Postoperative complications Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(1):57-62
DOI 10.5935/0103-507X.20190016
To assess the Perme mobility scale score as a predictor of functional status and complications in the postoperative period in patients undergoing liver transplantation.
The sample consisted of 30 patients who underwent liver transplantation. The patients were evaluated at two time points to determine their perception of pain, degree of dyspnea, peripheral muscle strength, and functional status according to the Perme scale. The collected data were analyzed by descriptive and inferential statistics. To compare the means between the evaluations, Student's t test for paired samples was applied. In case of asymmetry, the Wilcoxon test was used. In the evaluation of the association between the quantitative variables, the Pearson or Spearman correlation tests were applied.
A total of 30 individuals who underwent liver transplantation were included. The patients were predominantly male, and the mean age was 58.4 ± 9.9 years. The most prevalent underlying pathology was cirrhosis C virus (23.3%). Significant associations of the time on mechanical ventilation with the Perme scale score at discharge from the intensive care unit (r = -0.374; p = 0.042) and the number of physical therapy treatments (r = -0.578; p = 0.001) were recorded. When comparing the results of the initial evaluation and the evaluation at hospital discharge, there was a significant improvement in functional status (p < 0.001).
Functional mobility, peripheral muscle strength, pain perception, and dyspnea are significantly improved at hospital discharge compared with those at inpatient unit admission.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):57-62
DOI 10.5935/0103-507X.20190016
To assess the Perme mobility scale score as a predictor of functional status and complications in the postoperative period in patients undergoing liver transplantation.
The sample consisted of 30 patients who underwent liver transplantation. The patients were evaluated at two time points to determine their perception of pain, degree of dyspnea, peripheral muscle strength, and functional status according to the Perme scale. The collected data were analyzed by descriptive and inferential statistics. To compare the means between the evaluations, Student's t test for paired samples was applied. In case of asymmetry, the Wilcoxon test was used. In the evaluation of the association between the quantitative variables, the Pearson or Spearman correlation tests were applied.
A total of 30 individuals who underwent liver transplantation were included. The patients were predominantly male, and the mean age was 58.4 ± 9.9 years. The most prevalent underlying pathology was cirrhosis C virus (23.3%). Significant associations of the time on mechanical ventilation with the Perme scale score at discharge from the intensive care unit (r = -0.374; p = 0.042) and the number of physical therapy treatments (r = -0.578; p = 0.001) were recorded. When comparing the results of the initial evaluation and the evaluation at hospital discharge, there was a significant improvement in functional status (p < 0.001).
Functional mobility, peripheral muscle strength, pain perception, and dyspnea are significantly improved at hospital discharge compared with those at inpatient unit admission.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):233-238
DOI 10.5935/0103-507X.20130040
The objective of this study was to assess the correlation between the European System for Cardiac Operative Risk Evaluation (EuroSCORE) score and the risk of developing acute kidney injury in cardiac surgery patients.
This retrospective study was conducted at a tertiary hospital on consecutive cardiac surgery patients (e.g., valvular, ischemic and congenital heart diseases) between October 2010 and July 2011.
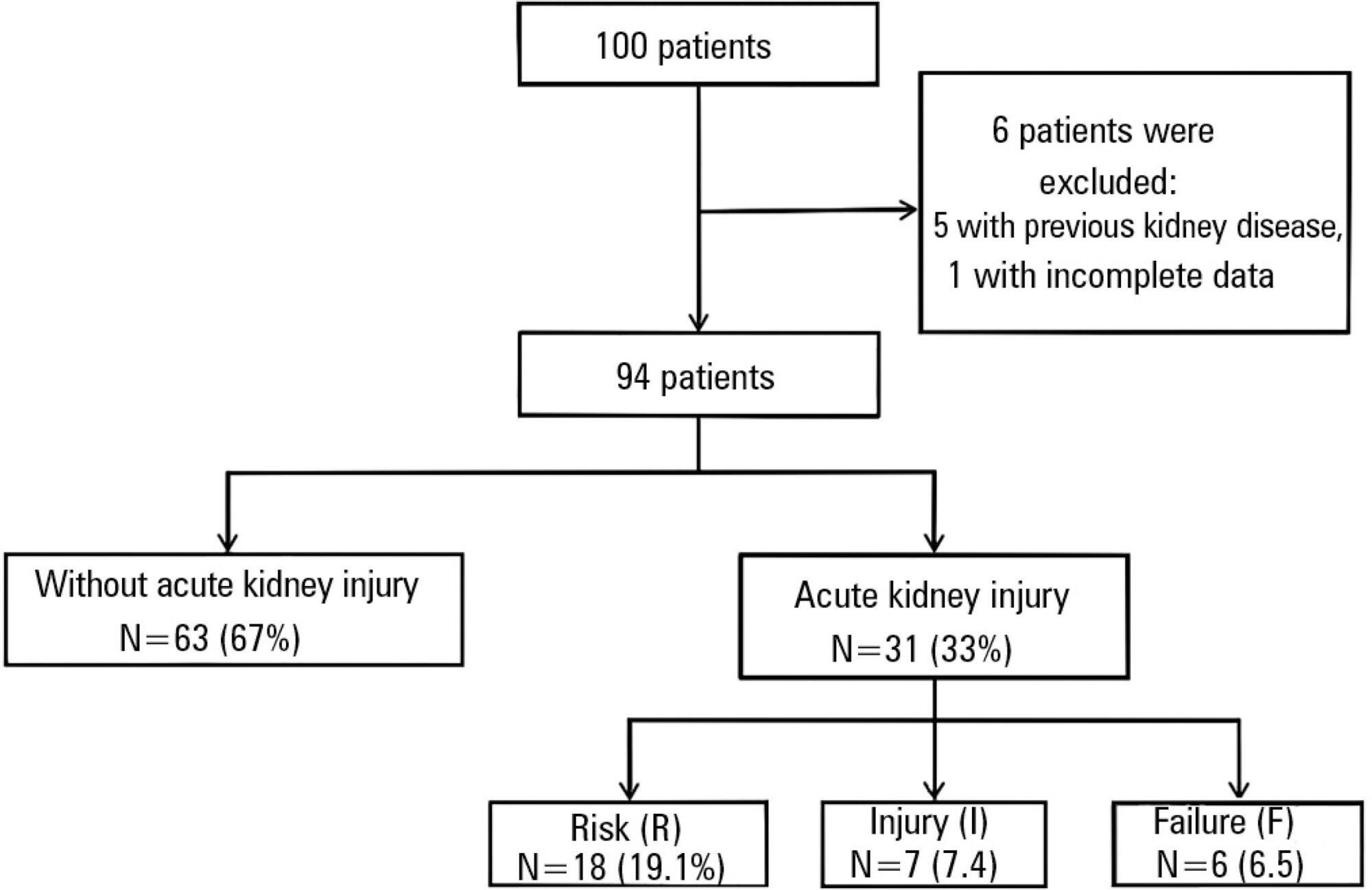
One hundred patients were assessed. Among the 100 patients, six were excluded, including five because of prior kidney disease or dialysis therapy and one because of incomplete medical records. The primary surgical indications were myocardial revascularization in 55 patients (58.5% of cases) and valve replacement in 28 patients (29.8%). According to the EuroSCORE, 55 patients were classified as high risk (58.5%), 27 patients as medium risk (28.7%) and 12 patients as low risk (12.8%). In the postoperative period, patients were classified with the Risk, Injury, Failure, Loss and End-stage kidney disease (RIFLE) score. Among the 31 patients (33%) who displayed an increase in serum creatinine, 18 patients (19.1%) were classified as RIFLE "R" (risk), seven patients (7.4%) were classified as RIFLE "I" (injury) and six patients (6.5%) were classified as RIFLE "F" (failure). Among the patients who were considered to be high risk according to the EuroSCORE criteria, 24 patients (43.6%) showed acute kidney injury. Among the patients who were classified as medium or low risk, acute kidney injury occurred in 18.5 and 16.6% of the cases, respectively. The correlations between risk stratification (low, medium and high) and the EuroSCORE and postoperative RIFLE scores were statistically significant (p=0.03).
In the studied population, there was a statistically significant correlation between the EuroSCORE and the risk of developing acute kidney injury in the postoperative period after cardiac surgery.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):233-238
DOI 10.5935/0103-507X.20130040
The objective of this study was to assess the correlation between the European System for Cardiac Operative Risk Evaluation (EuroSCORE) score and the risk of developing acute kidney injury in cardiac surgery patients.
This retrospective study was conducted at a tertiary hospital on consecutive cardiac surgery patients (e.g., valvular, ischemic and congenital heart diseases) between October 2010 and July 2011.
One hundred patients were assessed. Among the 100 patients, six were excluded, including five because of prior kidney disease or dialysis therapy and one because of incomplete medical records. The primary surgical indications were myocardial revascularization in 55 patients (58.5% of cases) and valve replacement in 28 patients (29.8%). According to the EuroSCORE, 55 patients were classified as high risk (58.5%), 27 patients as medium risk (28.7%) and 12 patients as low risk (12.8%). In the postoperative period, patients were classified with the Risk, Injury, Failure, Loss and End-stage kidney disease (RIFLE) score. Among the 31 patients (33%) who displayed an increase in serum creatinine, 18 patients (19.1%) were classified as RIFLE "R" (risk), seven patients (7.4%) were classified as RIFLE "I" (injury) and six patients (6.5%) were classified as RIFLE "F" (failure). Among the patients who were considered to be high risk according to the EuroSCORE criteria, 24 patients (43.6%) showed acute kidney injury. Among the patients who were classified as medium or low risk, acute kidney injury occurred in 18.5 and 16.6% of the cases, respectively. The correlations between risk stratification (low, medium and high) and the EuroSCORE and postoperative RIFLE scores were statistically significant (p=0.03).
In the studied population, there was a statistically significant correlation between the EuroSCORE and the risk of developing acute kidney injury in the postoperative period after cardiac surgery.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):312-318
DOI 10.5935/0103-507X.20130053
The development of abdominal surgery represents an alternative therapy for the morbidly obese; however, patients undergoing this surgical procedure often experience postoperative pulmonary complications. The use of alveolar recruitment maneuvers and/or perioperative ventilatory strategies is a possible alternative to reduce these complications, focusing on the reduction of postoperative pulmonary complications. In this review, the benefits of perioperative ventilatory strategies and the implementation of alveolar recruitment maneuvers in obese patients undergoing abdominal surgery are described.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):312-318
DOI 10.5935/0103-507X.20130053
The development of abdominal surgery represents an alternative therapy for the morbidly obese; however, patients undergoing this surgical procedure often experience postoperative pulmonary complications. The use of alveolar recruitment maneuvers and/or perioperative ventilatory strategies is a possible alternative to reduce these complications, focusing on the reduction of postoperative pulmonary complications. In this review, the benefits of perioperative ventilatory strategies and the implementation of alveolar recruitment maneuvers in obese patients undergoing abdominal surgery are described.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald's statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population's attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):312-320
DOI 10.1590/S0103-507X2011000300009
OBJECTIVE: To evaluate associations between post-operative complications in patients who survive surgery and in-hospital deaths and lengths of hospital stays of patients who undergo coronary artery bypass graft surgery METHODS: Patients who underwent coronary artery bypass graft surgery and survived the operating theater were randomly selected. Information on complications and hospital lengths of stay until hospital discharge or death were retrospectively collected based on medical records and declarations of death. These aspects were estimated according to the presence of complications, frequency of complications, mortality, relative risk and attributable population risk. Mean hospital lengths of stay were compared using Wald's statistics. RESULTS: Medical records indicating deaths in the operating theater were excluded, and 86.9% of the included records reported complications; the greatest loss of information (43.9%) was related to kidney failure. Hyperglycemia was estimated as the most frequent complication (74.6%), with an attributable risk of 31.6%. The population's attributable risks were greater than 60% for low cardiac output (77.0%), kidney failure (64.3%) and cardiorespiratory failure (60.4%). Twelve different situations were identified for paired combinations of significant differences between average post-operative hospitalization times and complications, according to the outcome of discharge or death. CONCLUSION: Several complications were identified during the postoperative period of coronary artery bypass graft surgery, with different frequencies and impacts on mortality. Control of the myocardium at the risk of ischemia, hemodynamic stabilization and volume replacement strategies may be effective for controlling mortality rates and shortening hospital lengths of stay.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):89-95
DOI 10.1590/S0103-507X2009000100013
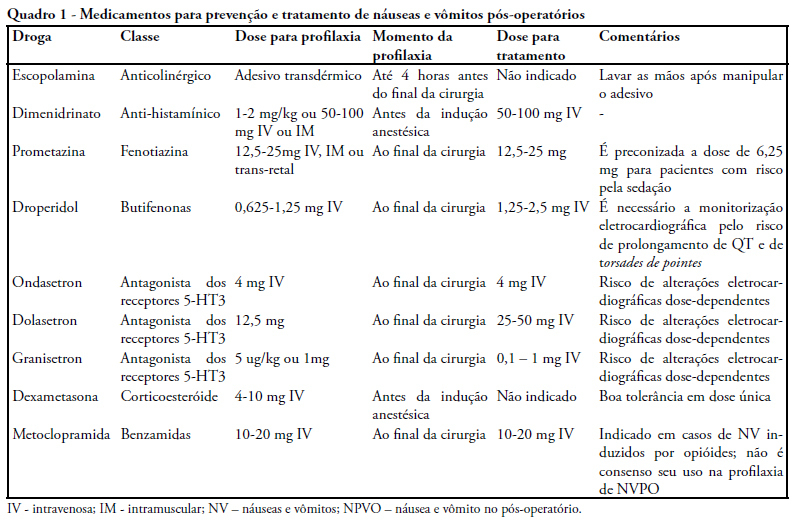
Postoperative nausea and vomiting are common and can be prevented. Complications of this condition cause higher rates of morbidity and mortality. A review of literature was carried out on MEDLINE, with focus on controlled clinical trials. Pathophysiology is complex, with many afferent and efferent pathways, and its comprehension facilitate the choice of medication. Risk factors are presented, with a stratified score of chance to develop postoperative nausea and vomiting. An algorithm for identification of higher risk patients was elaborated and classified the level of prevention/treatment recommended to avoid excessive use of drugs and their side effects. Postoperative nausea and vomiting must be prevented, because of the involved complications and discomfort for patients. A systematic approach with analysis of preoperative risk factors and prescription of medication can be effective for prevention.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):89-95
DOI 10.1590/S0103-507X2009000100013
Postoperative nausea and vomiting are common and can be prevented. Complications of this condition cause higher rates of morbidity and mortality. A review of literature was carried out on MEDLINE, with focus on controlled clinical trials. Pathophysiology is complex, with many afferent and efferent pathways, and its comprehension facilitate the choice of medication. Risk factors are presented, with a stratified score of chance to develop postoperative nausea and vomiting. An algorithm for identification of higher risk patients was elaborated and classified the level of prevention/treatment recommended to avoid excessive use of drugs and their side effects. Postoperative nausea and vomiting must be prevented, because of the involved complications and discomfort for patients. A systematic approach with analysis of preoperative risk factors and prescription of medication can be effective for prevention.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
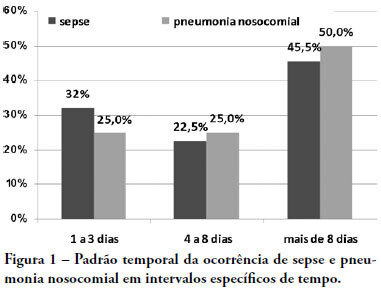
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):226-234
DOI 10.1590/S0103-507X2008000300004
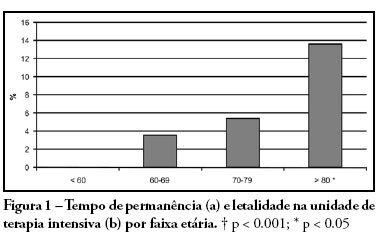
PURPOSE: Due to the increasing longevity of the and high prevalence of coronary heart disease in the aged , coronary artery bypass graft surgery has become frequent in older patients. The purpose of this study is to describe operative features, length of stay, complications and short term outcomes after coronary artery bypass graft in such patients. METHODS: From February 2005 to October 2007, 269 patients underwent coronary artery bypass graft. Demographic data, comorbidities, prognostic scores, coronary artery bypass graft elective versus urgent indication, intensive care unit length of stay, postoperative complications and intensive care unit mortality were recorded. Intra-operative characteristics, such as total surgery time, use of bypass device, on-pump time, urine output, fluid balance, use of blood products and number of grafts, were analyzed. Patients were divided in four age groups: group I (< 60 n = 68), II (60 to 69 n = 86), III (70 to 79 n = 93) IV and older than 80 years (n = 22). RESULTS: Group IV patients were more frequently submitted to coronary artery bypass graft combined with valve replacement, emergency surgery, and had longer stay in the intensive care unit (p < 0.01). The incidence of at least one postoperative complication was also higher among patients older than 80 (p < 0.001). Multivariate analysis identified age and on-pump time as independent risk factors for development of complications. Mortality increased in patients older than 70 years (p = 0.03). CONCLUSIONS: Octogenarian patients undergoing coronary artery bypass graft have longer intensive care unit length of stay, incidence of complications and mortality. Age and on-pump time were independent risk factors associated with the incidence of postoperative complications.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):226-234
DOI 10.1590/S0103-507X2008000300004
PURPOSE: Due to the increasing longevity of the and high prevalence of coronary heart disease in the aged , coronary artery bypass graft surgery has become frequent in older patients. The purpose of this study is to describe operative features, length of stay, complications and short term outcomes after coronary artery bypass graft in such patients. METHODS: From February 2005 to October 2007, 269 patients underwent coronary artery bypass graft. Demographic data, comorbidities, prognostic scores, coronary artery bypass graft elective versus urgent indication, intensive care unit length of stay, postoperative complications and intensive care unit mortality were recorded. Intra-operative characteristics, such as total surgery time, use of bypass device, on-pump time, urine output, fluid balance, use of blood products and number of grafts, were analyzed. Patients were divided in four age groups: group I (< 60 n = 68), II (60 to 69 n = 86), III (70 to 79 n = 93) IV and older than 80 years (n = 22). RESULTS: Group IV patients were more frequently submitted to coronary artery bypass graft combined with valve replacement, emergency surgery, and had longer stay in the intensive care unit (p < 0.01). The incidence of at least one postoperative complication was also higher among patients older than 80 (p < 0.001). Multivariate analysis identified age and on-pump time as independent risk factors for development of complications. Mortality increased in patients older than 70 years (p = 0.03). CONCLUSIONS: Octogenarian patients undergoing coronary artery bypass graft have longer intensive care unit length of stay, incidence of complications and mortality. Age and on-pump time were independent risk factors associated with the incidence of postoperative complications.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)