Gastrointestinal tract Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2010;22(4):346-350
DOI 10.1590/S0103-507X2010000400006
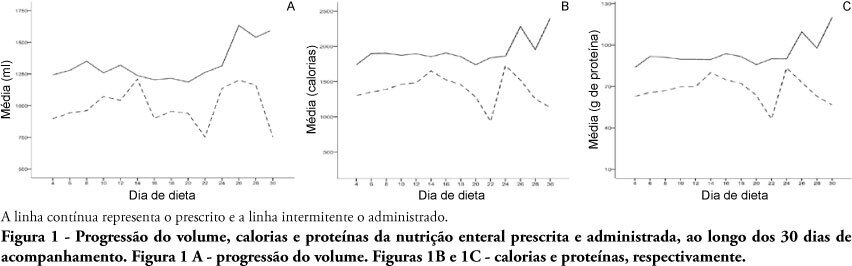
OBJECTIVES: Different conditions require that critically ill patients to receive lower than prescribed enteral nutrition volumes, energy and protein. This study objective was to evaluate the prescribed versus administered enteral nutrition difference in adults admitted to an intensive care unit. METHODS: In 2009, patients were followed for 30 days from the start of enteral nutrition to its discontinuation, or discharge from the intensive care unit. Parametric and nonparametric tests were used to evaluate prescribed versus administered differences. RESULTS: Eighty five patients were enrolled; mean age was 58.6±18.0 years and 40% were male. The patients remained in hospital for 29.5 days (IQ: 15.2 - 48.7) and were under enteral nutrition for 10 (IQ: 4.2 - 27.5) days. Lower than enteral nutrition prescribed volume (-428±243ml/day), energy (-665±412 Kcal/day) and protein (-30±19 g protein/day) was received. Individual patients' evaluation demonstrated that about 40% of the prescribed volume was not actually given. The main reasons for enteral nutrition interruptions were nausea and vomiting, abdominal distension, constipation and clinical complications (52%); diagnostic procedures (41.6%); and transition to oral feeding (5.6%). CONCLUSION: Patients admitted to intensive care unit receive less than the prescribed enteral nutrition. The routine care and gastrointestinal tract complications lead to enteral nutrition interruptions, contributing to less than prescribed calories administration.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):346-350
DOI 10.1590/S0103-507X2010000400006
OBJECTIVES: Different conditions require that critically ill patients to receive lower than prescribed enteral nutrition volumes, energy and protein. This study objective was to evaluate the prescribed versus administered enteral nutrition difference in adults admitted to an intensive care unit. METHODS: In 2009, patients were followed for 30 days from the start of enteral nutrition to its discontinuation, or discharge from the intensive care unit. Parametric and nonparametric tests were used to evaluate prescribed versus administered differences. RESULTS: Eighty five patients were enrolled; mean age was 58.6±18.0 years and 40% were male. The patients remained in hospital for 29.5 days (IQ: 15.2 - 48.7) and were under enteral nutrition for 10 (IQ: 4.2 - 27.5) days. Lower than enteral nutrition prescribed volume (-428±243ml/day), energy (-665±412 Kcal/day) and protein (-30±19 g protein/day) was received. Individual patients' evaluation demonstrated that about 40% of the prescribed volume was not actually given. The main reasons for enteral nutrition interruptions were nausea and vomiting, abdominal distension, constipation and clinical complications (52%); diagnostic procedures (41.6%); and transition to oral feeding (5.6%). CONCLUSION: Patients admitted to intensive care unit receive less than the prescribed enteral nutrition. The routine care and gastrointestinal tract complications lead to enteral nutrition interruptions, contributing to less than prescribed calories administration.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):118-124
DOI 10.1590/S0103-507X2010000200004
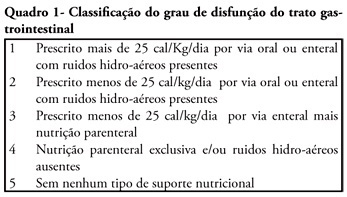
OBJECTIVE: We aimed to investigate the prevalence and independent predictors of prolonged gastrointestinal dysfunction in critically ill patients admitted to the intensive care unit. METHODS: Retrospective and observational cohort study performed in a mixed 24 beds intensive care unit in a tertiary center. Patients admitted in the intensive care unit between August 2003 and January 2004, who had a length of stay in the intensive care unit greater than 4 days were enrolled. Gastrointestinal function was evaluated daily according to a classification that considered physical examination (bowel sounds or distension) and the nutritional support progress. RESULTS: Were included 128 patients. The mean age was 56 ± 19 years, 63.3% were male and 77.3% were surgical patients. Prolonged gastrointestinal dysfunction occurred in 35% of patients, with prevalence 3.3 times higher in surgical patients (27%) than in medical patients (8%). Endoscopies were performed in 38 patients (29.7%), and in three quarters of them erosive lesions and or bleeding were observed. Gastrointestinal dysfunction was more frequent in patients presenting moderate or severe edema (51%) than in patients without edema (22.5%) (p<0.05). In the logistic regression analysis, a serum lactate level higher than 5.2 mEq/L (RR 6.69 95%CI 15-38.7, P = 0.034) and the presence of a low oxygenation index (RR 12.4 95%CI 2.18-70.8, p = 0.005) were predictive of gastrointestinal dysfunction. CONCLUSION: Prolonged gastrointestinal dysfunction was highly prevalent in this heterogeneous population of critically ill patients. Admission high serum lactate levels and a low oxygenation index were predictive of prolonged gastrointestinal dysfunction.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):118-124
DOI 10.1590/S0103-507X2010000200004
OBJECTIVE: We aimed to investigate the prevalence and independent predictors of prolonged gastrointestinal dysfunction in critically ill patients admitted to the intensive care unit. METHODS: Retrospective and observational cohort study performed in a mixed 24 beds intensive care unit in a tertiary center. Patients admitted in the intensive care unit between August 2003 and January 2004, who had a length of stay in the intensive care unit greater than 4 days were enrolled. Gastrointestinal function was evaluated daily according to a classification that considered physical examination (bowel sounds or distension) and the nutritional support progress. RESULTS: Were included 128 patients. The mean age was 56 ± 19 years, 63.3% were male and 77.3% were surgical patients. Prolonged gastrointestinal dysfunction occurred in 35% of patients, with prevalence 3.3 times higher in surgical patients (27%) than in medical patients (8%). Endoscopies were performed in 38 patients (29.7%), and in three quarters of them erosive lesions and or bleeding were observed. Gastrointestinal dysfunction was more frequent in patients presenting moderate or severe edema (51%) than in patients without edema (22.5%) (p<0.05). In the logistic regression analysis, a serum lactate level higher than 5.2 mEq/L (RR 6.69 95%CI 15-38.7, P = 0.034) and the presence of a low oxygenation index (RR 12.4 95%CI 2.18-70.8, p = 0.005) were predictive of gastrointestinal dysfunction. CONCLUSION: Prolonged gastrointestinal dysfunction was highly prevalent in this heterogeneous population of critically ill patients. Admission high serum lactate levels and a low oxygenation index were predictive of prolonged gastrointestinal dysfunction.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
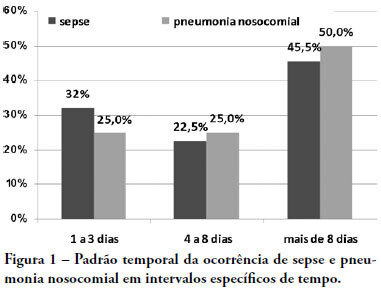
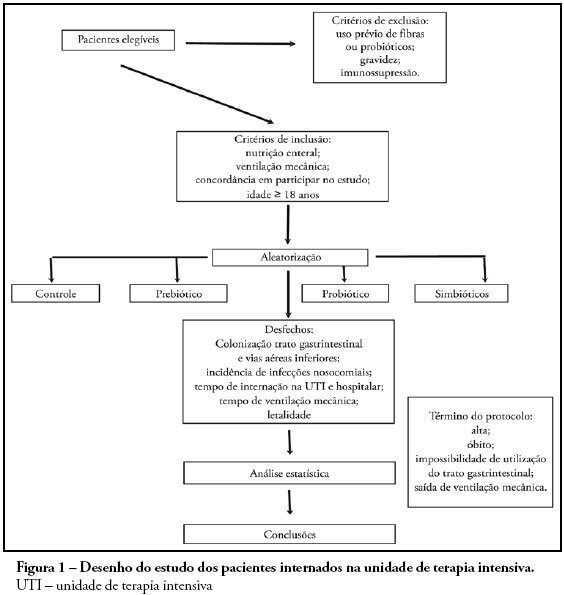
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)