craniocerebral trauma Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
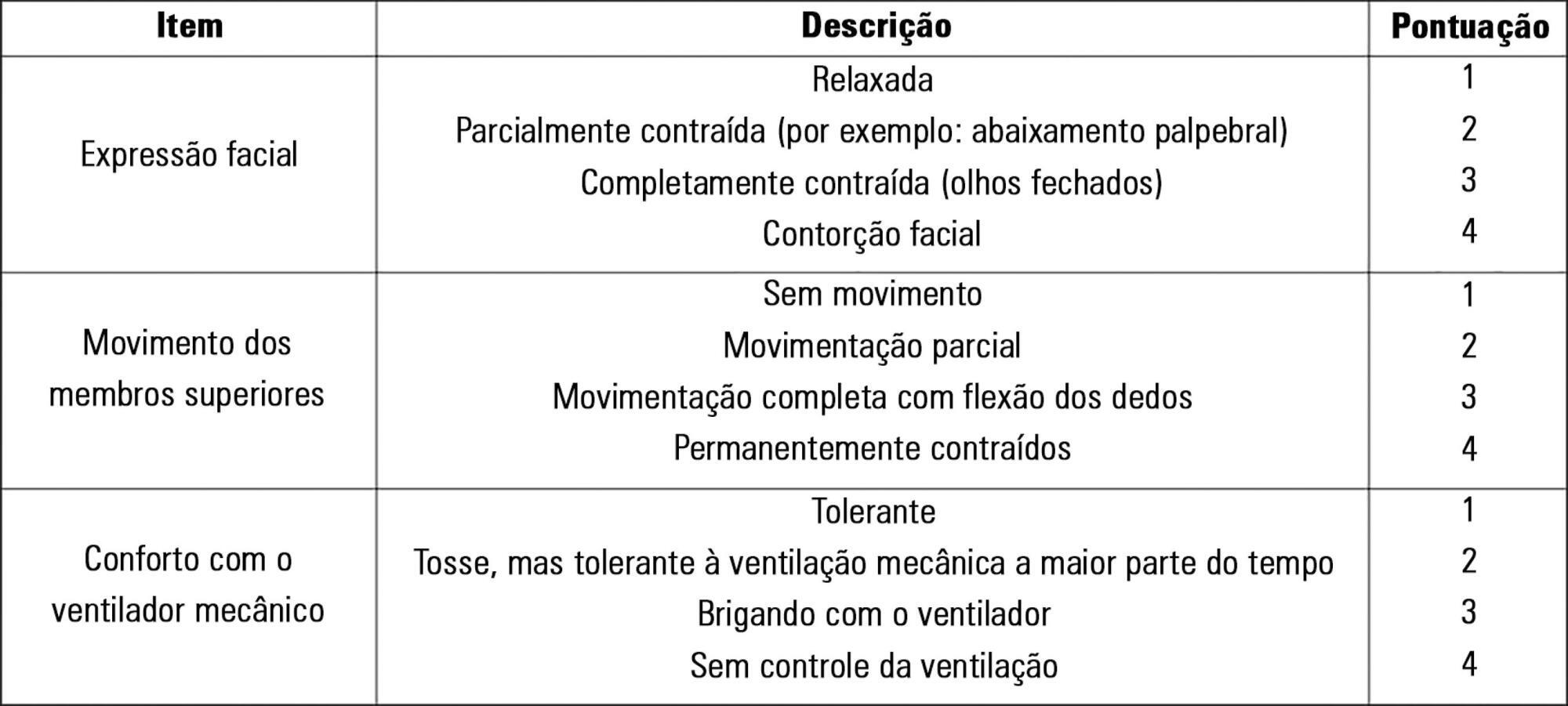
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):148-154
DOI 10.5935/0103-507X.20140022
Patients with traumatic brain injury are particularly susceptible to sepsis, which may exacerbate the systemic inflammatory response and lead to organ dysfunction. The influence of clinical variables on the mortality of intensive care unit patients with traumatic brain injury and sepsis was investigated.
The present investigation was a retrospective study involving 175 patients with traumatic brain injury who were treated in a period of 1 year at a reference hospital for trauma and who had sepsis, severe sepsis, or septic shock. Demographic and clinical data were obtained, and the SOFA score was calculated at the time sepsis was found and after 72 hours.
There was a predominance of young men with severe traumatic brain injury, multiple head injuries, sepsis with a pulmonary focus, prolonged hospital stay, and high mortality (37.7%). Circulatory and respiratory failure had a high incidence, but renal and coagulation failure were less frequent, and liver failure was not observed. After logistic regression, the presence of septic shock and respiratory failure 72 hours after the sepsis diagnosis was associated with higher mortality, with an odds ratio of 7.56 (95%CI=2.04-27.31, p=0.0024) and 6.62 (95%CI=1.93-22.78, p=0.0027), respectively. In addition, there was a higher mortality among patients who had no organ failure on D1 but who developed the condition after 72 hours of sepsis and in those patients who already had organ failure at the time sepsis was diagnosed and remained in this condition after 72 hours.
Septic shock and progressive organ (particularly respiratory) dysfunction increases the mortality of patients with traumatic brain injury and sepsis.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):148-154
DOI 10.5935/0103-507X.20140022
Patients with traumatic brain injury are particularly susceptible to sepsis, which may exacerbate the systemic inflammatory response and lead to organ dysfunction. The influence of clinical variables on the mortality of intensive care unit patients with traumatic brain injury and sepsis was investigated.
The present investigation was a retrospective study involving 175 patients with traumatic brain injury who were treated in a period of 1 year at a reference hospital for trauma and who had sepsis, severe sepsis, or septic shock. Demographic and clinical data were obtained, and the SOFA score was calculated at the time sepsis was found and after 72 hours.
There was a predominance of young men with severe traumatic brain injury, multiple head injuries, sepsis with a pulmonary focus, prolonged hospital stay, and high mortality (37.7%). Circulatory and respiratory failure had a high incidence, but renal and coagulation failure were less frequent, and liver failure was not observed. After logistic regression, the presence of septic shock and respiratory failure 72 hours after the sepsis diagnosis was associated with higher mortality, with an odds ratio of 7.56 (95%CI=2.04-27.31, p=0.0024) and 6.62 (95%CI=1.93-22.78, p=0.0027), respectively. In addition, there was a higher mortality among patients who had no organ failure on D1 but who developed the condition after 72 hours of sepsis and in those patients who already had organ failure at the time sepsis was diagnosed and remained in this condition after 72 hours.
Septic shock and progressive organ (particularly respiratory) dysfunction increases the mortality of patients with traumatic brain injury and sepsis.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
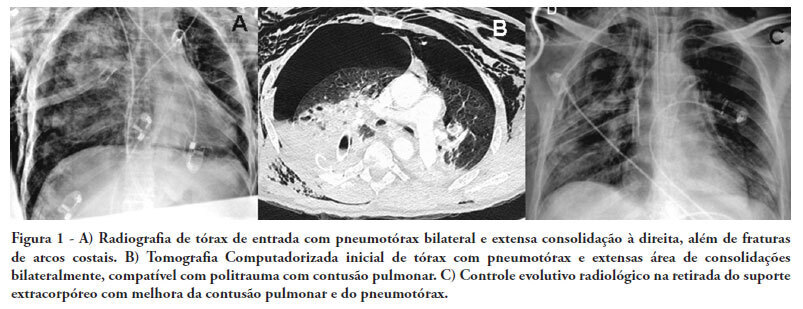
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2009;21(4):343-348
DOI 10.1590/S0103-507X2009000400002
OBJECTIVE: Traumatic brain injury is the major cause of death among individuals between 1-45 years-old. The outcome of traumatic brain injury may be related to brain susceptibility to the injury and genetic factors. Genes that may affect traumatic brain injury outcome are being investigated, however there is still few data concerning the association between genetic polymorphisms and traumatic brain injury outcome. The interleukin-1 beta gene (IL-1B) is one of the most studied genes, because levels of this cytokine are raised after traumatic brain injury and this can affect worsen the prognosis. The aim of this study was to test whether the -31C/T polymorphism, located at the promoter region of the IL-1B gene, is associated with primary short-term outcome (death or intensive care unit discharge) in severe traumatic brain injury patients. METHODS: Were studied 69 patients admitted with severe traumatic brain injury in three hospitals of the metropolitan region of Porto Alegre. The polymorphism was analyzed by polymerase chain reaction, followed by restriction digestion. RESULTS: Severe traumatic brain injury was associated with a 45% mortality rate. No significant differences were observed in the allele and genotype frequencies between patients stratified by traumatic brain injury outcome. CONCLUSION: Our findings suggest that -31C/T IL-1B gene polymorphism have no significant impact on the outcome of patients after acute severe traumatic brain injury.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):343-348
DOI 10.1590/S0103-507X2009000400002
OBJECTIVE: Traumatic brain injury is the major cause of death among individuals between 1-45 years-old. The outcome of traumatic brain injury may be related to brain susceptibility to the injury and genetic factors. Genes that may affect traumatic brain injury outcome are being investigated, however there is still few data concerning the association between genetic polymorphisms and traumatic brain injury outcome. The interleukin-1 beta gene (IL-1B) is one of the most studied genes, because levels of this cytokine are raised after traumatic brain injury and this can affect worsen the prognosis. The aim of this study was to test whether the -31C/T polymorphism, located at the promoter region of the IL-1B gene, is associated with primary short-term outcome (death or intensive care unit discharge) in severe traumatic brain injury patients. METHODS: Were studied 69 patients admitted with severe traumatic brain injury in three hospitals of the metropolitan region of Porto Alegre. The polymorphism was analyzed by polymerase chain reaction, followed by restriction digestion. RESULTS: Severe traumatic brain injury was associated with a 45% mortality rate. No significant differences were observed in the allele and genotype frequencies between patients stratified by traumatic brain injury outcome. CONCLUSION: Our findings suggest that -31C/T IL-1B gene polymorphism have no significant impact on the outcome of patients after acute severe traumatic brain injury.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):98-106
DOI 10.1590/S0103-507X2007000100013
BACKGROUND AND OBJECTIVES: Present a critical review of traumatic brain injury (TBI) in children and adolescents, focusing on severe TBI, the mortality and the factors related with poor outcome. CONTENTS: It was made a systematic review in MEDLINE, SciElo e Lilacs, with the key words: traumatic brain injury, craniocerebral trauma, children and mortality. The most important articles related in the Guidelines of Brain Trauma Foundation (2000 e 2003) were selected too. TBI is one of the most important causes of mortality and morbidity in children and adolescents, and morbidity in children and adolescents. The mortality variation was between 10% and 55%, depending of the patients select criteria, trauma severity and units where the studies were made. The children mortality was, in general, lower than that found in adults and the most important factors related with an increased mortality were: Glasgow Coma Score, hypotension, cerebral swelling and lower cerebral perfusion press. Severe TBI endpoint treatment is to correct the secondary brain lesions related factors. CONCLUSIONS: The factors related with better outcomes in children with severe TBI are still obscures, despite the large number of studies, large numbers of studies. Many of these factors can be avoided or correct by aggressive fluid resuscitation, surgery treatment, monitoration and adequate intensive care.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):98-106
DOI 10.1590/S0103-507X2007000100013
BACKGROUND AND OBJECTIVES: Present a critical review of traumatic brain injury (TBI) in children and adolescents, focusing on severe TBI, the mortality and the factors related with poor outcome. CONTENTS: It was made a systematic review in MEDLINE, SciElo e Lilacs, with the key words: traumatic brain injury, craniocerebral trauma, children and mortality. The most important articles related in the Guidelines of Brain Trauma Foundation (2000 e 2003) were selected too. TBI is one of the most important causes of mortality and morbidity in children and adolescents, and morbidity in children and adolescents. The mortality variation was between 10% and 55%, depending of the patients select criteria, trauma severity and units where the studies were made. The children mortality was, in general, lower than that found in adults and the most important factors related with an increased mortality were: Glasgow Coma Score, hypotension, cerebral swelling and lower cerebral perfusion press. Severe TBI endpoint treatment is to correct the secondary brain lesions related factors. CONCLUSIONS: The factors related with better outcomes in children with severe TBI are still obscures, despite the large number of studies, large numbers of studies. Many of these factors can be avoided or correct by aggressive fluid resuscitation, surgery treatment, monitoration and adequate intensive care.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)