
You searched for:"Marcelo de Oliveira Maia"
We found (3) results for your search.-
Articles
Contrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
Abstract
ArticlesContrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
DOI 10.5935/0103-507X.20170041
Views0ABSTRACT
Objective:
To establish whether there is superiority between contrast-induced acute kidney injury and contrast-induced nephropathy criteria as predictors of unfavorable clinical outcomes.
Methods:
Retrospective study carried out in a tertiary hospital with 157 patients undergoing radiocontrast infusion for propaedeutic purposes.
Results:
One hundred forty patients fulfilled the inclusion criteria: patients who met the criteria for contrast-induced acute kidney injury (59) also met the criteria for contrast-induced nephropathy (76), 44.3% met the criteria for KDIGO staging, 6.4% of the patients required renal replacement therapy, and 10.7% died.
Conclusion:
The diagnosis of contrast-induced nephropathy was the most sensitive criterion for renal replacement therapy and death, whereas KDIGO showed the highest specificity; there was no correlation between contrast volume and progression to contrast-induced acute kidney injury, contrast-induced nephropathy, support dialysis or death in the assessed population.
Keywords:Acute kidney injury/chemically inducedContrast media/adverse effectsPrognosisRenal dialysisRisk assessmentSeverity of illness indexSee moreViews0

Abstract
ArticlesContrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
DOI 10.5935/0103-507X.20170041
Views0ABSTRACT
Objective:
To establish whether there is superiority between contrast-induced acute kidney injury and contrast-induced nephropathy criteria as predictors of unfavorable clinical outcomes.
Methods:
Retrospective study carried out in a tertiary hospital with 157 patients undergoing radiocontrast infusion for propaedeutic purposes.
Results:
One hundred forty patients fulfilled the inclusion criteria: patients who met the criteria for contrast-induced acute kidney injury (59) also met the criteria for contrast-induced nephropathy (76), 44.3% met the criteria for KDIGO staging, 6.4% of the patients required renal replacement therapy, and 10.7% died.
Conclusion:
The diagnosis of contrast-induced nephropathy was the most sensitive criterion for renal replacement therapy and death, whereas KDIGO showed the highest specificity; there was no correlation between contrast volume and progression to contrast-induced acute kidney injury, contrast-induced nephropathy, support dialysis or death in the assessed population.
Keywords:Acute kidney injury/chemically inducedContrast media/adverse effectsPrognosisRenal dialysisRisk assessmentSeverity of illness indexSee more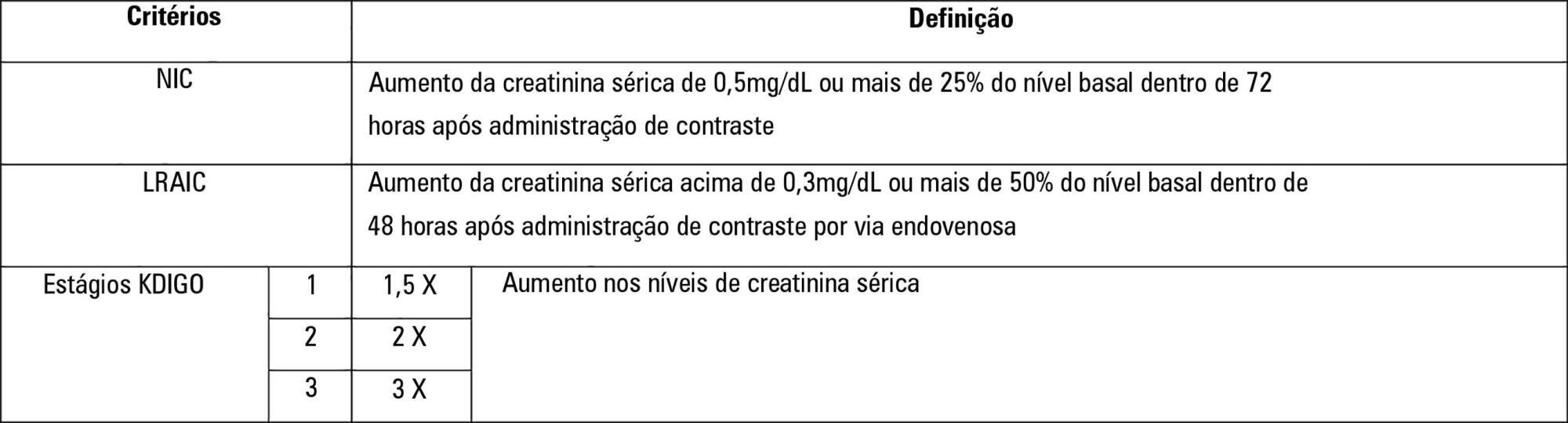
-
Case Report
Acute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
Abstract
Case ReportAcute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Views0Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin’s lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary “ground glass” opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient’s clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Keywords:Case reportsCryptogenic organizing pneumoniaDrug toxicityLung diseases, interstitialLymphoma, non-HodgkinRespiratory insufficiencyTomography, X-ray computedSee moreViews0Abstract
Case ReportAcute respiratory failure caused by organizing pneumonia secondary to antineoplastic therapy for non-Hodgkin’s lymphoma
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Views0Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin’s lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary “ground glass” opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient’s clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Keywords:Case reportsCryptogenic organizing pneumoniaDrug toxicityLung diseases, interstitialLymphoma, non-HodgkinRespiratory insufficiencyTomography, X-ray computedSee more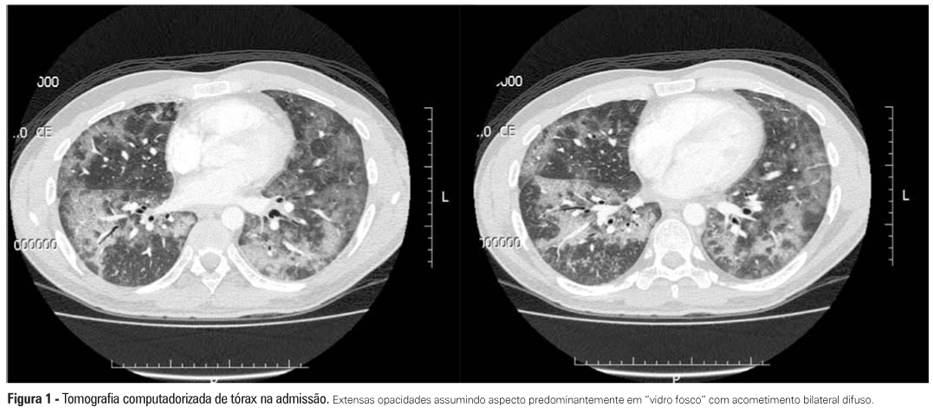
-
Original Articles
Epidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
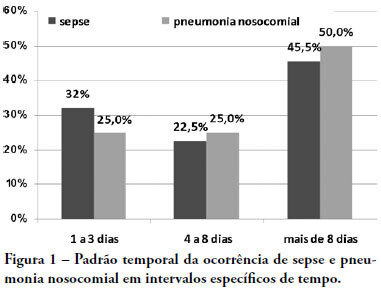
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Views0Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis