
You searched for:"Luiz Marcelo Sá Malbouisson"
We found (6) results for your search.-
Special Article
High versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
- Rodolpho Augusto de Moura Pedro
 ,
, - Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade, [ … ],
- Luíz Marcelo Sá Malbouisson
Abstract
Special ArticleHigh versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
- Rodolpho Augusto de Moura Pedro ,
- Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade,
- Wellington Andraus ,
- Luís Augusto Carneiro D’Albuquerque ,
- Luíz Marcelo Sá Malbouisson
Views13ABSTRACT
Objective:
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
Methods:
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 – 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 – 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
Conclusion:
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Keywords:Arterial pressureHemodynamicsLiver transplantationPerioperative carePostoperative periodRenal insufficiencySee moreViews13

Abstract
Special ArticleHigh versus low mean arterial pressure target in liver transplant patients. An open, controlled, single-center, randomized clinical trial – Protocol and methods (LIVER-PAM)
Crit Care Sci. 2023;35(1):11-18
DOI 10.5935/2965-2774.20230336-pt
- Rodolpho Augusto de Moura Pedro ,
- Bruna Carla Scharranch,
- Lucas de Oliveira Araújo ,
- Luciana Severo Brandão,
- Lúcia da Conceição Andrade,
- Wellington Andraus ,
- Luís Augusto Carneiro D’Albuquerque ,
- Luíz Marcelo Sá Malbouisson
Views13ABSTRACT
Objective:
To explain the rationale and protocol of the methods and analyses to be used in the LIVER-PAM randomized clinical trial, which seeks to understand whether a higher mean arterial pressure is capable of reducing the incidence of renal dysfunction postoperatively after liver transplantation.
Methods:
LIVER-PAM is an open-label, randomized, controlled, singlecenter clinical trial. Patients randomized to the intervention group will have a mean arterial pressure of 85 – 90mmHg in the initial 24 hours of postoperative management, while patients in the control group will have a mean arterial pressure of 65 – 70mmHg in the same period. A sample of 174 patients will be required to demonstrate a 20% reduction in the absolute incidence of renal dysfunction, with a power of 80% and an alpha of 0.05.
Conclusion:
If a 20% reduction in the absolute incidence of renal dysfunction in the postoperative period of liver transplantation is achieved with higher target mean arterial pressure in the first 24 hours, this would represent an inexpensive and simple therapy for improving current outcomes in the management of liver transplant patients.
Keywords:Arterial pressureHemodynamicsLiver transplantationPerioperative carePostoperative periodRenal insufficiencySee more - Rodolpho Augusto de Moura Pedro
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more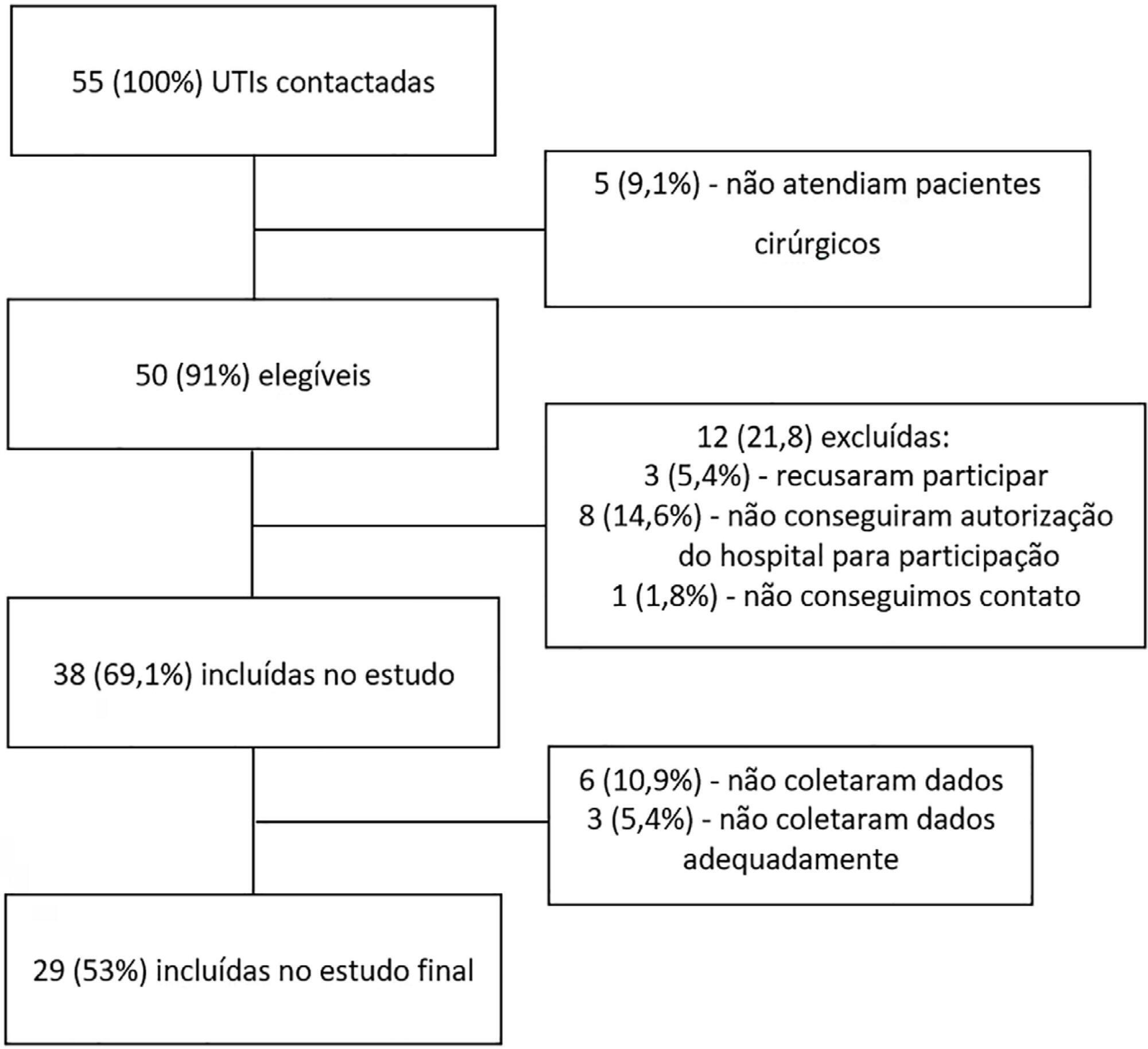
- João Manoel Silva Júnior
-
Commentaries
Intraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
Abstract
CommentariesIntraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
DOI 10.5935/0103-507X.20170065
Views0IntroductionPostoperative pulmonary complications are an important cause of hospital morbidity and mortality and are known to be associated with longer hospital stays and higher long-term mortality rates.() Thus, it is imperative to recognize early risk factors for the development of postoperative pulmonary complications (PPC) and to focus on the adoption of measures to prevent them […]See moreViews0Abstract
CommentariesIntraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
DOI 10.5935/0103-507X.20170065
Views0IntroductionPostoperative pulmonary complications are an important cause of hospital morbidity and mortality and are known to be associated with longer hospital stays and higher long-term mortality rates.() Thus, it is imperative to recognize early risk factors for the development of postoperative pulmonary complications (PPC) and to focus on the adoption of measures to prevent them […]See more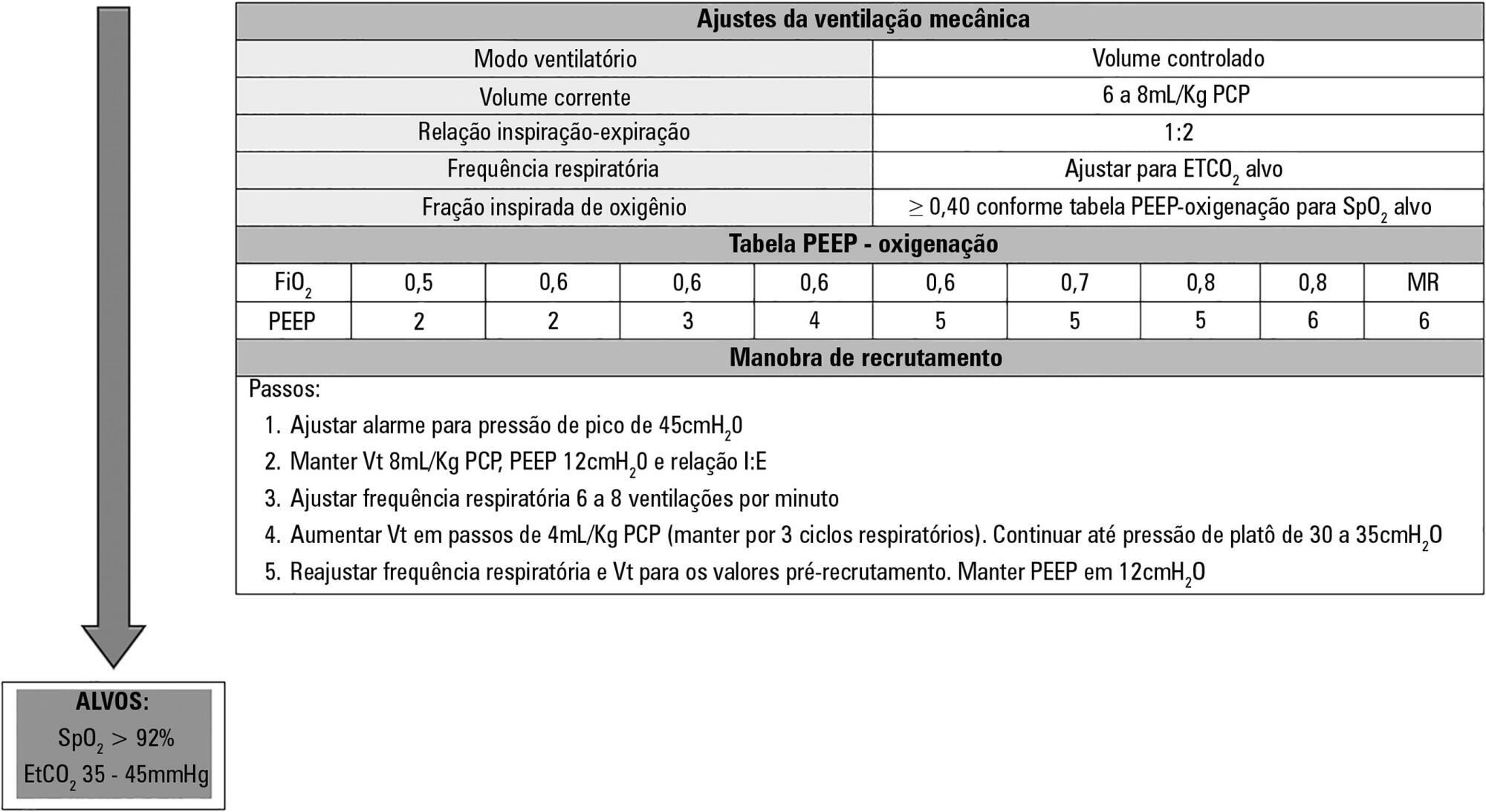
-
Special Article
Brazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views5See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Views5Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views5See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
-
Case Reports
Assistance of inhalation injury victims caused by fire in confined spaces: what we learned from the tragedy at Santa Maria
Rev Bras Ter Intensiva. 2014;26(4):421-429
Abstract
Case ReportsAssistance of inhalation injury victims caused by fire in confined spaces: what we learned from the tragedy at Santa Maria
Rev Bras Ter Intensiva. 2014;26(4):421-429
DOI 10.5935/0103-507X.20140065
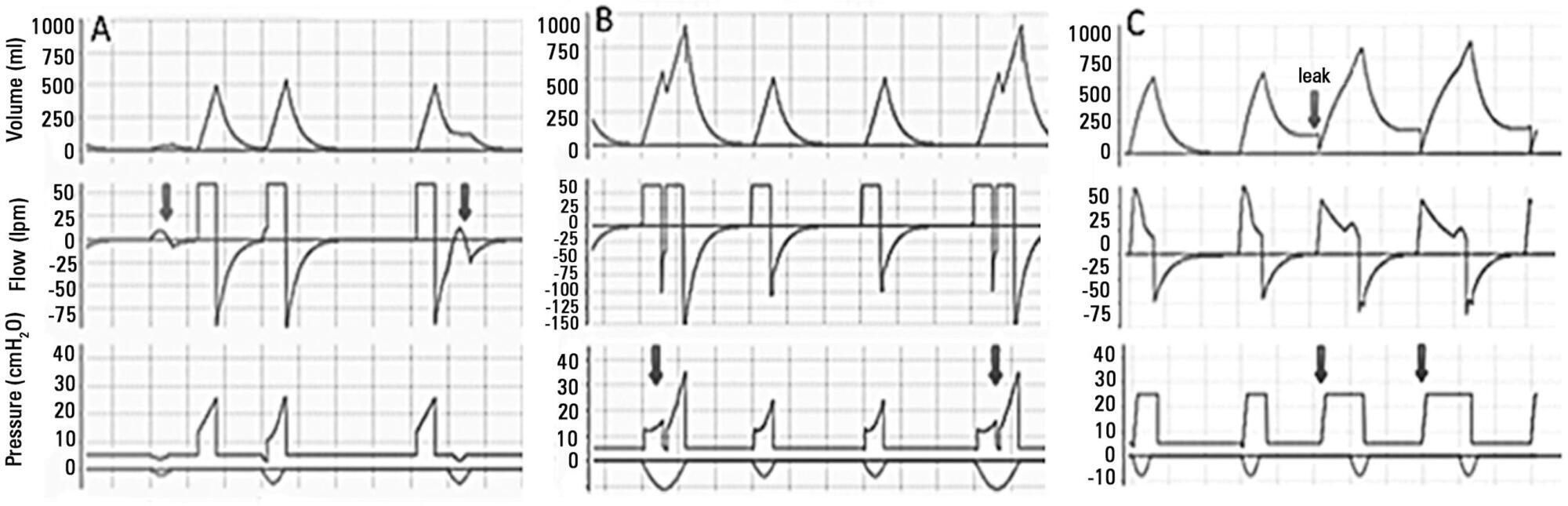
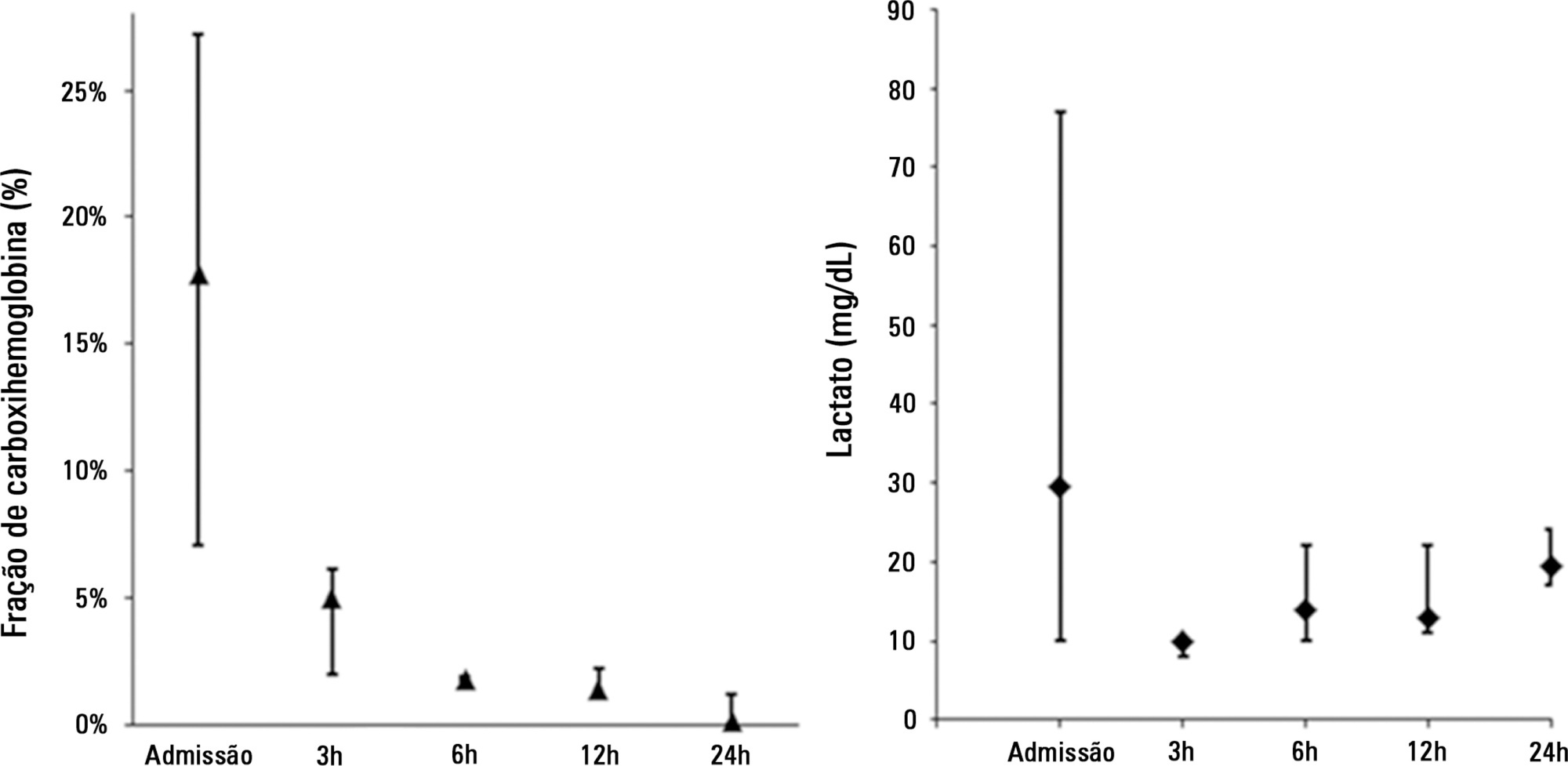
Views0See moreOn January 2013, a disaster at Santa Maria (RS) due to a fire in a confined space caused 242 deaths, most of them by inhalation injury. On November 2013, four individuals required intensive care following smoke inhalation from a fire at the Memorial da América Latina in São Paulo (SP). The present article reports the clinical progression and management of disaster victims presenting with inhalation injury. Patients ERL and OC exhibited early respiratory failure, bronchial aspiration of carbonaceous material, and carbon monoxide poisoning. Ventilation support was performed with 100% oxygen, the aspirated material was removed by bronchoscopy, and cyanide poisoning was empirically treated with sodium nitrite and sodium thiosulfate. Patient RP initially exhibited cough and retrosternal burning and subsequently progressed to respiratory failure due to upper airway swelling and early-onset pulmonary infection, which were treated with protective ventilation and antimicrobial agents. This patient was extubated following improvement of edema on bronchoscopy. Patient MA, an asthmatic, exhibited carbon monoxide poisoning and bronchospasm and was treated with normobaric hyperoxia, bronchodilators, and corticosteroids. The length of stay in the intensive care unit varied from four to 10 days, and all four patients exhibited satisfactory functional recovery. To conclude, inhalation injury has a preponderant role in fires in confined spaces. Invasive ventilation should not be delayed in cases with significant airway swelling. Hyperoxia should be induced early as a therapeutic means against carbon monoxide poisoning, in addition to empiric pharmacological treatment in suspected cases of cyanide poisoning.
Views0Abstract
Case ReportsAssistance of inhalation injury victims caused by fire in confined spaces: what we learned from the tragedy at Santa Maria
Rev Bras Ter Intensiva. 2014;26(4):421-429
DOI 10.5935/0103-507X.20140065
Views0See moreOn January 2013, a disaster at Santa Maria (RS) due to a fire in a confined space caused 242 deaths, most of them by inhalation injury. On November 2013, four individuals required intensive care following smoke inhalation from a fire at the Memorial da América Latina in São Paulo (SP). The present article reports the clinical progression and management of disaster victims presenting with inhalation injury. Patients ERL and OC exhibited early respiratory failure, bronchial aspiration of carbonaceous material, and carbon monoxide poisoning. Ventilation support was performed with 100% oxygen, the aspirated material was removed by bronchoscopy, and cyanide poisoning was empirically treated with sodium nitrite and sodium thiosulfate. Patient RP initially exhibited cough and retrosternal burning and subsequently progressed to respiratory failure due to upper airway swelling and early-onset pulmonary infection, which were treated with protective ventilation and antimicrobial agents. This patient was extubated following improvement of edema on bronchoscopy. Patient MA, an asthmatic, exhibited carbon monoxide poisoning and bronchospasm and was treated with normobaric hyperoxia, bronchodilators, and corticosteroids. The length of stay in the intensive care unit varied from four to 10 days, and all four patients exhibited satisfactory functional recovery. To conclude, inhalation injury has a preponderant role in fires in confined spaces. Invasive ventilation should not be delayed in cases with significant airway swelling. Hyperoxia should be induced early as a therapeutic means against carbon monoxide poisoning, in addition to empiric pharmacological treatment in suspected cases of cyanide poisoning.
-
Case Reports
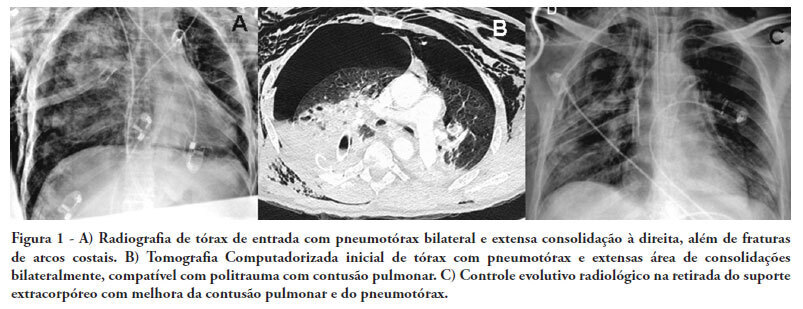
Hemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
Abstract
Case ReportsHemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
Views0See moreThere are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Views0Abstract
Case ReportsHemodynamic and respiratory support using venoarterial extracorporeal membrane oxygenation (ECMO) in a polytrauma patient
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
Views0See moreThere are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness ICU Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis