Drug toxicity Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
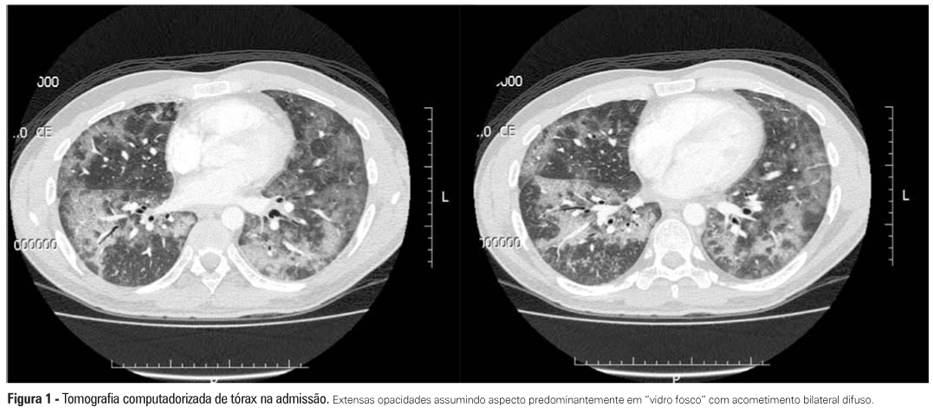
Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin's lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary "ground glass" opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient's clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):415-419
DOI 10.1590/S0103-507X2012000400020
Interstitial lung diseases belong to a group of diseases that typically exhibit a subacute or chronic progression but that may cause acute respiratory failure. The male patient, who was 37 years of age and undergoing therapy for non-Hodgkin's lymphoma, was admitted with cough, fever, dyspnea and acute hypoxemic respiratory failure. Mechanical ventilation and antibiotic therapy were initiated but were associated with unfavorable progression. Thoracic computed tomography showed bilateral pulmonary "ground glass" opacities. Methylprednisolone pulse therapy was initiated with satisfactory response because the patient had used three drugs related to organizing pneumonia (cyclophosphamide, doxorubicin and rituximab), and the clinical and radiological symptoms were suggestive. Organizing pneumonia may be idiopathic or linked to collagen diseases, drugs and cancer and usually responds to corticosteroid therapy. The diagnosis was anatomopathological, but the patient's clinical condition precluded performing a lung biopsy. Organizing pneumonia should be a differential diagnosis in patients with apparent pneumonia and a progression that is unfavorable to antimicrobial treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
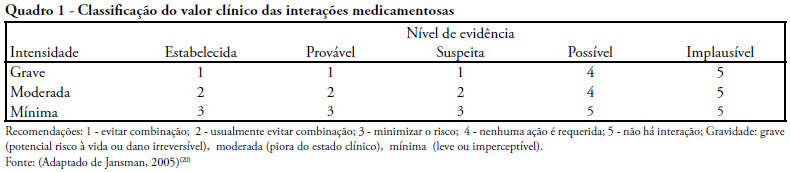
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)