tracheal intubation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva.2008;20(1):77-81
DOI 10.1590/S0103-507X2008000100012
BACKGROUND AND OBJECTIVES: Weaning patients from mechanical ventilation is a challenge in the intensive care unit (ICU) practice and is related to some complications. One of these is the pos-extubation laryngospasm, an event that can be anticipated for the cuff leak test (CLT). The objective was demonstrate that the CLT is a simple, reliable and low costs method to available the presence of obstruction in high airway in patients under weaning ventilator. CONTENTS: It was made a systematic review in databases MedLine, SciElo and LILACS with articles from 1995 to 2007. The selected studies focused the use of the CLT to predict laryngospasm and extubation failure. It was excluded studies with animals and others literature reviews. It was looked correlates the CLT with mechanical ventilation's days, age and specific groups that could beneficiates with the application of this technique. CONCLUSIONS: The CLT can be considerate a good index to predict laryngospasm pos-extubation, when considerate the studied population characteristics.
Abstract
Rev Bras Ter Intensiva.2008;20(1):77-81
DOI 10.1590/S0103-507X2008000100012
BACKGROUND AND OBJECTIVES: Weaning patients from mechanical ventilation is a challenge in the intensive care unit (ICU) practice and is related to some complications. One of these is the pos-extubation laryngospasm, an event that can be anticipated for the cuff leak test (CLT). The objective was demonstrate that the CLT is a simple, reliable and low costs method to available the presence of obstruction in high airway in patients under weaning ventilator. CONTENTS: It was made a systematic review in databases MedLine, SciElo and LILACS with articles from 1995 to 2007. The selected studies focused the use of the CLT to predict laryngospasm and extubation failure. It was excluded studies with animals and others literature reviews. It was looked correlates the CLT with mechanical ventilation's days, age and specific groups that could beneficiates with the application of this technique. CONCLUSIONS: The CLT can be considerate a good index to predict laryngospasm pos-extubation, when considerate the studied population characteristics.
Abstract
Rev Bras Ter Intensiva.2007;19(3):310-316
DOI 10.1590/S0103-507X2007000300007
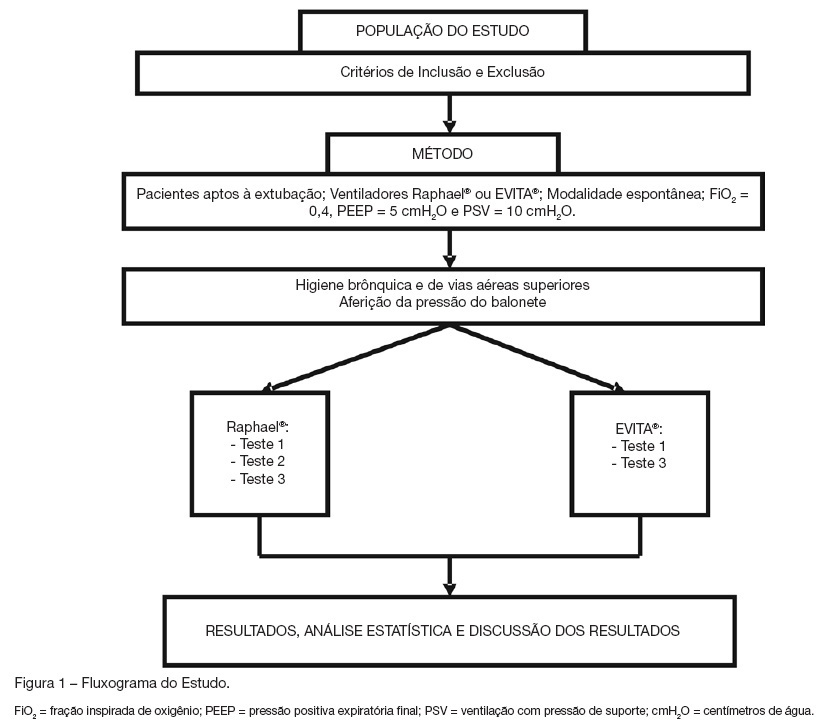
BACKGROUND AND OBJECTIVES: The cuff leak test aims to evaluate the presence of airway obstruction and normally is carried through in the controlled mode of mechanical ventilation. The objective of this study was to evaluate the cuff leak in patients breathing spontaneously, across three different methods, and to compare them. METHODS: Twenty intubated patients had been submitted to three different forms of cuff leak test, all of them in spontaneous respiration: measuring air leak buy using a ventilometer and with the patient connected to the mechanical ventilator (test 1); through the display of the mechanical ventilator (test 2); and with ventilometer and the patient detached from the mechanical ventilator (test 3). The air leak around the tracheal tube (TT) was defined as the percentage difference between the inspired tidal volume (insufflated cuff) and exhaled (deflated cuff). The air leak differences between the three tests were evaluated, as well as their correlations to three variables: cuff pressure, TT diameter and intubation time. RESULTS: Statistically significant (p < 0.05) air leak difference was observed between the tests 1 and 2 in relation to the test 3 in the general and regarding time intubation below 48h and cuff pressure below 20 cmH2O. Regarding the tube diameter, it had been difference only between tests 2 and 3 for 8.5 mm tubes. CONCLUSIONS: The cuff leak test in spontaneous ventilation seems to be more accurate when the patient is connected to the mechanical ventilator, and that additional studies are needed to determine the real contribution of the test in this ventilation mode to predict laryngeal edema.
Abstract
Rev Bras Ter Intensiva.2007;19(3):310-316
DOI 10.1590/S0103-507X2007000300007
BACKGROUND AND OBJECTIVES: The cuff leak test aims to evaluate the presence of airway obstruction and normally is carried through in the controlled mode of mechanical ventilation. The objective of this study was to evaluate the cuff leak in patients breathing spontaneously, across three different methods, and to compare them. METHODS: Twenty intubated patients had been submitted to three different forms of cuff leak test, all of them in spontaneous respiration: measuring air leak buy using a ventilometer and with the patient connected to the mechanical ventilator (test 1); through the display of the mechanical ventilator (test 2); and with ventilometer and the patient detached from the mechanical ventilator (test 3). The air leak around the tracheal tube (TT) was defined as the percentage difference between the inspired tidal volume (insufflated cuff) and exhaled (deflated cuff). The air leak differences between the three tests were evaluated, as well as their correlations to three variables: cuff pressure, TT diameter and intubation time. RESULTS: Statistically significant (p < 0.05) air leak difference was observed between the tests 1 and 2 in relation to the test 3 in the general and regarding time intubation below 48h and cuff pressure below 20 cmH2O. Regarding the tube diameter, it had been difference only between tests 2 and 3 for 8.5 mm tubes. CONCLUSIONS: The cuff leak test in spontaneous ventilation seems to be more accurate when the patient is connected to the mechanical ventilator, and that additional studies are needed to determine the real contribution of the test in this ventilation mode to predict laryngeal edema.
Abstract
Rev Bras Ter Intensiva.2007;19(1):118-122
DOI 10.1590/S0103-507X2007000100016
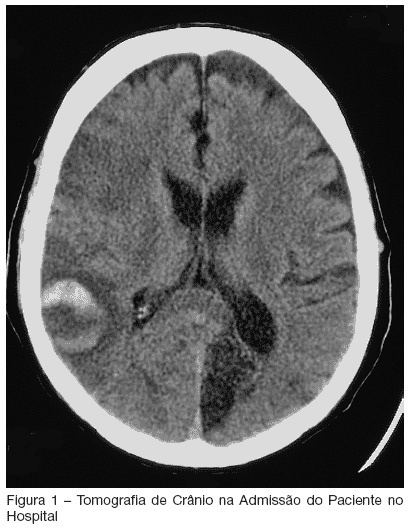
BACKGROUND AND OBJECTIVES: Critically ill patients represent a population with multiple risk factors for aspiration. Features such as decreased level of consciousness, mechanical ventilation, and comorbities as stroke, correlate with this increased threat in intensive care unit (ICU) patients. Recognition of deglutition dysfunction may identify patients at high risk of aspiration, and thereby help to avoid pulmonary complications such as recurrent pneumonia. The goal of our report is show a severe case of recurrent aspirative pneumonia after acute stroke and intubation, alerting to appropriate diagnosis and treatment of this condition. CASE REPORT: A male patient, 57 year old, was admitted to the hospital because of acute stroke. Ten days later, the patient began to have fever and severe shortness of breath. He was admitted to the ICU necessitating of intratracheal intubation. Four days after intubation he was extubated, however, he had a new aspirative pneumonia in ICU, newly treated. An evaluation of swallowing demonstrated a severe deglutition dysfunction with a high risk of aspiration. The patient was transferred, but aspirative pneumonia was diagnosed eight days after his ICU discharge and he was readmitted, stayed for a long time in ICU and presenting severe morbidity. CONCLUSIONS: ICU patients who are at risk for swallowing dysfunction and aspiration should be identified to prevent their associated morbidity and mortality.
Abstract
Rev Bras Ter Intensiva.2007;19(1):118-122
DOI 10.1590/S0103-507X2007000100016
BACKGROUND AND OBJECTIVES: Critically ill patients represent a population with multiple risk factors for aspiration. Features such as decreased level of consciousness, mechanical ventilation, and comorbities as stroke, correlate with this increased threat in intensive care unit (ICU) patients. Recognition of deglutition dysfunction may identify patients at high risk of aspiration, and thereby help to avoid pulmonary complications such as recurrent pneumonia. The goal of our report is show a severe case of recurrent aspirative pneumonia after acute stroke and intubation, alerting to appropriate diagnosis and treatment of this condition. CASE REPORT: A male patient, 57 year old, was admitted to the hospital because of acute stroke. Ten days later, the patient began to have fever and severe shortness of breath. He was admitted to the ICU necessitating of intratracheal intubation. Four days after intubation he was extubated, however, he had a new aspirative pneumonia in ICU, newly treated. An evaluation of swallowing demonstrated a severe deglutition dysfunction with a high risk of aspiration. The patient was transferred, but aspirative pneumonia was diagnosed eight days after his ICU discharge and he was readmitted, stayed for a long time in ICU and presenting severe morbidity. CONCLUSIONS: ICU patients who are at risk for swallowing dysfunction and aspiration should be identified to prevent their associated morbidity and mortality.