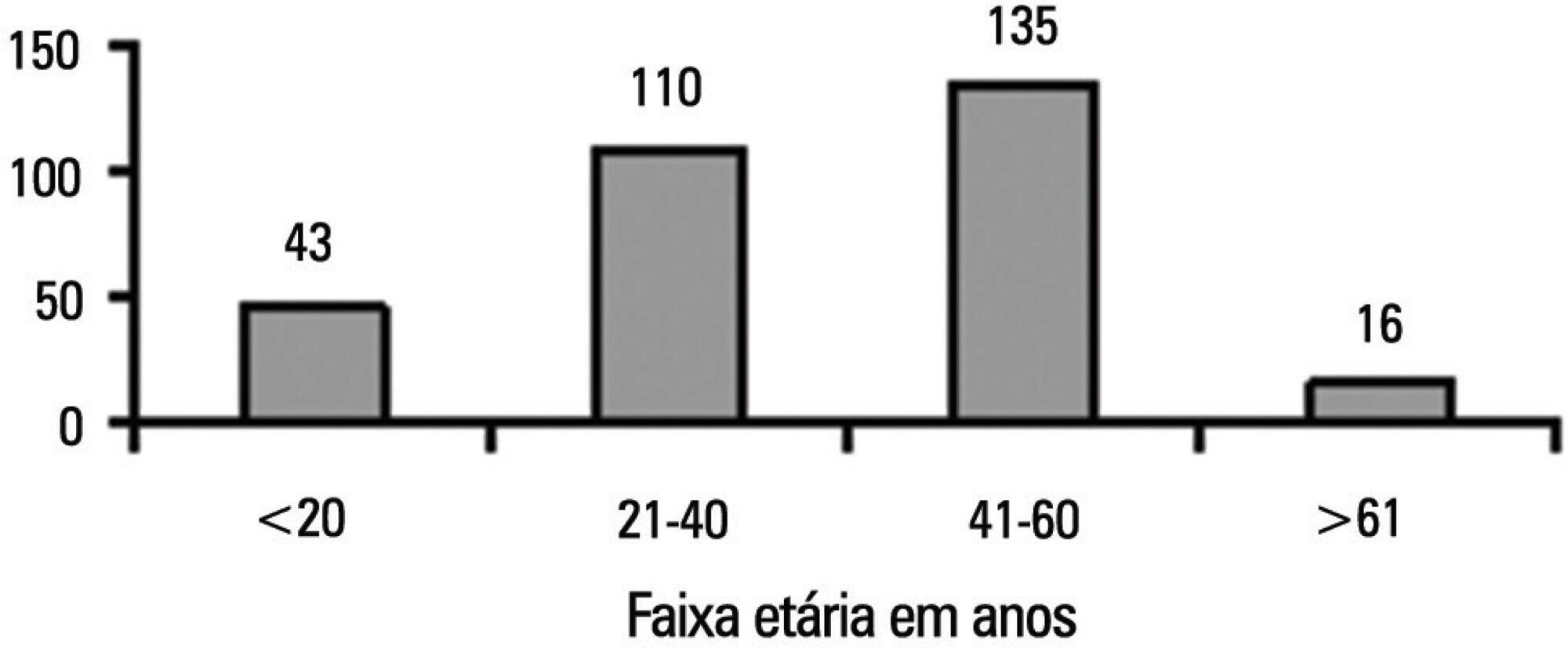
To characterize the profile of effective organ and tissue donors and to understand which organs and tissues were donated for transplantation.
Methods:
This was a quantitative, descriptive, exploratory, retrospective study that analyzed clinical data from 305 donors between January 2006 to December 2010. The data were then analyzed using descriptive analyses, generating frequency tables, measures of position (mean, minimum and maximum) and measures of dispersion (standard deviation) for data that was social and clinical in nature.
Results:
There was an overall predominance of white (72%) and male (55%) individuals between the ages of 41 and 60 years (44%). The primary cause of brain death was cerebrovascular accident (55%). In the patient history, 31% of the patients were classified as overweight, 27% as hypertensive and only 4.3% as having diabetes mellitus. Vasoactive drugs were used in 92.7% of the donors, and the main drug of choice was noradrenaline (81.6%). Hyperglycemia and hypernatremia were diagnosed in 78% and 71% of the donors, respectively.
Conclusion:
Significant hemodynamic changes were found, and the results indicate that the use of vasoactive drugs was the main strategy used to control these changes. Furthermore, most donors presented with hyperglycemia and hypernatremia, which were frequently reported in association with brain death. The persistent nature of these findings suggests that the organ donors were inadequately maintained.
Views0Abstract
Original ArticlesProfile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
DOI 10.5935/0103-507X.20140004
Views0See moreObjective:
To characterize the profile of effective organ and tissue donors and to understand which organs and tissues were donated for transplantation.
Methods:
This was a quantitative, descriptive, exploratory, retrospective study that analyzed clinical data from 305 donors between January 2006 to December 2010. The data were then analyzed using descriptive analyses, generating frequency tables, measures of position (mean, minimum and maximum) and measures of dispersion (standard deviation) for data that was social and clinical in nature.
Results:
There was an overall predominance of white (72%) and male (55%) individuals between the ages of 41 and 60 years (44%). The primary cause of brain death was cerebrovascular accident (55%). In the patient history, 31% of the patients were classified as overweight, 27% as hypertensive and only 4.3% as having diabetes mellitus. Vasoactive drugs were used in 92.7% of the donors, and the main drug of choice was noradrenaline (81.6%). Hyperglycemia and hypernatremia were diagnosed in 78% and 71% of the donors, respectively.
Conclusion:
Significant hemodynamic changes were found, and the results indicate that the use of vasoactive drugs was the main strategy used to control these changes. Furthermore, most donors presented with hyperglycemia and hypernatremia, which were frequently reported in association with brain death. The persistent nature of these findings suggests that the organ donors were inadequately maintained.
-
Lung injury and mechanical ventilation in cardiac surgery: a review
Rev Bras Ter Intensiva. 2010;22(4):375-383
Abstract
Lung injury and mechanical ventilation in cardiac surgery: a review
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Views0Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Keywords:AnoxiaCardiac surgical proceduresCardiopulmonary bypasslung injuryPostoperative periodRespiration, artificialRespiratory distress syndromeSee moreViews0Abstract
Lung injury and mechanical ventilation in cardiac surgery: a review
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Views0Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Keywords:AnoxiaCardiac surgical proceduresCardiopulmonary bypasslung injuryPostoperative periodRespiration, artificialRespiratory distress syndromeSee more -
Original Articles
Factors associated with increased mortality and prolonged length of stay in an adult intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):250-256
Abstract
Original ArticlesFactors associated with increased mortality and prolonged length of stay in an adult intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):250-256
DOI 10.1590/S0103-507X2010000300006
Views0See moreOBJECTIVE: The intensive care unit is synonymous of high severity, and its mortality rates are between 5.4 and 33%. With the development of new technologies, a patient can be maintained for long time in the unit, causing high costs, psychological and moral for all involved. This study aimed to evaluate the risk factors for mortality and prolonged length of stay in an adult intensive care unit. METHODS: The study included all patients consecutively admitted to the adult medical/surgical intensive care unit of Hospital das Clínicas da Universidade Estadual de Campinas, for six months. We collected data such as sex, age, diagnosis, personal history, APACHE II score, days of invasive mechanical ventilation orotracheal reintubation, tracheostomy, days of hospitalization in the intensive care unit and discharge or death in the intensive care unit. RESULTS: Were included in the study 401 patients; 59.6% men and 40.4% women, age 53.8±18.0. The mean intensive care unit stay was 8.2±10.8 days, with a mortality rate of 13.5%. Significant data for mortality and prolonged length of stay in intensive care unit (p <0.0001), were: APACHE II>11, OT-Re and tracheostomy. CONCLUSION: The mortality and prolonged length of stay in intensive care unit intensive care unit as risk factors were: APACHE>11, orotracheal reintubation and tracheostomy.
Views0Abstract
Original ArticlesFactors associated with increased mortality and prolonged length of stay in an adult intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):250-256
DOI 10.1590/S0103-507X2010000300006
Views0See moreOBJECTIVE: The intensive care unit is synonymous of high severity, and its mortality rates are between 5.4 and 33%. With the development of new technologies, a patient can be maintained for long time in the unit, causing high costs, psychological and moral for all involved. This study aimed to evaluate the risk factors for mortality and prolonged length of stay in an adult intensive care unit. METHODS: The study included all patients consecutively admitted to the adult medical/surgical intensive care unit of Hospital das Clínicas da Universidade Estadual de Campinas, for six months. We collected data such as sex, age, diagnosis, personal history, APACHE II score, days of invasive mechanical ventilation orotracheal reintubation, tracheostomy, days of hospitalization in the intensive care unit and discharge or death in the intensive care unit. RESULTS: Were included in the study 401 patients; 59.6% men and 40.4% women, age 53.8±18.0. The mean intensive care unit stay was 8.2±10.8 days, with a mortality rate of 13.5%. Significant data for mortality and prolonged length of stay in intensive care unit (p <0.0001), were: APACHE II>11, OT-Re and tracheostomy. CONCLUSION: The mortality and prolonged length of stay in intensive care unit intensive care unit as risk factors were: APACHE>11, orotracheal reintubation and tracheostomy.
-
Consenso Brasileiro de Monitorização e Suporte Hemodinâmico
Part II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoPart II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
Views1See moreBACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Views1Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoPart II: basic hemodynamic monitoring and the use of pulmonary artery catheter
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
Views1See moreBACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
-
Consenso Brasileiro de Monitorização e Suporte Hemodinâmico
Brazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoBrazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
Views1See moreBACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the ” gold standard” to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Views1Abstract
Consenso Brasileiro de Monitorização e Suporte HemodinâmicoBrazilian consensus of monitoring and hemodynamic support – part III: alternative methods for cardiac output monitoring and volemia estimation
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
Views1See moreBACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the ” gold standard” to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
-
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
Abstract
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
Views0BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients’ level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Keywords:consciousness disturbancesmaximum inspiratory pressuremechanical ventilationunidirectional valveWeaningSee moreViews0Abstract
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
Views0BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients’ level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Keywords:consciousness disturbancesmaximum inspiratory pressuremechanical ventilationunidirectional valveWeaningSee more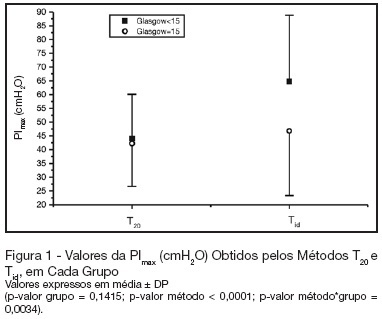
-
Cuff leak test preextubation: comparison between three methods in spontaneous ventilation
Rev Bras Ter Intensiva. 2007;19(3):310-316
Abstract
Cuff leak test preextubation: comparison between three methods in spontaneous ventilation
Rev Bras Ter Intensiva. 2007;19(3):310-316
DOI 10.1590/S0103-507X2007000300007
Views0BACKGROUND AND OBJECTIVES: The cuff leak test aims to evaluate the presence of airway obstruction and normally is carried through in the controlled mode of mechanical ventilation. The objective of this study was to evaluate the cuff leak in patients breathing spontaneously, across three different methods, and to compare them. METHODS: Twenty intubated patients had been submitted to three different forms of cuff leak test, all of them in spontaneous respiration: measuring air leak buy using a ventilometer and with the patient connected to the mechanical ventilator (test 1); through the display of the mechanical ventilator (test 2); and with ventilometer and the patient detached from the mechanical ventilator (test 3). The air leak around the tracheal tube (TT) was defined as the percentage difference between the inspired tidal volume (insufflated cuff) and exhaled (deflated cuff). The air leak differences between the three tests were evaluated, as well as their correlations to three variables: cuff pressure, TT diameter and intubation time. RESULTS: Statistically significant (p < 0.05) air leak difference was observed between the tests 1 and 2 in relation to the test 3 in the general and regarding time intubation below 48h and cuff pressure below 20 cmH2O. Regarding the tube diameter, it had been difference only between tests 2 and 3 for 8.5 mm tubes. CONCLUSIONS: The cuff leak test in spontaneous ventilation seems to be more accurate when the patient is connected to the mechanical ventilator, and that additional studies are needed to determine the real contribution of the test in this ventilation mode to predict laryngeal edema.
Keywords:artificial ventilationcuff leak testlaryngeal edematracheal intubationventilatory function testsSee moreViews0Abstract
Cuff leak test preextubation: comparison between three methods in spontaneous ventilation
Rev Bras Ter Intensiva. 2007;19(3):310-316
DOI 10.1590/S0103-507X2007000300007
Views0BACKGROUND AND OBJECTIVES: The cuff leak test aims to evaluate the presence of airway obstruction and normally is carried through in the controlled mode of mechanical ventilation. The objective of this study was to evaluate the cuff leak in patients breathing spontaneously, across three different methods, and to compare them. METHODS: Twenty intubated patients had been submitted to three different forms of cuff leak test, all of them in spontaneous respiration: measuring air leak buy using a ventilometer and with the patient connected to the mechanical ventilator (test 1); through the display of the mechanical ventilator (test 2); and with ventilometer and the patient detached from the mechanical ventilator (test 3). The air leak around the tracheal tube (TT) was defined as the percentage difference between the inspired tidal volume (insufflated cuff) and exhaled (deflated cuff). The air leak differences between the three tests were evaluated, as well as their correlations to three variables: cuff pressure, TT diameter and intubation time. RESULTS: Statistically significant (p < 0.05) air leak difference was observed between the tests 1 and 2 in relation to the test 3 in the general and regarding time intubation below 48h and cuff pressure below 20 cmH2O. Regarding the tube diameter, it had been difference only between tests 2 and 3 for 8.5 mm tubes. CONCLUSIONS: The cuff leak test in spontaneous ventilation seems to be more accurate when the patient is connected to the mechanical ventilator, and that additional studies are needed to determine the real contribution of the test in this ventilation mode to predict laryngeal edema.
Keywords:artificial ventilationcuff leak testlaryngeal edematracheal intubationventilatory function testsSee more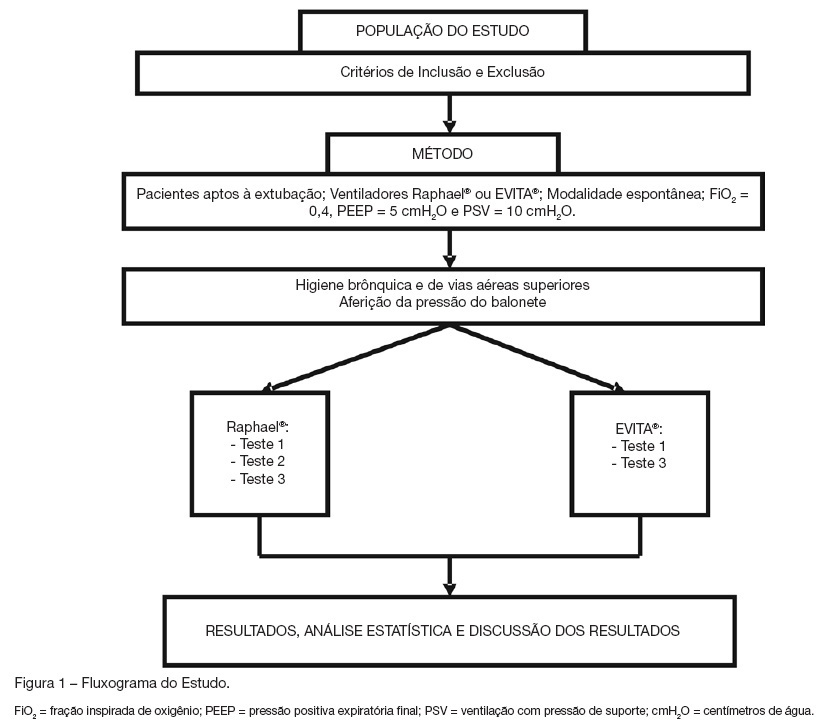
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis