Pneumonia, ventilator-associated Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):310-316
DOI 10.5935/0103-507X.20170039
To phenotypically evaluate biofilm production by Pseudomonas aeruginosa clinically isolated from patients with ventilator-associated pneumonia.
Twenty clinical isolates of P. aeruginosa were analyzed, 19 of which were from clinical samples of tracheal aspirate, and one was from a bronchoalveolar lavage sample. The evaluation of the capacity of P. aeruginosa to produce biofilm was verified using two techniques, one qualitative and the other quantitative.
The qualitative technique showed that only 15% of the isolates were considered biofilm producers, while the quantitative technique showed that 75% of the isolates were biofilm producers. The biofilm isolates presented the following susceptibility profile: 53.3% were multidrug-resistant, and 46.7% were multidrug-sensitive.
The quantitative technique was more effective than the qualitative technique for the detection of biofilm production. For the bacterial population analyzed, biofilm production was independent of the susceptibility profile of the bacteria, demonstrating that the therapeutic failure could be related to biofilm production, as it prevented the destruction of the bacteria present in this structure, causing complications of pneumonia associated with mechanical ventilation, including extrapulmonary infections, and making it difficult to treat the infection.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):310-316
DOI 10.5935/0103-507X.20170039
To phenotypically evaluate biofilm production by Pseudomonas aeruginosa clinically isolated from patients with ventilator-associated pneumonia.
Twenty clinical isolates of P. aeruginosa were analyzed, 19 of which were from clinical samples of tracheal aspirate, and one was from a bronchoalveolar lavage sample. The evaluation of the capacity of P. aeruginosa to produce biofilm was verified using two techniques, one qualitative and the other quantitative.
The qualitative technique showed that only 15% of the isolates were considered biofilm producers, while the quantitative technique showed that 75% of the isolates were biofilm producers. The biofilm isolates presented the following susceptibility profile: 53.3% were multidrug-resistant, and 46.7% were multidrug-sensitive.
The quantitative technique was more effective than the qualitative technique for the detection of biofilm production. For the bacterial population analyzed, biofilm production was independent of the susceptibility profile of the bacteria, demonstrating that the therapeutic failure could be related to biofilm production, as it prevented the destruction of the bacteria present in this structure, causing complications of pneumonia associated with mechanical ventilation, including extrapulmonary infections, and making it difficult to treat the infection.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):55-62
DOI 10.5935/0103-507X.20170009
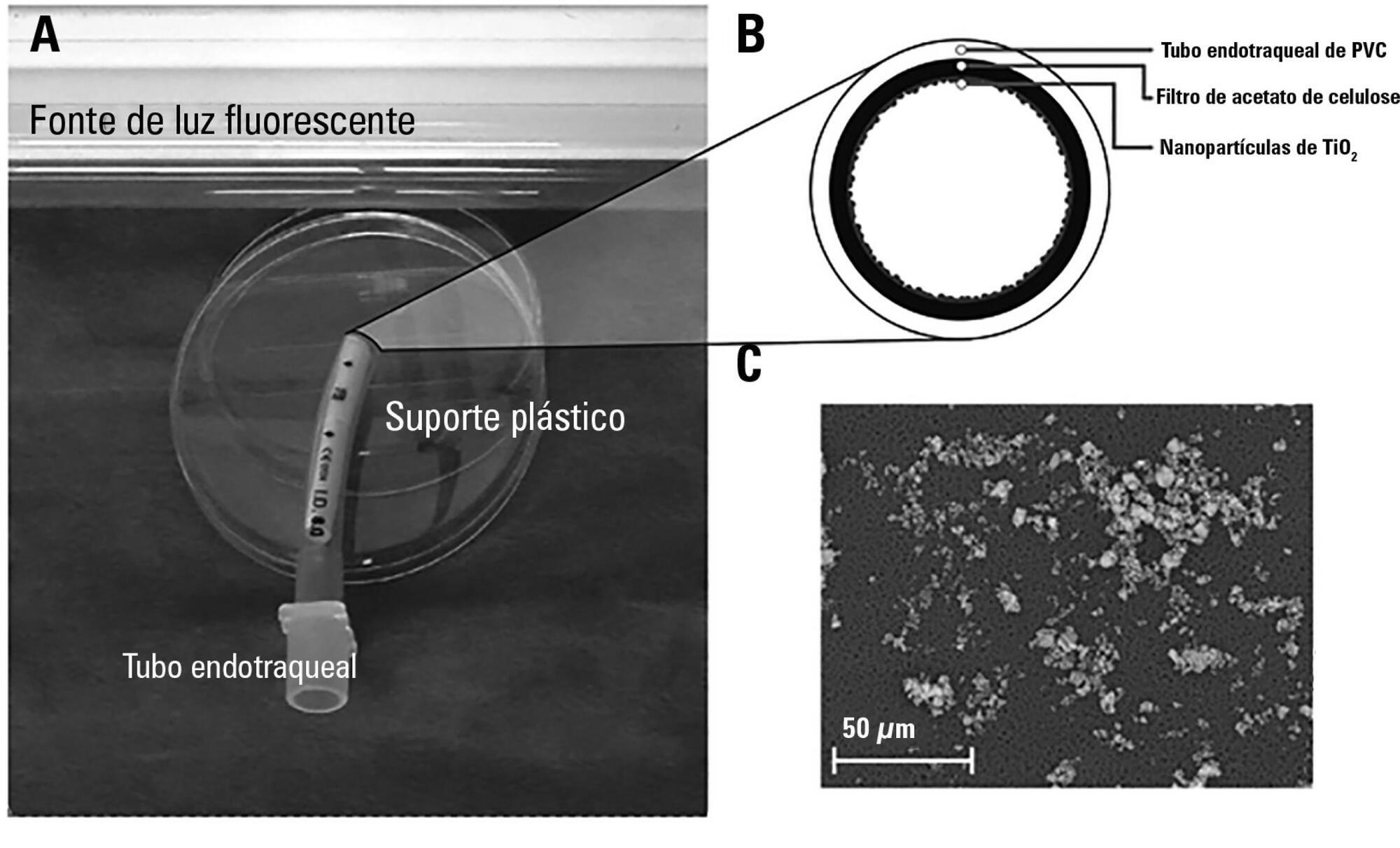
The aim of this study was to assess the antibacterial activity against Staphylococcus aureus and Pseudomonas aeruginosa of two nanoparticle endotracheal tube coatings with visible light-induced photocatalysis.
Two types of titanium dioxide nanoparticles were tested: standard anatase (TiO2) and N-doped TiO2 (N-TiO2). Nanoparticles were placed on the internal surface of a segment of commercial endotracheal tubes, which were loaded on a cellulose acetate filter; control endotracheal tubes were left without a nanoparticle coating. A bacterial inoculum of 150 colony forming units was placed in the endotracheal tubes and then exposed to a fluorescent light source (3700 lux, 300-700 nm wavelength) for 5, 10, 20, 40, 60 and 80 minutes. Colony forming units were counted after 24 hours of incubation at 37°C. Bacterial inactivation was calculated as the percentage reduction of bacterial growth compared to endotracheal tubes not exposed to light.
In the absence of light, no relevant antibacterial activity was shown against neither strain. For P. aeruginosa, both coatings had a higher bacterial inactivation than controls at any time point (p < 0.001), and no difference was observed between TiO2 and N-TiO2. For S. aureus, inactivation was higher than for controls starting at 5 minutes for N-TiO2 (p = 0.018) and 10 minutes for TiO2 (p = 0.014); inactivation with N-TiO2 was higher than that with TiO2 at 20 minutes (p < 0.001), 40 minutes (p < 0.001) and 60 minutes (p < 0.001).
Nanosized commercial and N-doped TiO2 inhibit bacterial growth under visible fluorescent light. N-TiO2 has higher antibacterial activity against S. aureus compared to TiO2.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):55-62
DOI 10.5935/0103-507X.20170009
The aim of this study was to assess the antibacterial activity against Staphylococcus aureus and Pseudomonas aeruginosa of two nanoparticle endotracheal tube coatings with visible light-induced photocatalysis.
Two types of titanium dioxide nanoparticles were tested: standard anatase (TiO2) and N-doped TiO2 (N-TiO2). Nanoparticles were placed on the internal surface of a segment of commercial endotracheal tubes, which were loaded on a cellulose acetate filter; control endotracheal tubes were left without a nanoparticle coating. A bacterial inoculum of 150 colony forming units was placed in the endotracheal tubes and then exposed to a fluorescent light source (3700 lux, 300-700 nm wavelength) for 5, 10, 20, 40, 60 and 80 minutes. Colony forming units were counted after 24 hours of incubation at 37°C. Bacterial inactivation was calculated as the percentage reduction of bacterial growth compared to endotracheal tubes not exposed to light.
In the absence of light, no relevant antibacterial activity was shown against neither strain. For P. aeruginosa, both coatings had a higher bacterial inactivation than controls at any time point (p < 0.001), and no difference was observed between TiO2 and N-TiO2. For S. aureus, inactivation was higher than for controls starting at 5 minutes for N-TiO2 (p = 0.018) and 10 minutes for TiO2 (p = 0.014); inactivation with N-TiO2 was higher than that with TiO2 at 20 minutes (p < 0.001), 40 minutes (p < 0.001) and 60 minutes (p < 0.001).
Nanosized commercial and N-doped TiO2 inhibit bacterial growth under visible fluorescent light. N-TiO2 has higher antibacterial activity against S. aureus compared to TiO2.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
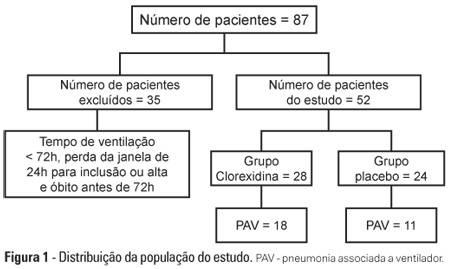
OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):401-406
DOI 10.1590/S0103-507X2012000400018
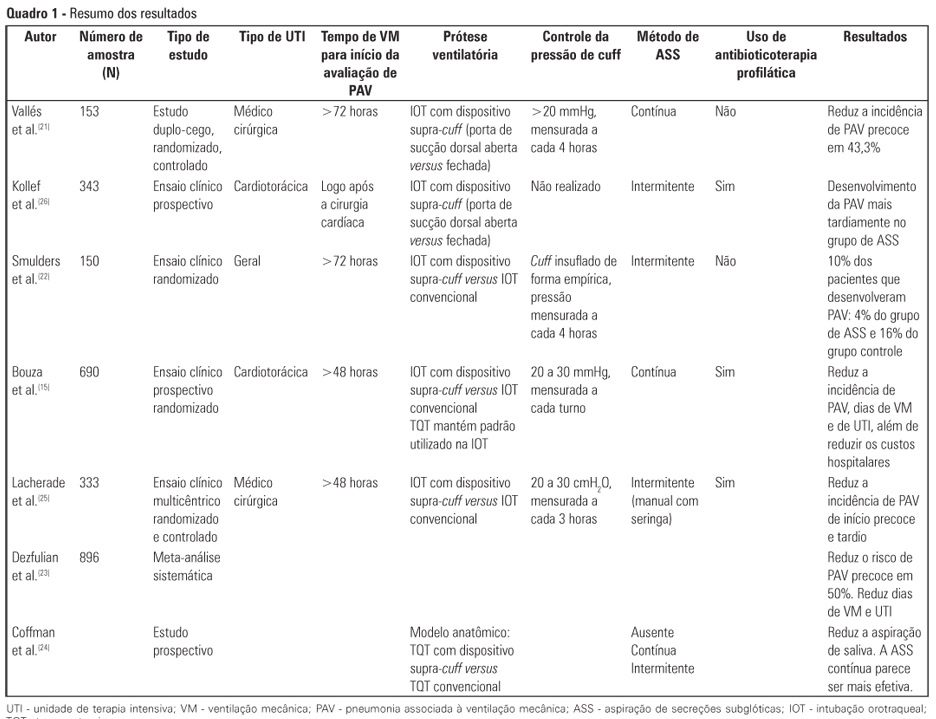
Critically ill patients are intubated or tracheostomized because, in most cases, these individuals require invasive mechanical ventilation. The cannulae that are used include the cuff, which can act as a reservoir for oropharyngeal secretions, predisposing to ventilator-associated pneumonia. Studies have revealed that the suction of subglottic secretions through the dorsal suction lumen above the endotracheal tube cuff delays the onset and reduces the incidence of ventilator-associated pneumonia. The aim of this review is to assess published studies regarding the significance of using suction with a supra-cuff device for the prevention of ventilator-associated pneumonia in critically ill patients treated with orotracheal intubation or tracheostomy. Therefore, by searching national and international databases, a literature review was undertaken of studies published between the years 1986 and 2011. Few results were found relating the suction of subglottic secretions to decreased duration of mechanical ventilation and length of stay in the intensive care unit. The suction of subglottic secretions is ineffective in decreasing mortality but is effective in reducing the incidence of early-onset ventilator-associated pneumonia and hospital costs. Techniques involving continuous suction of subglottic secretions may be particularly efficient in removing secretions; however, intermittent suction appears to be the least harmful method. In conclusion, cannulae with a supra-cuff suction device enable the aspiration of subglottic secretions, providing benefits to critically ill patients by reducing the incidence of ventilator-associated pneumonia and, consequently, hospital costs - with no large-scale adverse effects.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):401-406
DOI 10.1590/S0103-507X2012000400018
Critically ill patients are intubated or tracheostomized because, in most cases, these individuals require invasive mechanical ventilation. The cannulae that are used include the cuff, which can act as a reservoir for oropharyngeal secretions, predisposing to ventilator-associated pneumonia. Studies have revealed that the suction of subglottic secretions through the dorsal suction lumen above the endotracheal tube cuff delays the onset and reduces the incidence of ventilator-associated pneumonia. The aim of this review is to assess published studies regarding the significance of using suction with a supra-cuff device for the prevention of ventilator-associated pneumonia in critically ill patients treated with orotracheal intubation or tracheostomy. Therefore, by searching national and international databases, a literature review was undertaken of studies published between the years 1986 and 2011. Few results were found relating the suction of subglottic secretions to decreased duration of mechanical ventilation and length of stay in the intensive care unit. The suction of subglottic secretions is ineffective in decreasing mortality but is effective in reducing the incidence of early-onset ventilator-associated pneumonia and hospital costs. Techniques involving continuous suction of subglottic secretions may be particularly efficient in removing secretions; however, intermittent suction appears to be the least harmful method. In conclusion, cannulae with a supra-cuff suction device enable the aspiration of subglottic secretions, providing benefits to critically ill patients by reducing the incidence of ventilator-associated pneumonia and, consequently, hospital costs - with no large-scale adverse effects.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):80-88
DOI 10.1590/S0103-507X2009000100012
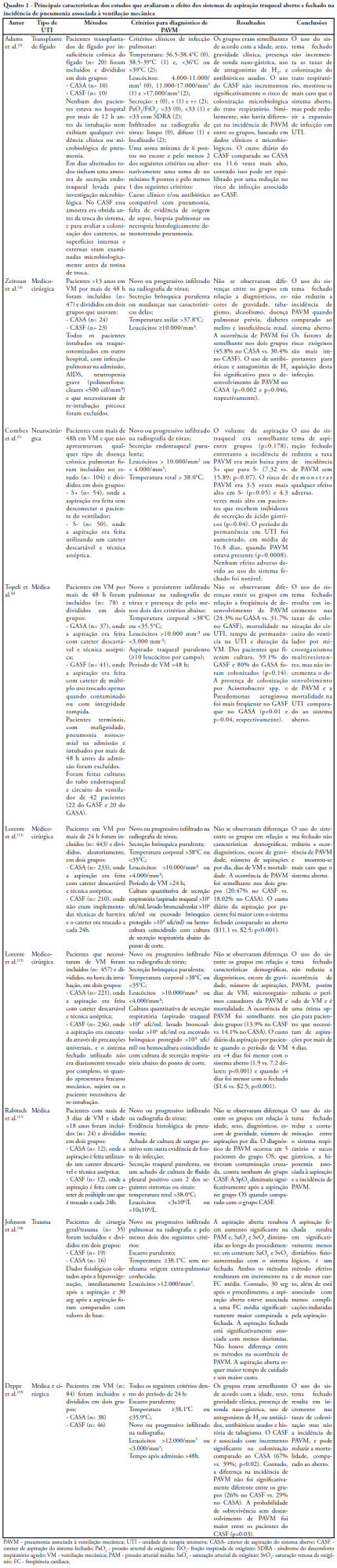
Pneumonia is the most common nosocominal infection in intensive care units and mechanical ventilation is a significant factor associated to its development. The objective of this study was to describe the impact of the open and closed tracheal suction systems on the incidence of ventilation-associated pneumonia. A search in the Pubmed database was performed to identify randomized controlled trials, published from 1990 to November 2008. Nine studies were included. Of the studies reviewed, seven did not disclose any significant advantages of using the closed system when compared to th e open, whereas two reported that use of the closed system increased colonization rates but not incidence of ventilation-associated pneumonia and one observed that use of the closed system did not increase colonization of the respiratory tract but reduced the spread of infection resulting in decreased sepsis rates. Only two studies found a reduction in the incidence of ventilation-associated pneumonia with use of the closed system, and one revealed a 3.5 times greater risk of developing this infection with the open system. Results suggest that the impact of the open and closed tracheal suction system is similar on development of ventilation-associated pneumonia, choice of the suction system should therefore be based on other parameters. While the closed system increases risk of colonization of the respiratory tract, but has the advantages of continuing mechanical ventilation and lessening hemodynamic impairment.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):80-88
DOI 10.1590/S0103-507X2009000100012
Pneumonia is the most common nosocominal infection in intensive care units and mechanical ventilation is a significant factor associated to its development. The objective of this study was to describe the impact of the open and closed tracheal suction systems on the incidence of ventilation-associated pneumonia. A search in the Pubmed database was performed to identify randomized controlled trials, published from 1990 to November 2008. Nine studies were included. Of the studies reviewed, seven did not disclose any significant advantages of using the closed system when compared to th e open, whereas two reported that use of the closed system increased colonization rates but not incidence of ventilation-associated pneumonia and one observed that use of the closed system did not increase colonization of the respiratory tract but reduced the spread of infection resulting in decreased sepsis rates. Only two studies found a reduction in the incidence of ventilation-associated pneumonia with use of the closed system, and one revealed a 3.5 times greater risk of developing this infection with the open system. Results suggest that the impact of the open and closed tracheal suction system is similar on development of ventilation-associated pneumonia, choice of the suction system should therefore be based on other parameters. While the closed system increases risk of colonization of the respiratory tract, but has the advantages of continuing mechanical ventilation and lessening hemodynamic impairment.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
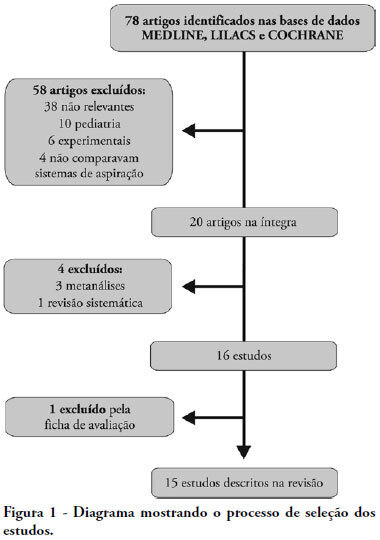
OBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
OBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
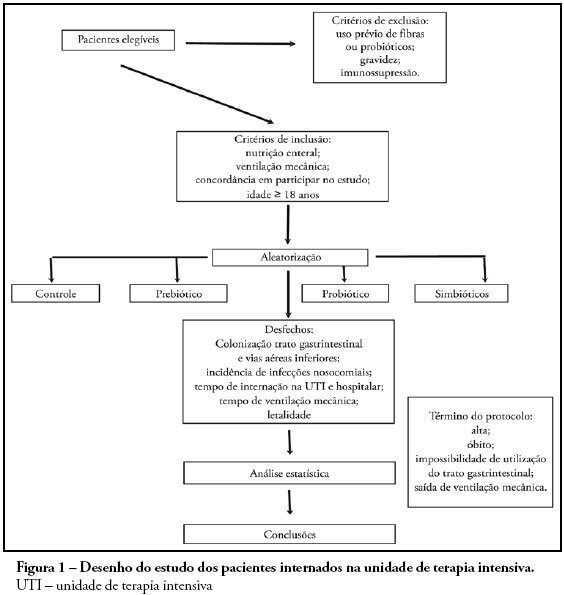
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)