Deep sedation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):164-170
DOI 10.5935/0103-507X.20190028
To evaluate the satisfaction of patients admitted to the intensive care unit using a diary and analyze possible points for improving this instrument.
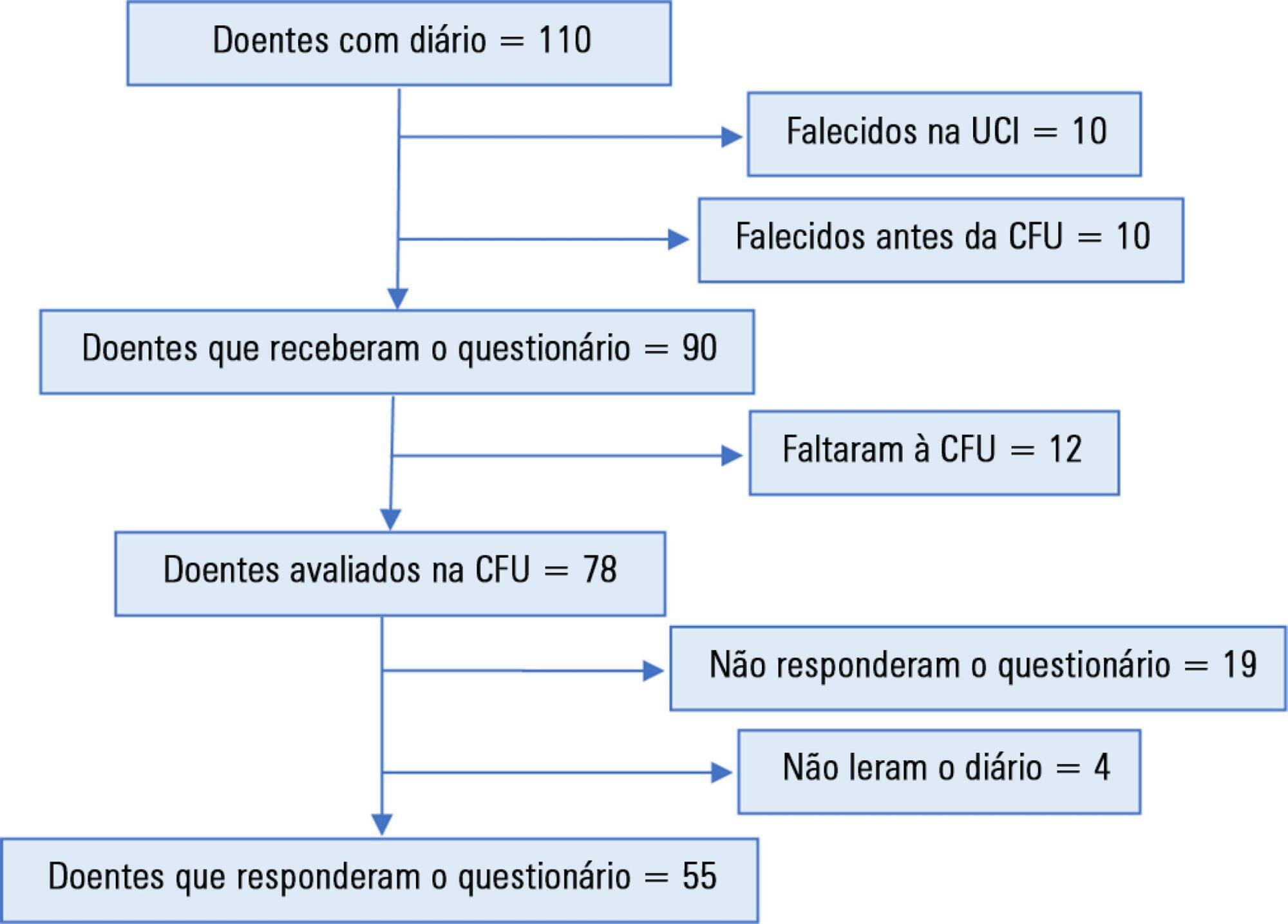
This was an observational, retrospective study, conducted between March 2014 and July 2017, in a multidisciplinary intensive care unit of a district hospital. The diary was implemented in patients sedated for 3 or more days. Three months after discharge, their satisfaction was assessed using a questionnaire. A patient who agreed with the 5 statements assessing the diary's help in clarifying the intensive care unit stay, in filling memory gaps, in recovery, in reassurance, and in the recommendation of this intervention was defined as satisfied.
A total of 110 patients were included, of whom 55 answered the questionnaire. Of these, 36 (65.5%) were classified as satisfied. Each item had a positive response in more than 74% of cases. A total of 60% of the participants suggested increasing the number of photographs. No significant differences were found in the subgroup analysis (age, sex, duration of sedation and ventilation, length of diary keeping, severity on admission, or delirium, depression, or anxiety in the intensive care unit).
Most patients were satisfied with the diary but suggested an increase in the number of photographs.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):164-170
DOI 10.5935/0103-507X.20190028
To evaluate the satisfaction of patients admitted to the intensive care unit using a diary and analyze possible points for improving this instrument.
This was an observational, retrospective study, conducted between March 2014 and July 2017, in a multidisciplinary intensive care unit of a district hospital. The diary was implemented in patients sedated for 3 or more days. Three months after discharge, their satisfaction was assessed using a questionnaire. A patient who agreed with the 5 statements assessing the diary's help in clarifying the intensive care unit stay, in filling memory gaps, in recovery, in reassurance, and in the recommendation of this intervention was defined as satisfied.
A total of 110 patients were included, of whom 55 answered the questionnaire. Of these, 36 (65.5%) were classified as satisfied. Each item had a positive response in more than 74% of cases. A total of 60% of the participants suggested increasing the number of photographs. No significant differences were found in the subgroup analysis (age, sex, duration of sedation and ventilation, length of diary keeping, severity on admission, or delirium, depression, or anxiety in the intensive care unit).
Most patients were satisfied with the diary but suggested an increase in the number of photographs.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
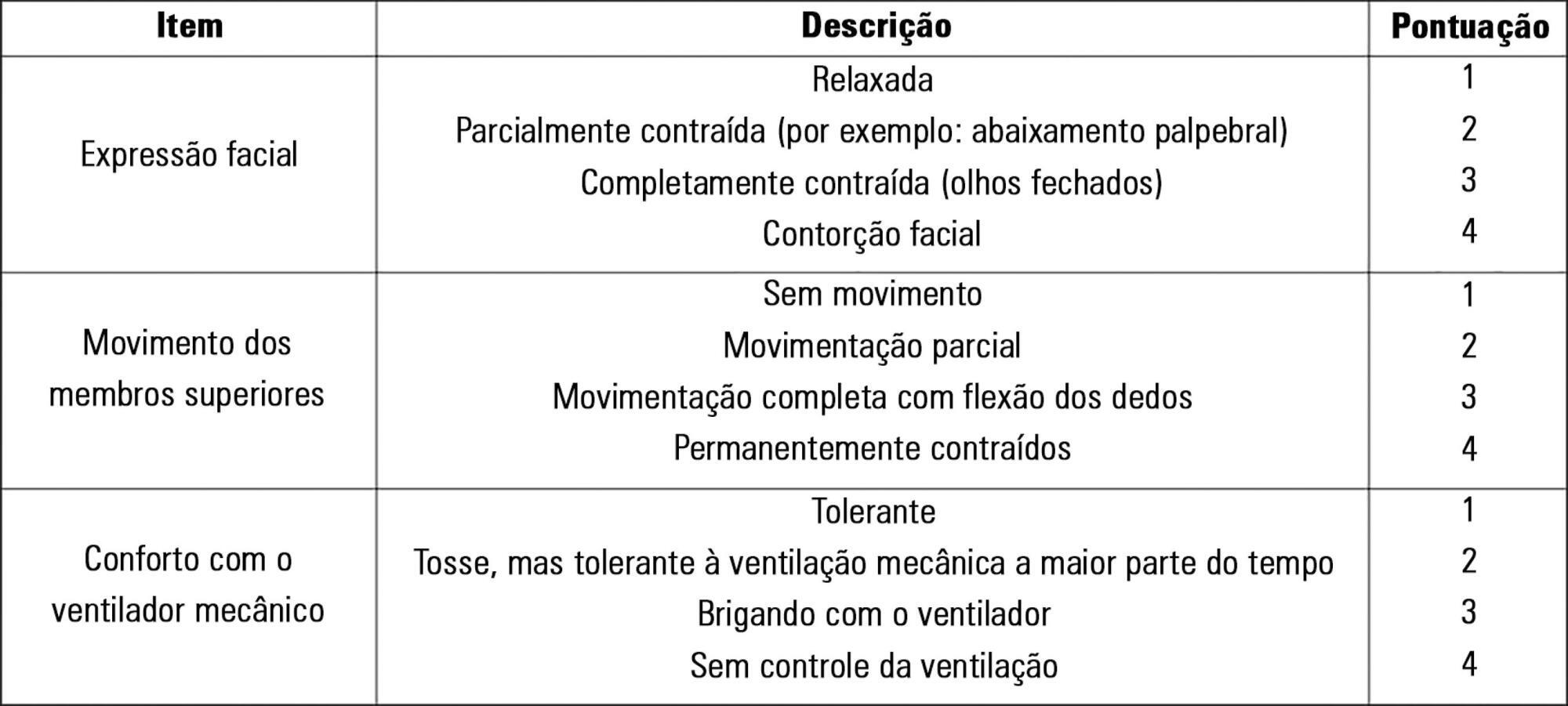
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
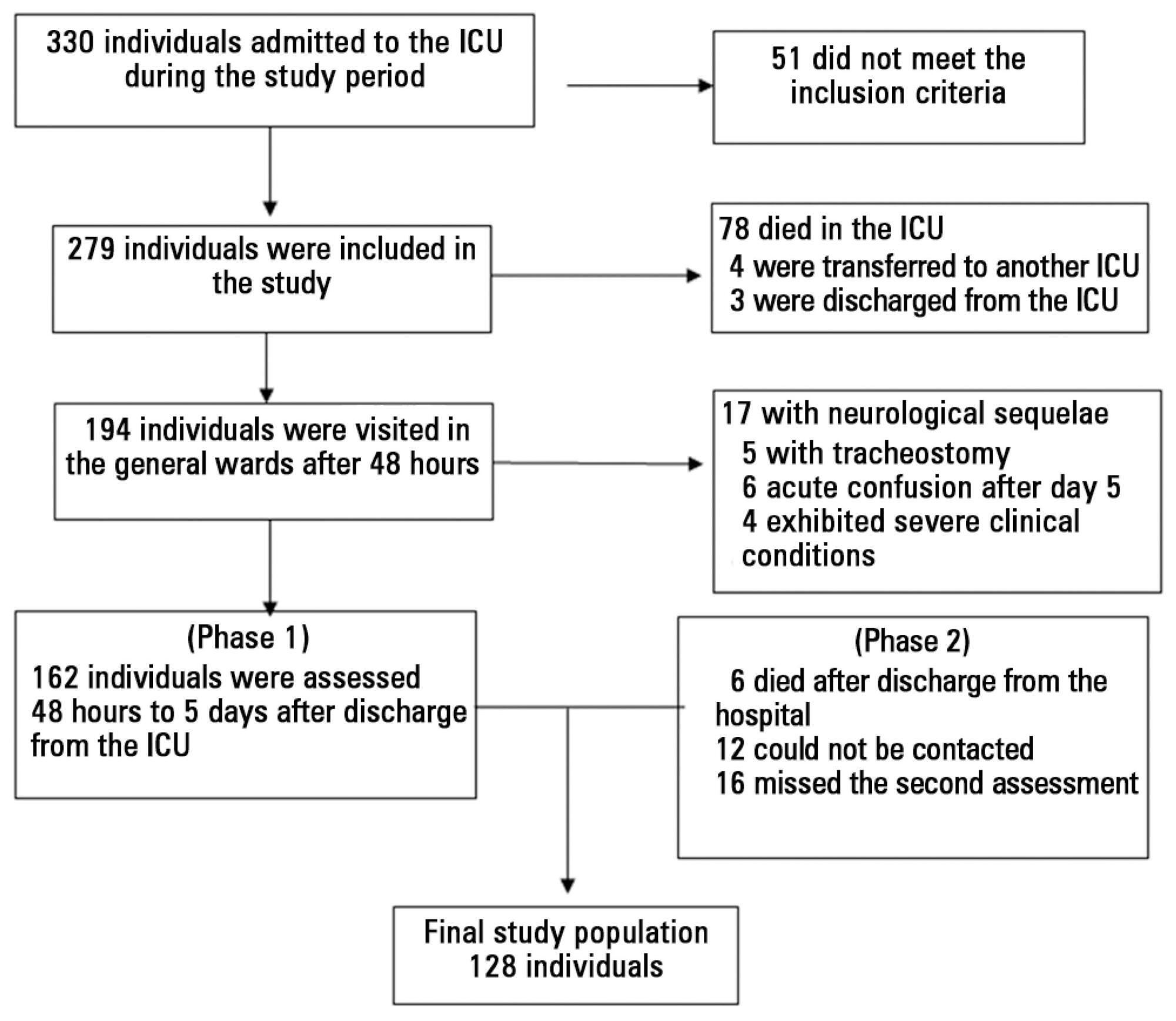
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants' clinical records; the data relative to the participants' memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants' clinical records; the data relative to the participants' memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
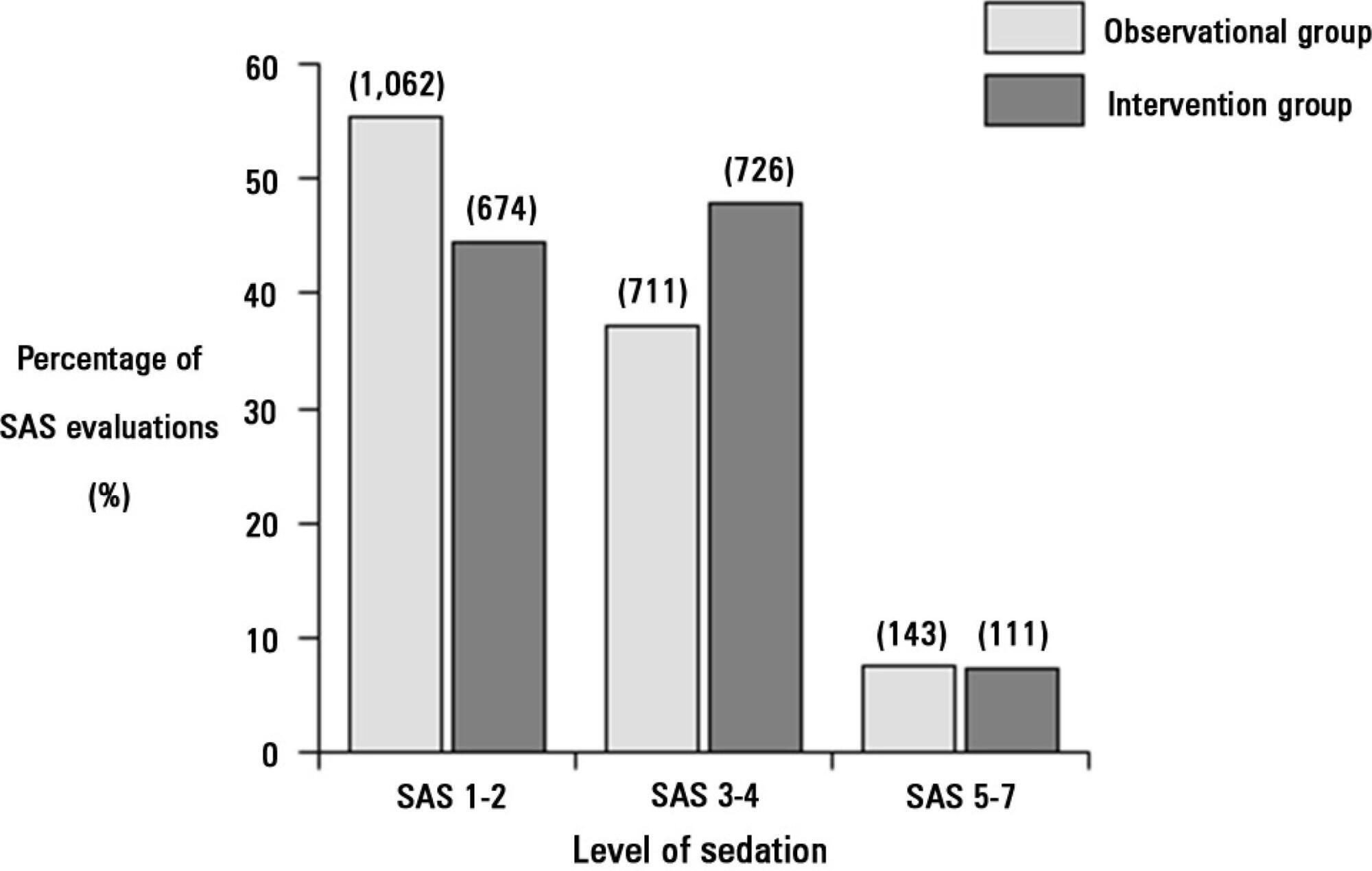
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
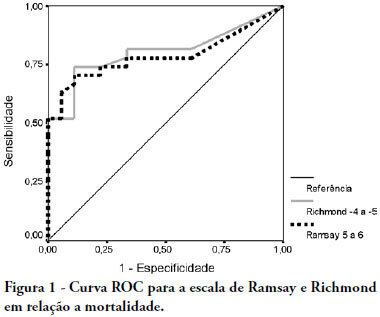
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)