Clinical protocols Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
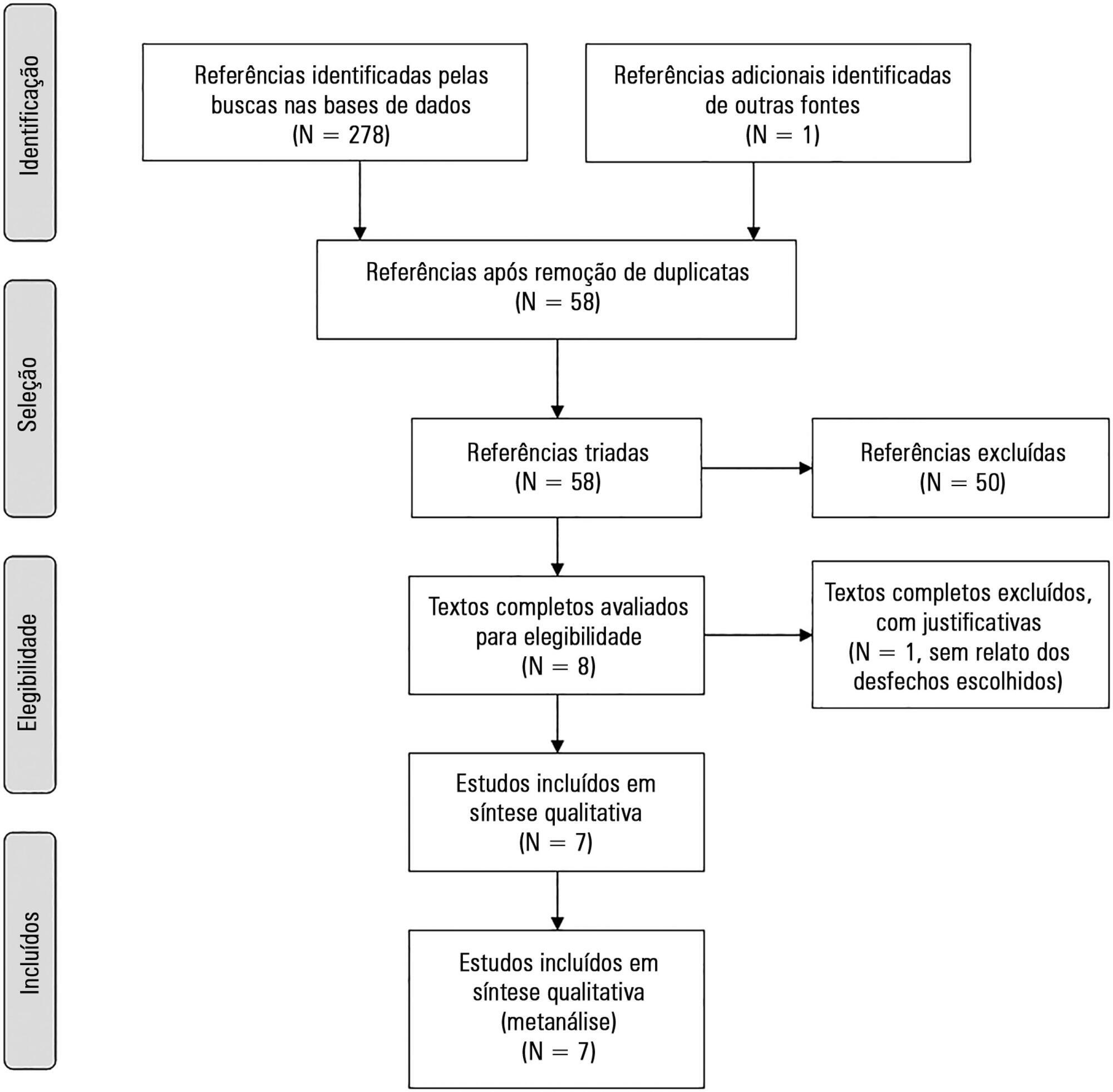
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 - 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 - 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 - -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 - 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 - 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 - -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
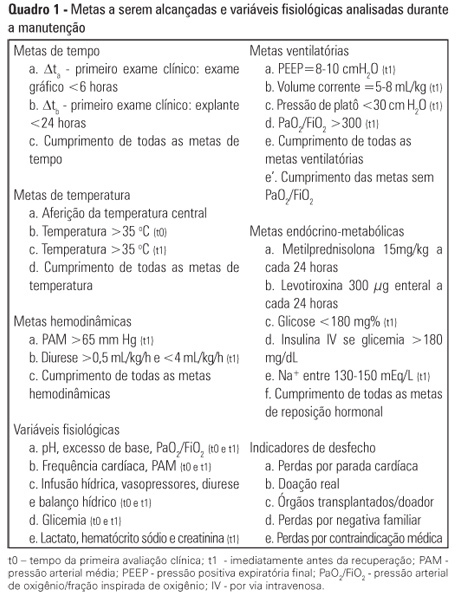
OBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student's t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
OBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student's t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
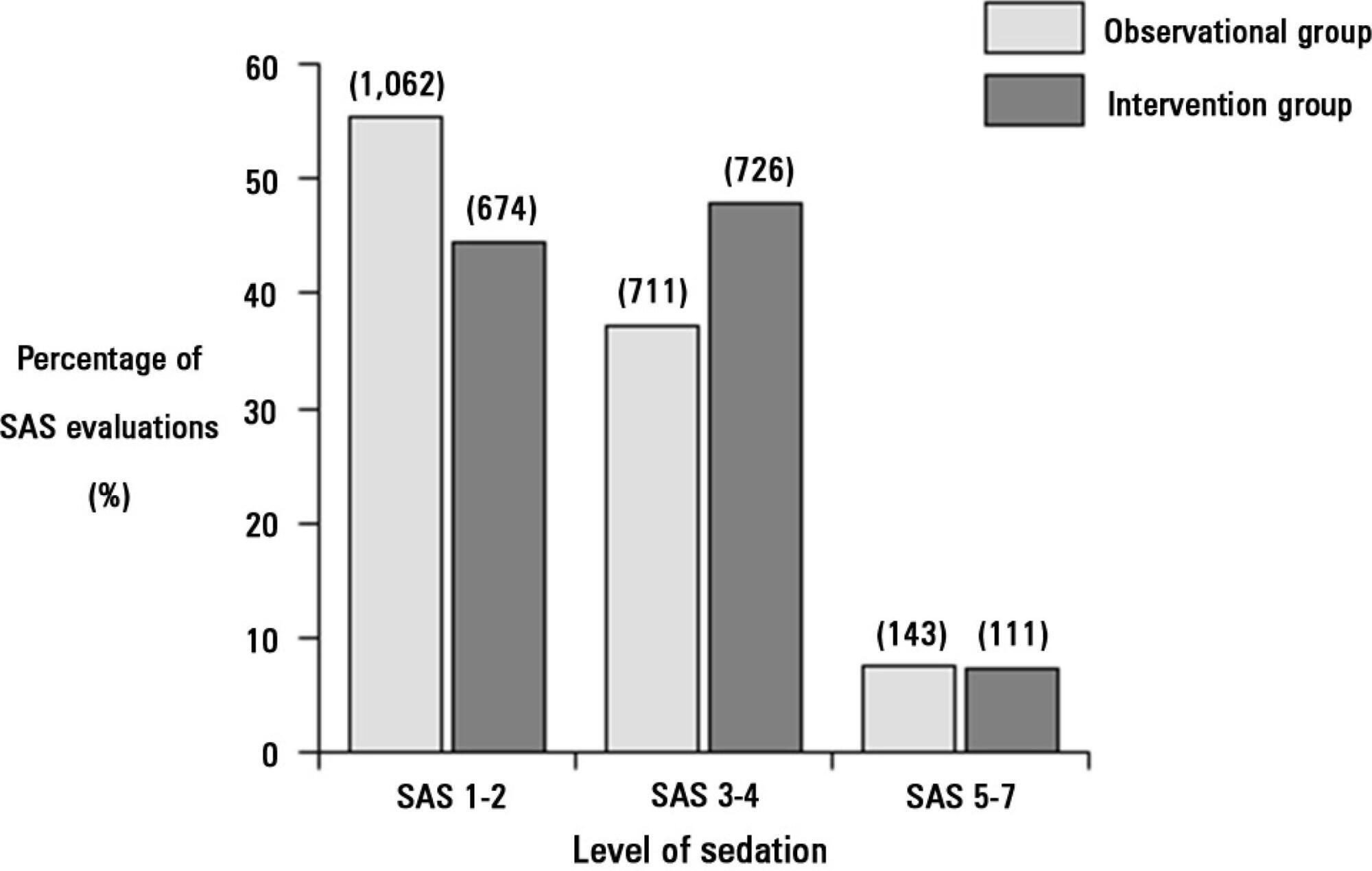
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.