lung injury Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(2):212-219
DOI 10.5935/0103-507X.20220018-en
To analyze the influence of mechanical power and its components on mechanical ventilation for patients infected with SARS-CoV-2; identify the values of the mechanical ventilation components and verify their correlations with each other and with the mechanical power and effects on the result of the Gattinoni-S and Giosa formulas.
This was an observational, longitudinal, analytical and quantitative study of respirator and mechanical power parameters in patients with SARS-CoV-2.
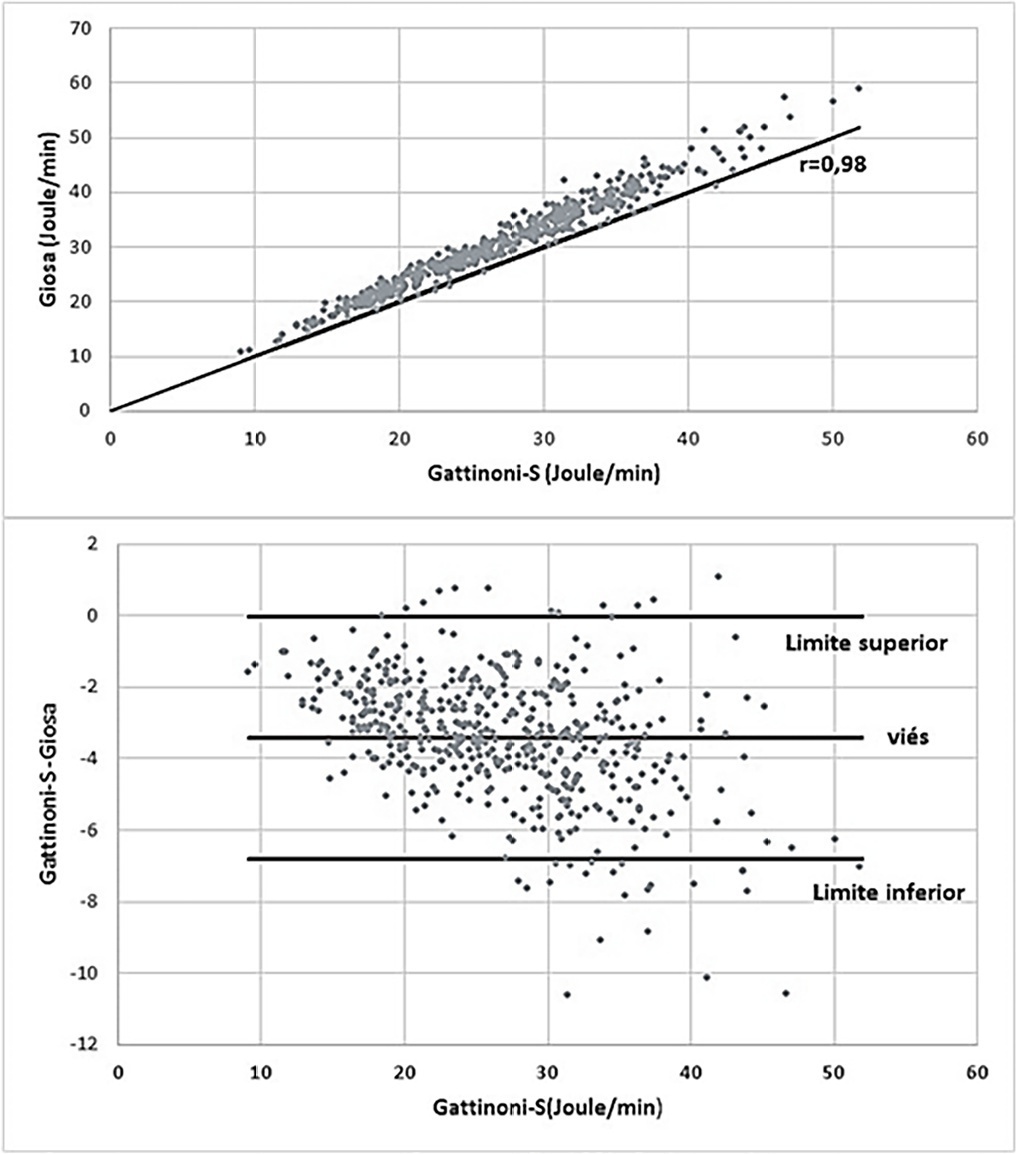
The mean mechanical power was 26.9J/minute (Gattinoni-S) and 30.3 J/minute (Giosa). The driving pressure was 14.4cmH2O, the plateau pressure was 26.5cmH2O, the positive end-expiratory pressure was 12.1cmH2O, the elastance was 40.6cmH2O/L, the tidal volume was 0.36L, and the respiratory rate was 32 breaths/minute. The correlation between the Gattinoni and Giosa formulas was 0.98, with a bias of -3.4J/minute and a difference in the correlation of the resistance pressure of 0.39 (Gattinoni) and 0.24 (Giosa). Among the components, the correlations between elastance and driving pressure (0.88), positive end-expiratory pressure (-0.54) and tidal volume (-0.44) stood out.
In the analysis of mechanical ventilation for patients with SARS-CoV-2, it was found that the correlations of its components with mechanical power influenced its high momentary values and and that the correlations of its components with each other influenced their behavior throughout the study period. Because they have specific effects on the Gatinnoni-S and Giosa formulas, the mechanical ventilation components influenced their calculations and caused divergence in the mechanical power values.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):212-219
DOI 10.5935/0103-507X.20220018-en
To analyze the influence of mechanical power and its components on mechanical ventilation for patients infected with SARS-CoV-2; identify the values of the mechanical ventilation components and verify their correlations with each other and with the mechanical power and effects on the result of the Gattinoni-S and Giosa formulas.
This was an observational, longitudinal, analytical and quantitative study of respirator and mechanical power parameters in patients with SARS-CoV-2.
The mean mechanical power was 26.9J/minute (Gattinoni-S) and 30.3 J/minute (Giosa). The driving pressure was 14.4cmH2O, the plateau pressure was 26.5cmH2O, the positive end-expiratory pressure was 12.1cmH2O, the elastance was 40.6cmH2O/L, the tidal volume was 0.36L, and the respiratory rate was 32 breaths/minute. The correlation between the Gattinoni and Giosa formulas was 0.98, with a bias of -3.4J/minute and a difference in the correlation of the resistance pressure of 0.39 (Gattinoni) and 0.24 (Giosa). Among the components, the correlations between elastance and driving pressure (0.88), positive end-expiratory pressure (-0.54) and tidal volume (-0.44) stood out.
In the analysis of mechanical ventilation for patients with SARS-CoV-2, it was found that the correlations of its components with mechanical power influenced its high momentary values and and that the correlations of its components with each other influenced their behavior throughout the study period. Because they have specific effects on the Gatinnoni-S and Giosa formulas, the mechanical ventilation components influenced their calculations and caused divergence in the mechanical power values.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):373-379
DOI 10.5935/0103-507X.20160067
To determine the effect of feedback and education regarding the use of predicted body weight to adjust tidal volume in a lung-protective mechanical ventilation strategy.
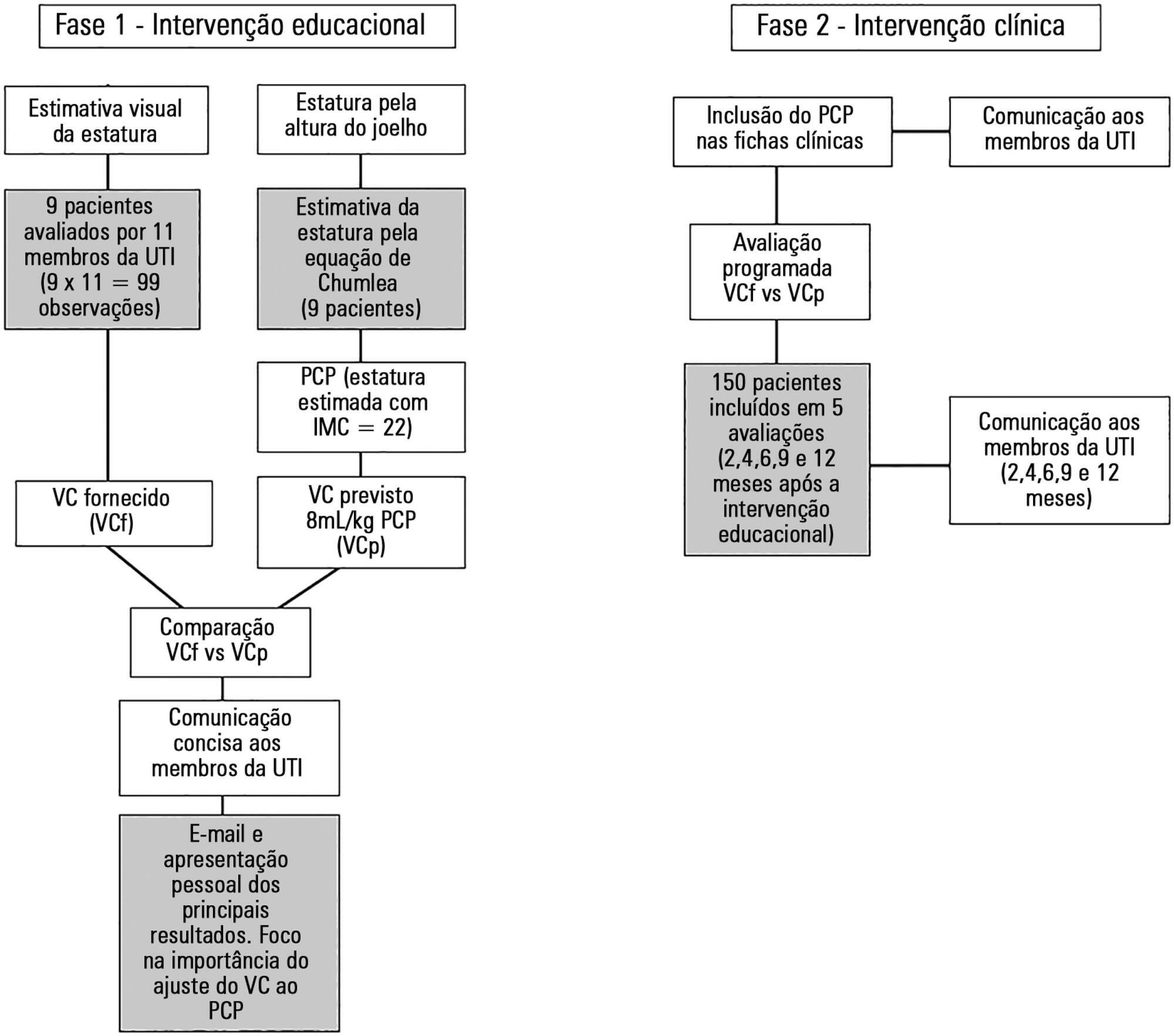
The study was performed from October 2014 to November 2015 (12 months) in a single university polyvalent intensive care unit. We developed a combined intervention (education and feedback), placing particular attention on the importance of adjusting tidal volumes to predicted body weight bedside. In parallel, predicted body weight was estimated from knee height and included in clinical charts.
One hundred fifty-nine patients were included. Predicted body weight assessed by knee height instead of visual evaluation revealed that the delivered tidal volume was significantly higher than predicted. After the inclusion of predicted body weight, we observed a sustained reduction in delivered tidal volume from a mean (standard error) of 8.97 ± 0.32 to 7.49 ± 0.19mL/kg (p < 0.002). Furthermore, the protocol adherence was subsequently sustained for 12 months (delivered tidal volume 7.49 ± 0.54 versus 7.62 ± 0.20mL/kg; p = 0.103).
The lack of a reliable method to estimate the predicted body weight is a significant impairment for the application of a worldwide standard of care during mechanical ventilation. A combined intervention based on education and repeated feedbacks promoted sustained tidal volume education during the study period (12 months).
Abstract
Rev Bras Ter Intensiva. 2016;28(4):373-379
DOI 10.5935/0103-507X.20160067
To determine the effect of feedback and education regarding the use of predicted body weight to adjust tidal volume in a lung-protective mechanical ventilation strategy.
The study was performed from October 2014 to November 2015 (12 months) in a single university polyvalent intensive care unit. We developed a combined intervention (education and feedback), placing particular attention on the importance of adjusting tidal volumes to predicted body weight bedside. In parallel, predicted body weight was estimated from knee height and included in clinical charts.
One hundred fifty-nine patients were included. Predicted body weight assessed by knee height instead of visual evaluation revealed that the delivered tidal volume was significantly higher than predicted. After the inclusion of predicted body weight, we observed a sustained reduction in delivered tidal volume from a mean (standard error) of 8.97 ± 0.32 to 7.49 ± 0.19mL/kg (p < 0.002). Furthermore, the protocol adherence was subsequently sustained for 12 months (delivered tidal volume 7.49 ± 0.54 versus 7.62 ± 0.20mL/kg; p = 0.103).
The lack of a reliable method to estimate the predicted body weight is a significant impairment for the application of a worldwide standard of care during mechanical ventilation. A combined intervention based on education and repeated feedbacks promoted sustained tidal volume education during the study period (12 months).
Abstract
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):416-424
DOI 10.1590/S0103-507X2009000400012
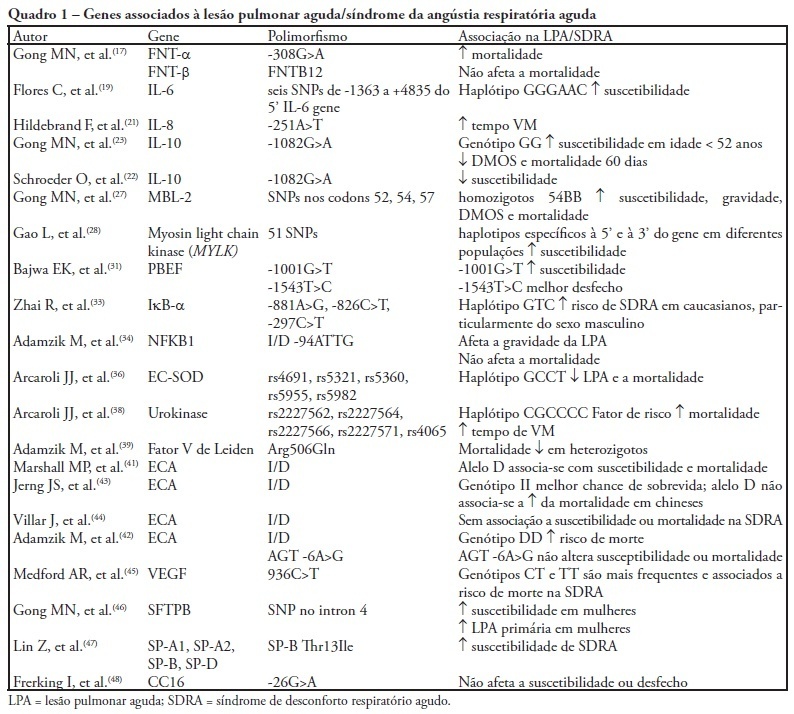
Acute lung injury and its most severe presentation, acute respiratory distress syndrome, are a common denominator for several diseases which can lead to exaggerated lung inflammation. In the last years this variability has been ascribed, at least partially, to genetic issues. This study aims to review the role of the main genes involved in acute lung injury and acute respiratory distress syndrome susceptibility, morbidity and mortality. By search on PubMed and LiLACS databases, using the key words acute lung injury, acute respiratory distress syndrome and adult acute respiratory distress syndrome in combination with genetic polymorphisms, 69 papers were selected, from which 38 were included in this review. Were also considered relevant articles extracted from the reference lists in the articles selected from the databases. Genetic polymorphisms are gene variations in at least 1% population. These gene variations may influence the inflammatory response mediators' expression, directly affecting the susceptibility to acute lung injury, the intensity of lung parenchyma inflammation, the development clinical course and outcome. Association studies reproducible in large populations will definitely allow genomics to be included into the diagnostic and therapeutic armamentarium for acute lung injury/acute respiratory distress syndrome patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):416-424
DOI 10.1590/S0103-507X2009000400012
Acute lung injury and its most severe presentation, acute respiratory distress syndrome, are a common denominator for several diseases which can lead to exaggerated lung inflammation. In the last years this variability has been ascribed, at least partially, to genetic issues. This study aims to review the role of the main genes involved in acute lung injury and acute respiratory distress syndrome susceptibility, morbidity and mortality. By search on PubMed and LiLACS databases, using the key words acute lung injury, acute respiratory distress syndrome and adult acute respiratory distress syndrome in combination with genetic polymorphisms, 69 papers were selected, from which 38 were included in this review. Were also considered relevant articles extracted from the reference lists in the articles selected from the databases. Genetic polymorphisms are gene variations in at least 1% population. These gene variations may influence the inflammatory response mediators' expression, directly affecting the susceptibility to acute lung injury, the intensity of lung parenchyma inflammation, the development clinical course and outcome. Association studies reproducible in large populations will definitely allow genomics to be included into the diagnostic and therapeutic armamentarium for acute lung injury/acute respiratory distress syndrome patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):103-105
DOI 10.1590/S0103-507X2008000100017
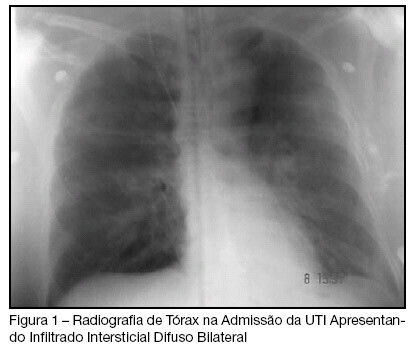
BACKGROUND AND OBJECTIVES: The Transfusion-Related Acute Lung Injury (TRALI), is defined as noncardiogenic pulmonary edema temporally related to transfusion therapy, evolving with ventilation necessity mechanics in the great majority of the cases. This objective of this study was to present case of TRALI in the immediate postoperative of neurosurgery. CASE REPORT: We describe the case of a patient who presented broncoespasm and decreased oxygen saturation after to have received fresh-frozen plasma in the neurosurgery, who presented TRALI. The patient was submitted a invasive hemodynamic monitoring, sedation and supplemental oxygen with mechanical ventilation, with gradual improvement, leaving the intensive care unit in the eight day of postoperative. CONCLUSIONS: The TRALI must be investigated in the patients who receive transfusion therapy and present lung injury.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):103-105
DOI 10.1590/S0103-507X2008000100017
BACKGROUND AND OBJECTIVES: The Transfusion-Related Acute Lung Injury (TRALI), is defined as noncardiogenic pulmonary edema temporally related to transfusion therapy, evolving with ventilation necessity mechanics in the great majority of the cases. This objective of this study was to present case of TRALI in the immediate postoperative of neurosurgery. CASE REPORT: We describe the case of a patient who presented broncoespasm and decreased oxygen saturation after to have received fresh-frozen plasma in the neurosurgery, who presented TRALI. The patient was submitted a invasive hemodynamic monitoring, sedation and supplemental oxygen with mechanical ventilation, with gradual improvement, leaving the intensive care unit in the eight day of postoperative. CONCLUSIONS: The TRALI must be investigated in the patients who receive transfusion therapy and present lung injury.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)