analgesia Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
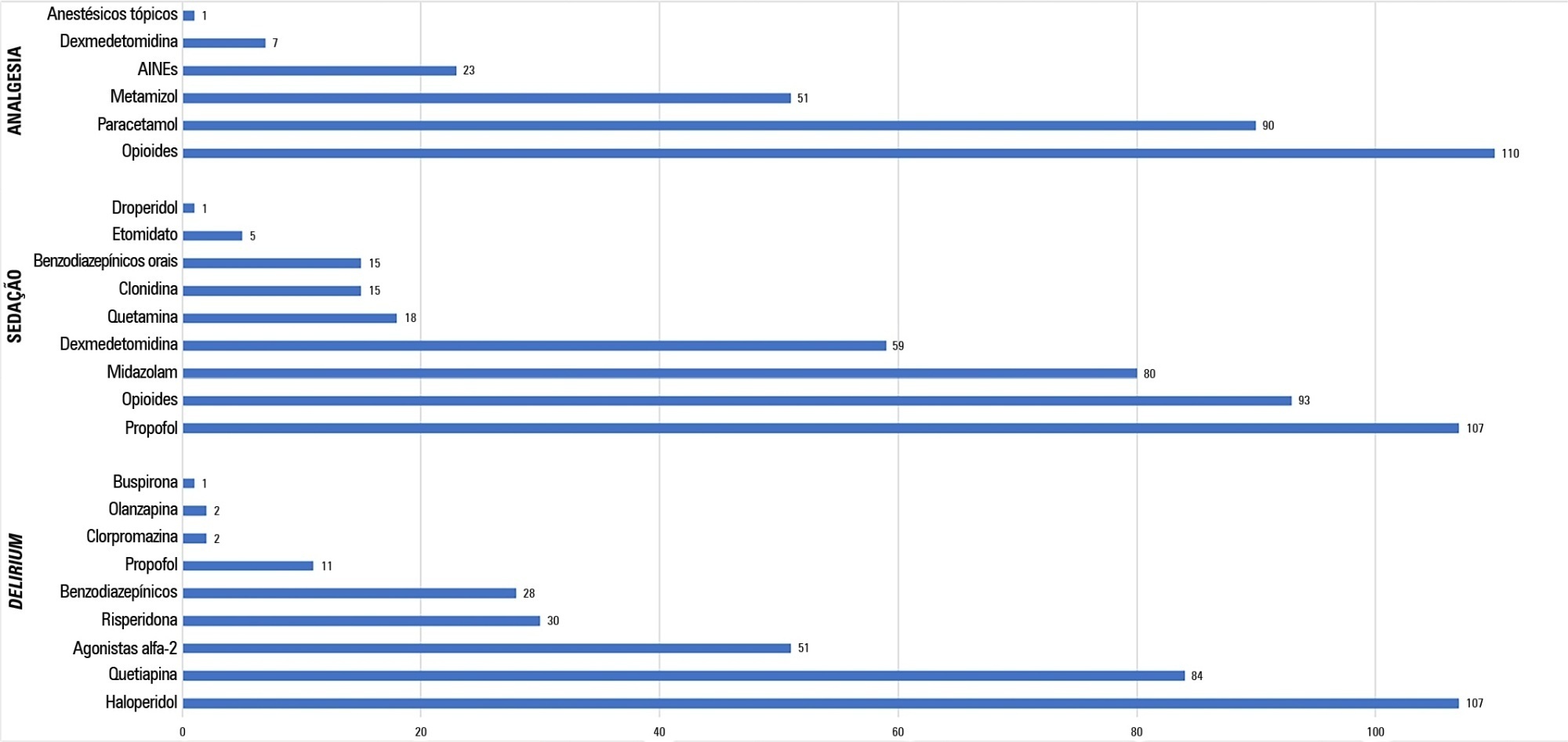
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):227-236
DOI 10.5935/0103-507X.20220020-en
To establish current Portuguese critical care practices regarding analgesia, sedation, and delirium based on a comparison between the activities reported and daily clinical practice.
A national survey was conducted among physicians invited to report their practice toward analgesia, sedation, and delirium in intensive care units. A point prevalence study was performed to analyze daily practices.
A total of 117 physicians answered the survey, and 192 patients were included in the point prevalence study. Survey and point prevalence studies reflect a high sedation assessment (92%; 88.5%), with the Richmond Agitated Sedation Scale being the most reported and used scale (41.7%; 58.2%) and propofol being the most reported and used medication (91.4%; 58.6%). Midazolam prescribing was reported by 68.4% of responders, but a point prevalence study revealed a use of 27.6%.
The results from the survey did not accurately reflect the common practices in Portuguese intensive care units, as reported in the point prevalence study. Efforts should be made specifically to avoid oversedation and to promote delirium assessment.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):48-67
DOI 10.5935/0103-507X.20210005
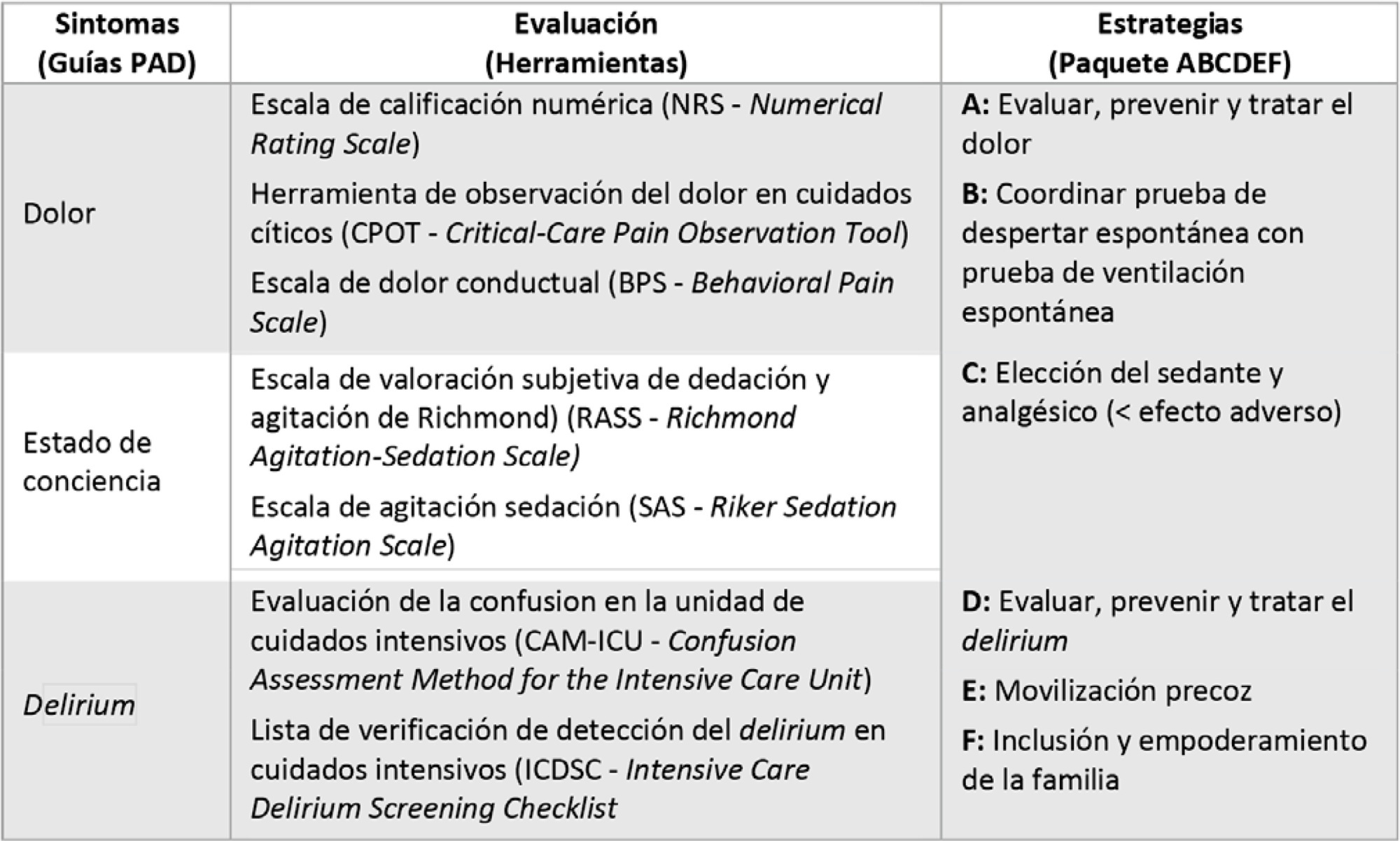
To propose agile strategies for a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for patients with COVID-19-associated acute respiratory distress syndrome, considering the high risk of infection among health workers, the humanitarian treatment that we must provide to patients and the inclusion of patients’ families, in a context lacking specific therapeutic strategies against the virus globally available to date and a potential lack of health resources.
A nonsystematic review of the scientific evidence in the main bibliographic databases was carried out, together with national and international clinical experience and judgment. Finally, a consensus of recommendations was made among the members of the Committee for Analgesia, Sedation and Delirium of the Sociedad Argentina de Terapia Intensiva.
Recommendations were agreed upon, and tools were developed to ensure a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for adult patients with acute respiratory distress syndrome due to COVID-19.
Given the new order generated in intensive therapies due to the advancing COVID-19 pandemic, we propose to not leave aside the usual good practices but to adapt them to the particular context generated. Our consensus is supported by scientific evidence and national and international experience and will be an attractive consultation tool in intensive therapies.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):48-67
DOI 10.5935/0103-507X.20210005
To propose agile strategies for a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for patients with COVID-19-associated acute respiratory distress syndrome, considering the high risk of infection among health workers, the humanitarian treatment that we must provide to patients and the inclusion of patients’ families, in a context lacking specific therapeutic strategies against the virus globally available to date and a potential lack of health resources.
A nonsystematic review of the scientific evidence in the main bibliographic databases was carried out, together with national and international clinical experience and judgment. Finally, a consensus of recommendations was made among the members of the Committee for Analgesia, Sedation and Delirium of the Sociedad Argentina de Terapia Intensiva.
Recommendations were agreed upon, and tools were developed to ensure a comprehensive approach to analgesia, sedation, delirium, early mobility and family engagement for adult patients with acute respiratory distress syndrome due to COVID-19.
Given the new order generated in intensive therapies due to the advancing COVID-19 pandemic, we propose to not leave aside the usual good practices but to adapt them to the particular context generated. Our consensus is supported by scientific evidence and national and international experience and will be an attractive consultation tool in intensive therapies.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):21-26
DOI 10.5935/0103-507X.20190007
This study sought to describe and quantify the pharmacological and nonpharmacological strategies used to relieve the pain/stress of neonates during hospitalization in neonatal intensive care units.
This quantitative, longitudinal, and descriptive study examined 50 neonates from neonatal intensive care unit admission to discharge.
A total of 9,948 painful/stressful procedures were recorded (mean = 11.25 ± 6.3) per day per neonate. A total of 11,722 pain-management and relief interventions were performed, of which 11,495 (98.1%) were nonpharmacological strategies, and 227 (1.9%) were pharmacological interventions. On average, each neonate received 235 pain-management and treatment interventions during hospitalization, 13 nonpharmacological interventions per day, and one pharmacological intervention every 2 days.
Neonates receive few specific measures for pain relief given the high number of painful and stressful procedures performed during hospitalization. Thus, it is essential to implement effective pain-relief protocols.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):21-26
DOI 10.5935/0103-507X.20190007
This study sought to describe and quantify the pharmacological and nonpharmacological strategies used to relieve the pain/stress of neonates during hospitalization in neonatal intensive care units.
This quantitative, longitudinal, and descriptive study examined 50 neonates from neonatal intensive care unit admission to discharge.
A total of 9,948 painful/stressful procedures were recorded (mean = 11.25 ± 6.3) per day per neonate. A total of 11,722 pain-management and relief interventions were performed, of which 11,495 (98.1%) were nonpharmacological strategies, and 227 (1.9%) were pharmacological interventions. On average, each neonate received 235 pain-management and treatment interventions during hospitalization, 13 nonpharmacological interventions per day, and one pharmacological intervention every 2 days.
Neonates receive few specific measures for pain relief given the high number of painful and stressful procedures performed during hospitalization. Thus, it is essential to implement effective pain-relief protocols.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):337-345
DOI 10.5935/0103-507X.20170058
To establish the prevalence of delirium in a general intensive care unit and to identify associated factors, clinical expression and the influence on outcomes.
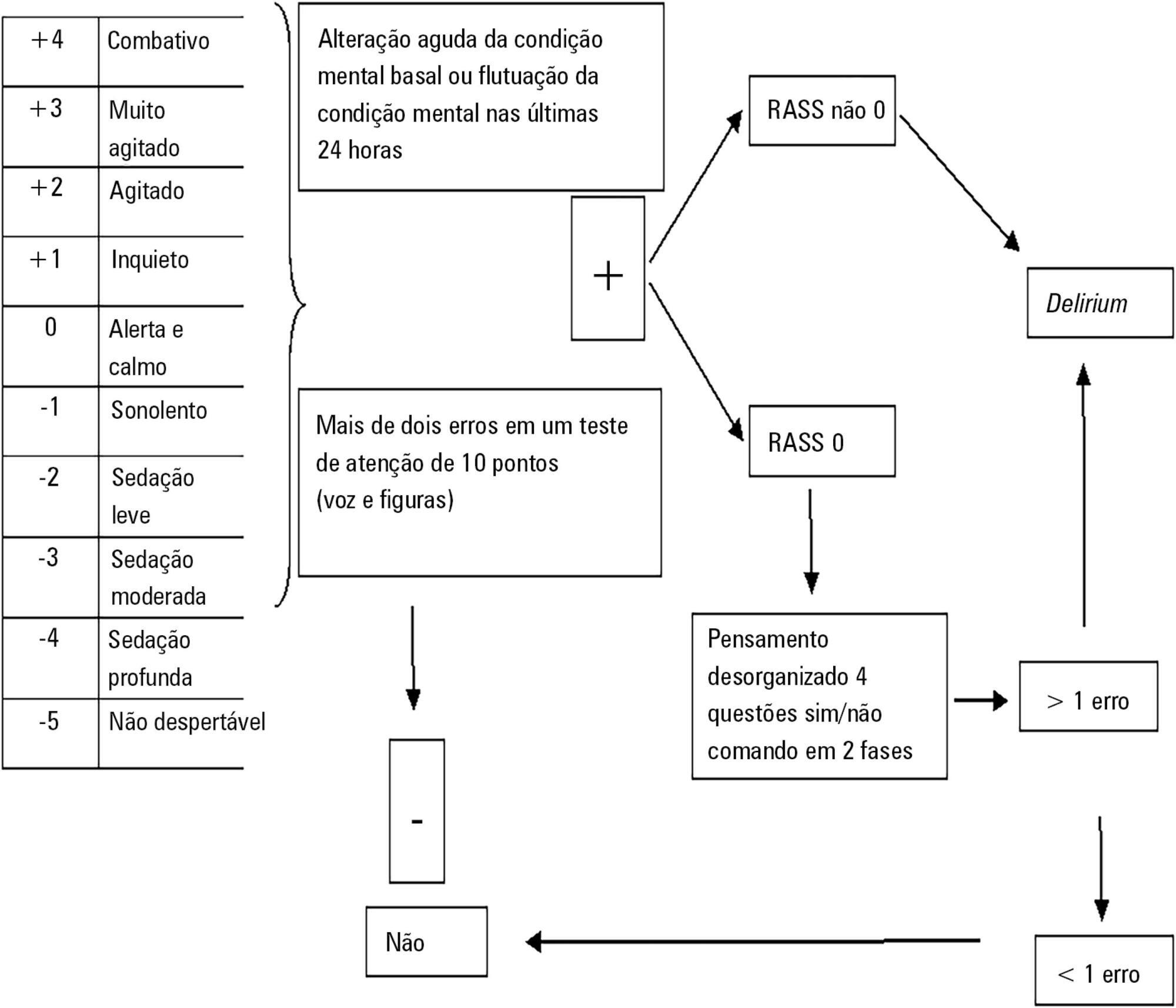
This was a prospective cohort study in a medical surgical intensive care unit. The Richmond Agitation-Sedation Scale and Confusion Assessment Method for the Intensive Care Unit were used daily to identify delirium in mechanically ventilated patients.
In this series, delirium prevalence was 80% (N = 184 delirious patients out of 230 patients). The number of patients according to delirium psychomotor subtypes was as follows: 11 hyperactive patients (6%), 9 hypoactive patients (5%) and 160 mixed patients (89%). Multiple logistic regression modeling using delirium as the dependent outcome variable (to study the risk factors for delirium) revealed that age > 65 years, history of alcohol consumption, and number of mechanical ventilation days were independent variables associated with the development of delirium. The multiple logistic regression model using hospital mortality as the dependent outcome variable (to study the risk factors for death) showed that severity of illness, according to the Acute Physiology and Chronic Health Evaluation II, mechanical ventilation for more than 7 days, and sedation days were all independent predictors for excess hospital mortality.
This Latin American prospective cohort investigation confirmed specific factors important for the development of delirium and the outcome of death among general intensive care unit patients. In both analyses, we found that the duration of mechanical ventilation was a predictor of untoward outcomes.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):337-345
DOI 10.5935/0103-507X.20170058
To establish the prevalence of delirium in a general intensive care unit and to identify associated factors, clinical expression and the influence on outcomes.
This was a prospective cohort study in a medical surgical intensive care unit. The Richmond Agitation-Sedation Scale and Confusion Assessment Method for the Intensive Care Unit were used daily to identify delirium in mechanically ventilated patients.
In this series, delirium prevalence was 80% (N = 184 delirious patients out of 230 patients). The number of patients according to delirium psychomotor subtypes was as follows: 11 hyperactive patients (6%), 9 hypoactive patients (5%) and 160 mixed patients (89%). Multiple logistic regression modeling using delirium as the dependent outcome variable (to study the risk factors for delirium) revealed that age > 65 years, history of alcohol consumption, and number of mechanical ventilation days were independent variables associated with the development of delirium. The multiple logistic regression model using hospital mortality as the dependent outcome variable (to study the risk factors for death) showed that severity of illness, according to the Acute Physiology and Chronic Health Evaluation II, mechanical ventilation for more than 7 days, and sedation days were all independent predictors for excess hospital mortality.
This Latin American prospective cohort investigation confirmed specific factors important for the development of delirium and the outcome of death among general intensive care unit patients. In both analyses, we found that the duration of mechanical ventilation was a predictor of untoward outcomes.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
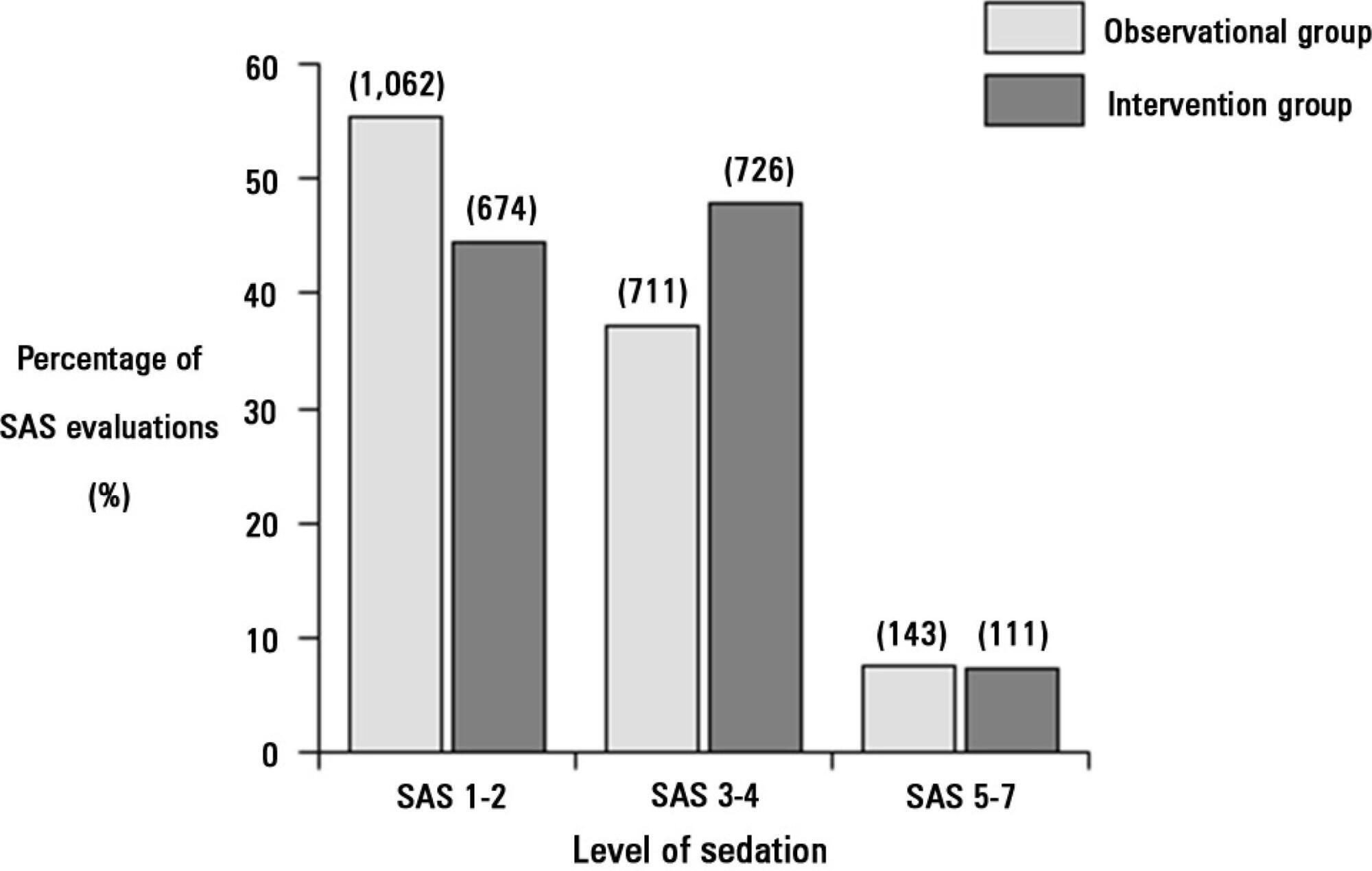
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Although low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units' invasive procedures, therefore contributing to pain reduction
Abstract
Rev Bras Ter Intensiva. 2011;23(3):370-373
DOI 10.1590/S0103-507X2011000300016
Although low-birth neonates are acknowledged to experience pain, many routine procedures continue to be conducted without proper pharmacological or non-pharmacological analgesia. Kangaroo care is a low-cost strategy that can be used in the preterm newborn. Mothers should be encouraged to use this easy-to-perform method, which is feasible both before and during neonatal units' invasive procedures, therefore contributing to pain reduction
Abstract
Rev Bras Ter Intensiva. 2008;20(4):405-410
DOI 10.1590/S0103-507X2008000400014
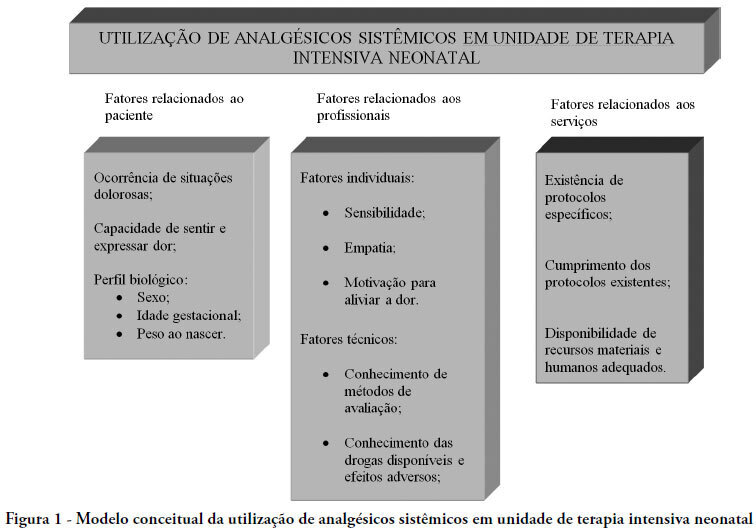
The purpose of this paper was to carry out a review of literature on the history and current stage of the knowledge of systemic analgesia in neonatology and the factors influencing its use. A search for scientific articles was made in the MEDLINE, SciELO and LILACS databases using the keywords: analgesia, systemic analgesics, pain, neonatology, newborn, intensive care units and neonatal intensive care units. Additional research was made on dissertations and thesis databanks as well as text books. Literature consulted disclosed that, in general, analgesia is not a routine practice in neonatal intensive care units, despite the numerous studies demonstrating its importance. Although pain relief is a basic principle of medicine, involving ethic and humanitarian issues and despite the current availability of a number of practical guidelines and consensus regarding pain management in newborns at risk, findings of the present study fall far short of current recommendations. Urgent intervention is required to redress this situation.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):405-410
DOI 10.1590/S0103-507X2008000400014
The purpose of this paper was to carry out a review of literature on the history and current stage of the knowledge of systemic analgesia in neonatology and the factors influencing its use. A search for scientific articles was made in the MEDLINE, SciELO and LILACS databases using the keywords: analgesia, systemic analgesics, pain, neonatology, newborn, intensive care units and neonatal intensive care units. Additional research was made on dissertations and thesis databanks as well as text books. Literature consulted disclosed that, in general, analgesia is not a routine practice in neonatal intensive care units, despite the numerous studies demonstrating its importance. Although pain relief is a basic principle of medicine, involving ethic and humanitarian issues and despite the current availability of a number of practical guidelines and consensus regarding pain management in newborns at risk, findings of the present study fall far short of current recommendations. Urgent intervention is required to redress this situation.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)