Cardiac surgical procedures Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(3):361-367
DOI 10.5935/0103-507X.20190059
To compare the impact of two fast-track strategies regarding the extubation time and removal of invasive mechanical ventilation in adults after cardiac surgery on clinical and hospital outcomes.
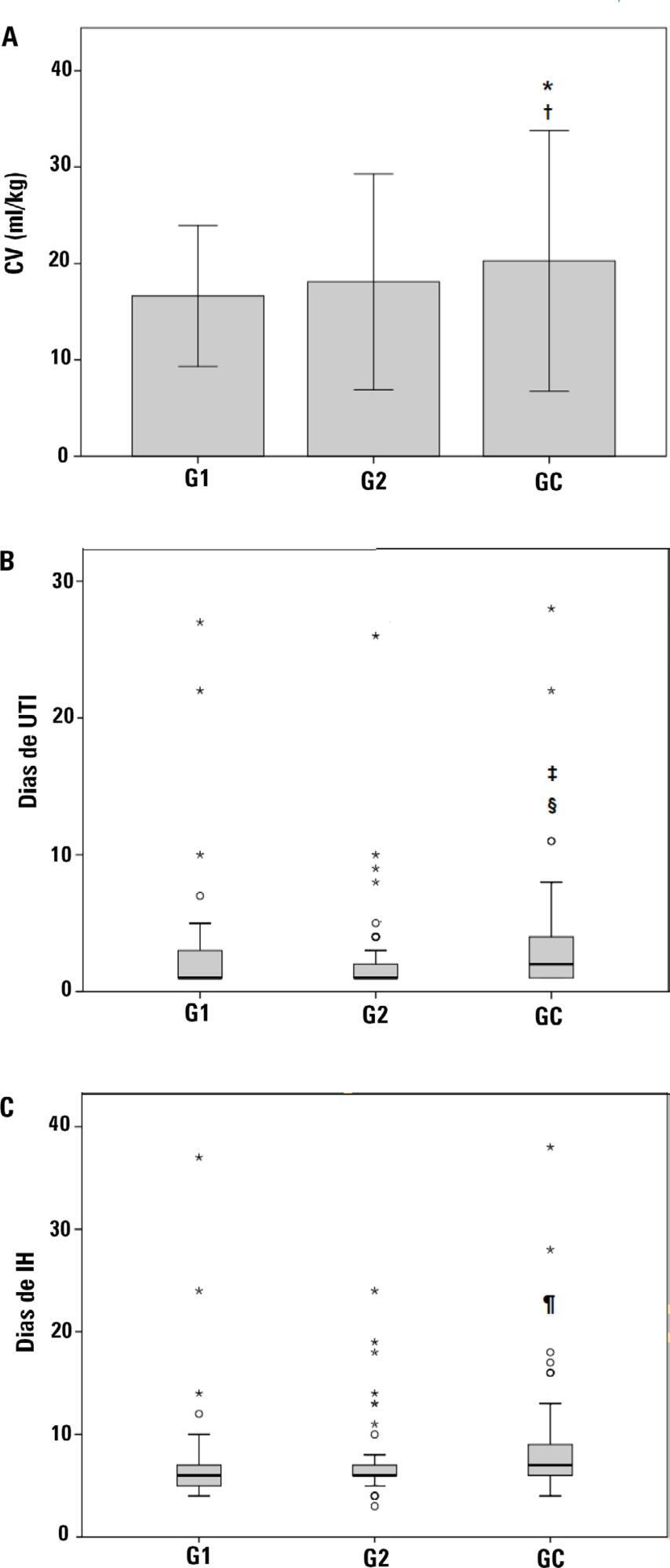
This was a retrospective cohort study with patients undergoing cardiac surgery. Patients were classified according to the extubation time as the Control Group (extubated 6 hours after admission to the intensive care unit, with a maximum mechanical ventilation time of 18 hours), Group 1 (extubated in the operating room after surgery) and Group 2 (extubated within 6 hours after admission to the intensive care unit). The primary outcomes analyzed were vital capacity on the first postoperative day, length of hospital stay, and length of stay in the intensive care unit. The secondary outcomes were reintubation, hospital-acquired pneumonia, sepsis, and death.
For the 223 patients evaluated, the vital capacity was lower in Groups 1 and 2 compared to the Control (p = 0.000 and p = 0.046, respectively). The length of stay in the intensive care unit was significantly lower in Groups 1 and 2 compared to the Control (p = 0.009 and p = 0.000, respectively), whereas the length of hospital stay was lower in Group 1 compared to the Control (p = 0.014). There was an association between extubation in the operating room (Group 1) with reintubation (p = 0.025) and postoperative complications (p = 0.038).
Patients undergoing fast-track management with extubation within 6 hours had shorter stays in the intensive care unit without increasing postoperative complications and death. Patients extubated in the operating room had a shorter hospital stay and a shorter stay in the intensive care unit but showed an increase in the frequency of reintubation and postoperative complications.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):361-367
DOI 10.5935/0103-507X.20190059
To compare the impact of two fast-track strategies regarding the extubation time and removal of invasive mechanical ventilation in adults after cardiac surgery on clinical and hospital outcomes.
This was a retrospective cohort study with patients undergoing cardiac surgery. Patients were classified according to the extubation time as the Control Group (extubated 6 hours after admission to the intensive care unit, with a maximum mechanical ventilation time of 18 hours), Group 1 (extubated in the operating room after surgery) and Group 2 (extubated within 6 hours after admission to the intensive care unit). The primary outcomes analyzed were vital capacity on the first postoperative day, length of hospital stay, and length of stay in the intensive care unit. The secondary outcomes were reintubation, hospital-acquired pneumonia, sepsis, and death.
For the 223 patients evaluated, the vital capacity was lower in Groups 1 and 2 compared to the Control (p = 0.000 and p = 0.046, respectively). The length of stay in the intensive care unit was significantly lower in Groups 1 and 2 compared to the Control (p = 0.009 and p = 0.000, respectively), whereas the length of hospital stay was lower in Group 1 compared to the Control (p = 0.014). There was an association between extubation in the operating room (Group 1) with reintubation (p = 0.025) and postoperative complications (p = 0.038).
Patients undergoing fast-track management with extubation within 6 hours had shorter stays in the intensive care unit without increasing postoperative complications and death. Patients extubated in the operating room had a shorter hospital stay and a shorter stay in the intensive care unit but showed an increase in the frequency of reintubation and postoperative complications.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald's statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population's attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald's statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population's attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):375-383
DOI 10.1590/S0103-507X2010000400011
Respiratory failure after cardiopulmonary bypass heart surgery can result from many pre-, intra- or postoperative respiratory system-related factors. This review was aimed to discuss some factors related to acute lung injury observed during the postoperative period of cardiac surgery and the mechanical ventilation modalities which should be considered to prevent hypoxemia.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)