
You searched for:"Pedro Póvoa"
We found (19) results for your search.-
Original Article
Delirium severity and outcomes of critically ill COVID-19 patients
- Luciana Leal do Rego
 ,
, - Jorge Ibrain Figueira Salluh ,
- Vicente Cés de Souza-Dantas ,
- José Roberto Lapa e Silva ,
- Pedro Póvoa , [ … ],
- Rodrigo Bernardo Serafim
Abstract
Original ArticleDelirium severity and outcomes of critically ill COVID-19 patients
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
- Luciana Leal do Rego ,
- Jorge Ibrain Figueira Salluh ,
- Vicente Cés de Souza-Dantas ,
- José Roberto Lapa e Silva ,
- Pedro Póvoa ,
- Rodrigo Bernardo Serafim
Views10ABSTRACT
Objective:
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
Methods:
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Results:
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 – 25] versus 6 [4 – 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 – 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 – 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
Conclusion:
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Keywords:Coronavirus infectionsCOVID-19Critical care outcomesCritical illnessDeliriumIntensive care unitsPrognosisPsychiatric status rating scalesrisk factorsSurveys and questionnairesSee moreViews10

Abstract
Original ArticleDelirium severity and outcomes of critically ill COVID-19 patients
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
- Luciana Leal do Rego ,
- Jorge Ibrain Figueira Salluh ,
- Vicente Cés de Souza-Dantas ,
- José Roberto Lapa e Silva ,
- Pedro Póvoa ,
- Rodrigo Bernardo Serafim
Views10ABSTRACT
Objective:
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
Methods:
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Results:
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 – 25] versus 6 [4 – 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 – 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 – 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
Conclusion:
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Keywords:Coronavirus infectionsCOVID-19Critical care outcomesCritical illnessDeliriumIntensive care unitsPrognosisPsychiatric status rating scalesrisk factorsSurveys and questionnairesSee more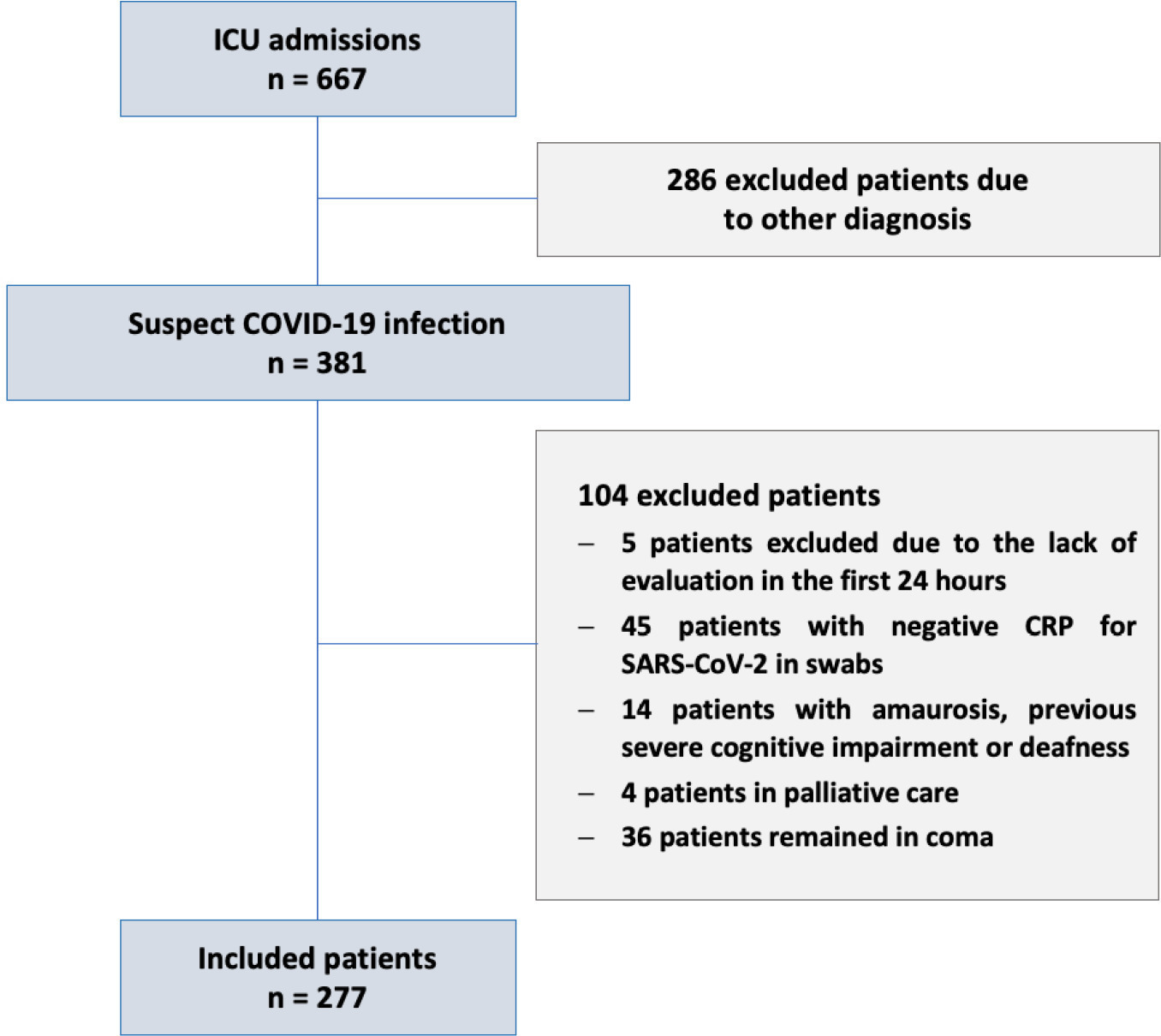
- Luciana Leal do Rego
-
Original Article
What changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
- Rui Antunes Pereira ,
- Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes , [ … ],
- Susana Mendes Fernandes
Abstract
Original ArticleWhat changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
- Rui Antunes Pereira ,
- Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes ,
- Sara Ventura ,
- Irene Aragão ,
- Raul Miguel de Freitas Lima Neto ,
- Elena Molinos ,
- Ana Marques ,
- Nelson Cardoso ,
- Flávio Marino ,
- Filipa Brás Monteiro ,
- Ana Pinho Oliveira ,
- Rogério C Silva ,
- André Miguel Neto Real ,
- Bruno Sarmento Banheiro ,
- Renato Reis ,
- Maria Adão-Serrano ,
- Ana Cracium ,
- Ana Valadas ,
- João Miguel Ribeiro ,
- Pedro Póvoa ,
- Camila Tapadinhas ,
- Vítor Mendes ,
- Luís Coelho ,
- Raquel Maia ,
- Paulo Telles Freitas ,
- Isabel Amorim Ferreira ,
- Tiago Ramires ,
- Luís Silva Val-Flores ,
- Mariana Cascão ,
- Rita Alves ,
- Simão C Rodeia ,
- Cleide Barrigoto ,
- Rosa Cardiga ,
- Maria João Ferreira da Silva ,
- Bruno Vale ,
- Tatiana Fonseca ,
- Ana Lúcia Rios,
- João Camões ,
- Danay Pérez,
- Susana Cabral ,
- Maria Inês Ribeiro,
- João João Mendes ,
- João Gouveia ,
- Susana Mendes Fernandes
Views1ABSTRACT
Objective:
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
Methods:
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 – 16 and 17 – 34, were defined.
Results:
Five hundred forty-one adult patients with a median age of 65 [57 – 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 – 3] versus 2 [0 – 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
Conclusion:
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Keywords:acute respiratory distress syndromeAdrenal cortex hormonesCoronavirus infectionsCOVID-19Critical care outcomesCritical illnessIntensive carePandemicsSARS-CoV-2See moreViews1Abstract
Original ArticleWhat changed between the peak and plateau periods of the first COVID-19 pandemic wave? A multicentric Portuguese cohort study in intensive care
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
- Rui Antunes Pereira ,
- Marta Sousa ,
- José Pedro Cidade ,
- Luís Melo ,
- Diogo Lopes ,
- Sara Ventura ,
- Irene Aragão ,
- Raul Miguel de Freitas Lima Neto ,
- Elena Molinos ,
- Ana Marques ,
- Nelson Cardoso ,
- Flávio Marino ,
- Filipa Brás Monteiro ,
- Ana Pinho Oliveira ,
- Rogério C Silva ,
- André Miguel Neto Real ,
- Bruno Sarmento Banheiro ,
- Renato Reis ,
- Maria Adão-Serrano ,
- Ana Cracium ,
- Ana Valadas ,
- João Miguel Ribeiro ,
- Pedro Póvoa ,
- Camila Tapadinhas ,
- Vítor Mendes ,
- Luís Coelho ,
- Raquel Maia ,
- Paulo Telles Freitas ,
- Isabel Amorim Ferreira ,
- Tiago Ramires ,
- Luís Silva Val-Flores ,
- Mariana Cascão ,
- Rita Alves ,
- Simão C Rodeia ,
- Cleide Barrigoto ,
- Rosa Cardiga ,
- Maria João Ferreira da Silva ,
- Bruno Vale ,
- Tatiana Fonseca ,
- Ana Lúcia Rios,
- João Camões ,
- Danay Pérez,
- Susana Cabral ,
- Maria Inês Ribeiro,
- João João Mendes ,
- João Gouveia ,
- Susana Mendes Fernandes
Views1ABSTRACT
Objective:
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
Methods:
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 – 16 and 17 – 34, were defined.
Results:
Five hundred forty-one adult patients with a median age of 65 [57 – 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 – 3] versus 2 [0 – 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
Conclusion:
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Keywords:acute respiratory distress syndromeAdrenal cortex hormonesCoronavirus infectionsCOVID-19Critical care outcomesCritical illnessIntensive carePandemicsSARS-CoV-2See more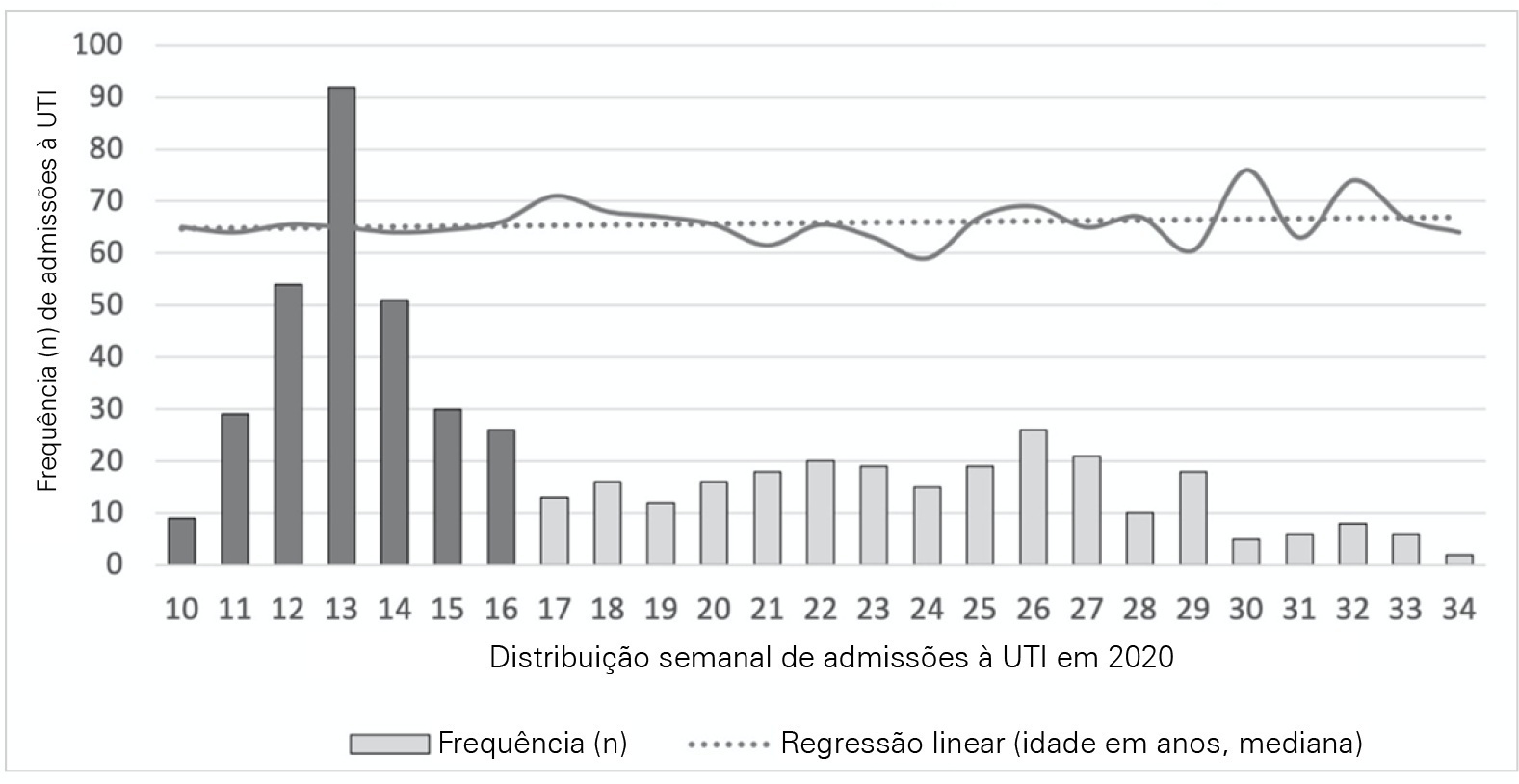
- Rui Antunes Pereira
-
Original Article
Robust, maintainable, emergency invasive mechanical ventilator
- Paulo J. R. Fonte ,
- Alberto Martinho ,
- Américo Pereira,
- Andreia Gomes ,
- Ângela Neves , [ … ],
- Telmo G. Santos
Abstract
Original ArticleRobust, maintainable, emergency invasive mechanical ventilator
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
- Paulo J. R. Fonte ,
- Alberto Martinho ,
- Américo Pereira,
- Andreia Gomes ,
- Ângela Neves ,
- Antero Abrunhosa ,
- António Bugalho ,
- António Gabriel-Santos ,
- António Grilo ,
- Carlos Carmo,
- Elsa Maltez ,
- João Agostinho do Nascimento ,
- João Goes ,
- João Martins ,
- João Pedro Oliveira ,
- Jorge Pimenta ,
- José Paulo Santos ,
- Luís C. Gil ,
- Luís Lopes ,
- Mário Pimenta ,
- Olga Moreira ,
- Orlando Cunha ,
- Pedro Pinheiro de Sousa,
- Pedro Póvoa ,
- Sandra Cavaco-Gonçalves ,
- Susana Barroso ,
- Telmo G. Santos
Views1ABSTRACT
Objective:
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
Methods:
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
Results:
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
Conclusion:
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.
Keywords:AnimalsContinuous positive airway pressureGasesmechanicalOxygenPulmonary VentilationRespiratory rateventilatorsVolatile organic compoundsSee moreViews1Abstract
Original ArticleRobust, maintainable, emergency invasive mechanical ventilator
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
- Paulo J. R. Fonte ,
- Alberto Martinho ,
- Américo Pereira,
- Andreia Gomes ,
- Ângela Neves ,
- Antero Abrunhosa ,
- António Bugalho ,
- António Gabriel-Santos ,
- António Grilo ,
- Carlos Carmo,
- Elsa Maltez ,
- João Agostinho do Nascimento ,
- João Goes ,
- João Martins ,
- João Pedro Oliveira ,
- Jorge Pimenta ,
- José Paulo Santos ,
- Luís C. Gil ,
- Luís Lopes ,
- Mário Pimenta ,
- Olga Moreira ,
- Orlando Cunha ,
- Pedro Pinheiro de Sousa,
- Pedro Póvoa ,
- Sandra Cavaco-Gonçalves ,
- Susana Barroso ,
- Telmo G. Santos
Views1ABSTRACT
Objective:
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
Methods:
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
Results:
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
Conclusion:
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.
Keywords:AnimalsContinuous positive airway pressureGasesmechanicalOxygenPulmonary VentilationRespiratory rateventilatorsVolatile organic compoundsSee more
- Paulo J. R. Fonte
-
Original Article
Sedation, analgesia, and delirium management in Portugal: a survey and point prevalence study
- Maria Carolina Paulino ,
- Isabel Jesus Pereira ,
- Vasco Costa ,
- Aida Neves ,
- Anabela Santos, [ … ],
- Cristina Granja
Abstract
Original ArticleSedation, analgesia, and delirium management in Portugal: a survey and point prevalence study
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
- Maria Carolina Paulino ,
- Isabel Jesus Pereira ,
- Vasco Costa ,
- Aida Neves ,
- Anabela Santos,
- Carla Margarida Teixeira ,
- Isabel Coimbra ,
- Paula Fernandes ,
- Ricardo Bernardo,
- Pedro Póvoa,
- Cristina Granja
Views3See moreABSTRACT
Objective:
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
Methods:
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
Results:
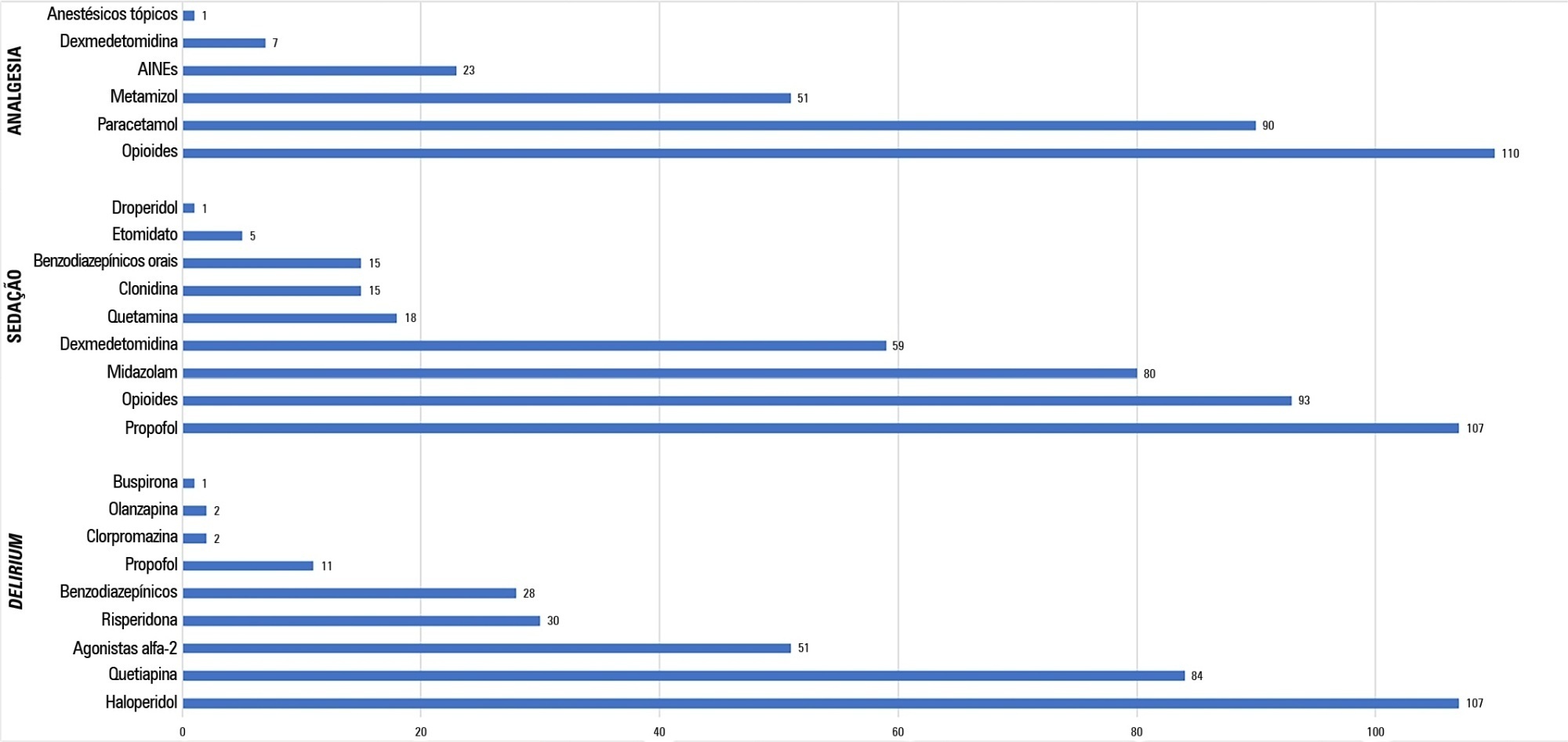
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
Conclusion:
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Views3Abstract
Original ArticleSedation, analgesia, and delirium management in Portugal: a survey and point prevalence study
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
- Maria Carolina Paulino ,
- Isabel Jesus Pereira ,
- Vasco Costa ,
- Aida Neves ,
- Anabela Santos,
- Carla Margarida Teixeira ,
- Isabel Coimbra ,
- Paula Fernandes ,
- Ricardo Bernardo,
- Pedro Póvoa,
- Cristina Granja
Views3See moreABSTRACT
Objective:
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
Methods:
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
Results:
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
Conclusion:
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
- Maria Carolina Paulino
-
Commentary
What every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
Abstract
CommentaryWhat every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
DOI 10.5935/0103-507X.20200004
Views0IntroductionSeveral studies have described the negative outcomes associated with delirium in the short or long term,(,) but not every form of delirium has the same prognosis. The duration and severity of delirium have been found to be the main factors associated with worse outcomes.(,) In fact, a very short delirium duration seems to have little […]See moreViews0Abstract
CommentaryWhat every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
DOI 10.5935/0103-507X.20200004
Views0IntroductionSeveral studies have described the negative outcomes associated with delirium in the short or long term,(,) but not every form of delirium has the same prognosis. The duration and severity of delirium have been found to be the main factors associated with worse outcomes.(,) In fact, a very short delirium duration seems to have little […]See more -
Review Articles
Ventilator-associated tracheobronchitis: an update
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello, [ … ],
- Pedro Póvoa
Abstract
Review ArticlesVentilator-associated tracheobronchitis: an update
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello,
- Saad Nseir ,
- Pedro Póvoa
Views0ABSTRACT
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Keywords:Critical careHealthcare-associated pneumoniaMortalityNosocomial infectionPneumoniaPneumonia, ventilator-associatedVentilator-associated tracheobronchitisSee moreViews0Abstract
Review ArticlesVentilator-associated tracheobronchitis: an update
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello,
- Saad Nseir ,
- Pedro Póvoa
Views0ABSTRACT
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Keywords:Critical careHealthcare-associated pneumoniaMortalityNosocomial infectionPneumoniaPneumonia, ventilator-associatedVentilator-associated tracheobronchitisSee more -
Original Article
suPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Views0Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
-
Commentaries
Dear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
Abstract
CommentariesDear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Views0The controversyThe medical community became divided over the clinical value of the new criteria (i.e., regarding their actual impact and safety when applied at the bedside). The criticism mainly focused on the following three aspects: (1) underlying theoretical concepts; (2) the methods used to define the criteria; and (3) their potential impacts on clinical practice.Regarding […]See moreViews0Abstract
CommentariesDear Sepsis-3, we are sorry to say that we don’t like you
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Views0The controversyThe medical community became divided over the clinical value of the new criteria (i.e., regarding their actual impact and safety when applied at the bedside). The criticism mainly focused on the following three aspects: (1) underlying theoretical concepts; (2) the methods used to define the criteria; and (3) their potential impacts on clinical practice.Regarding […]See more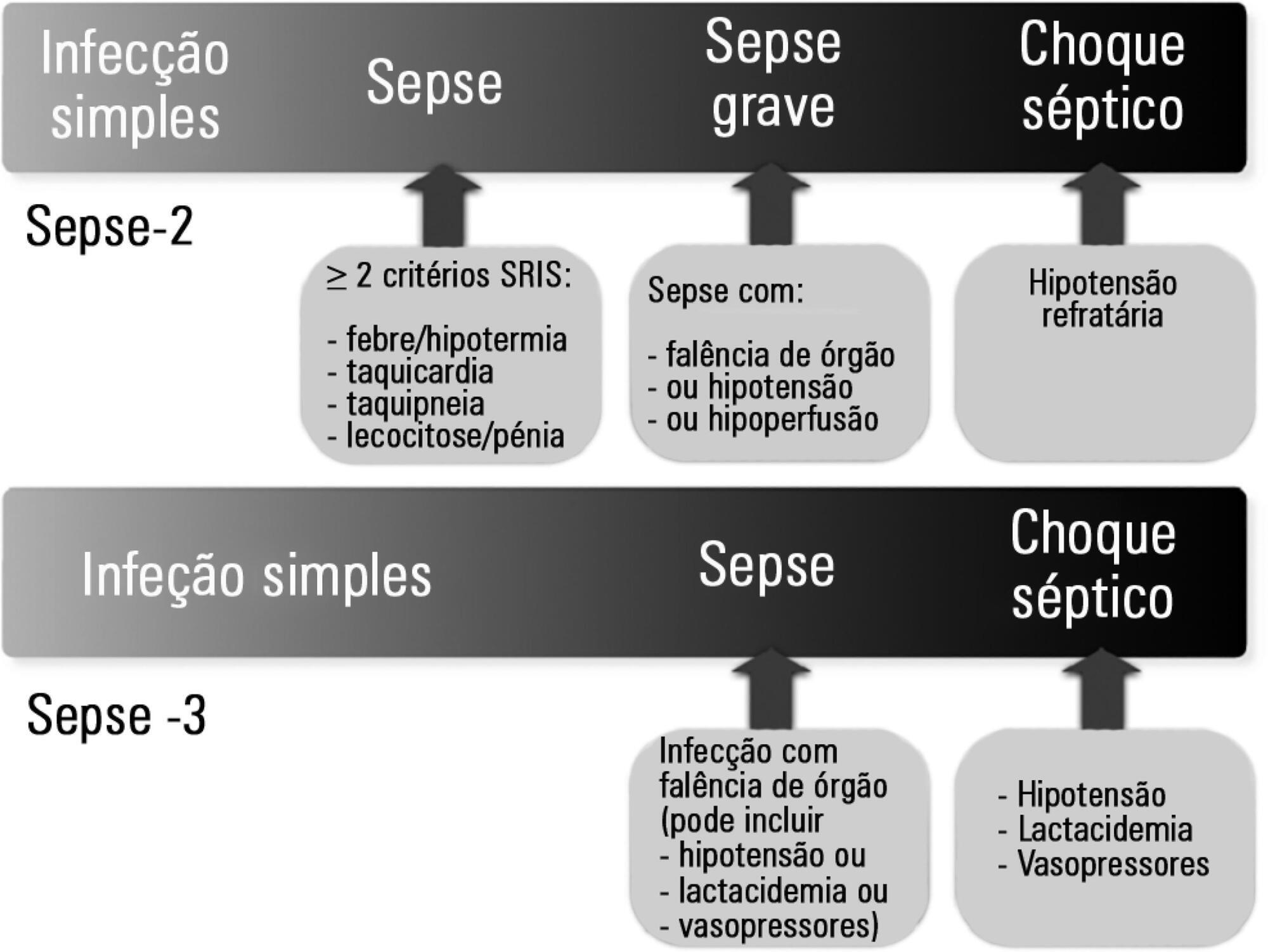
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis