Acute Lung Injury Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(4):427-435
DOI 10.5935/0103-507X.20170067
To compare the effects of high-frequency oscillatory ventilation and conventional protective mechanical ventilation associated with the prone position on oxygenation, histology and pulmonary oxidative damage in an experimental model of acute lung injury.
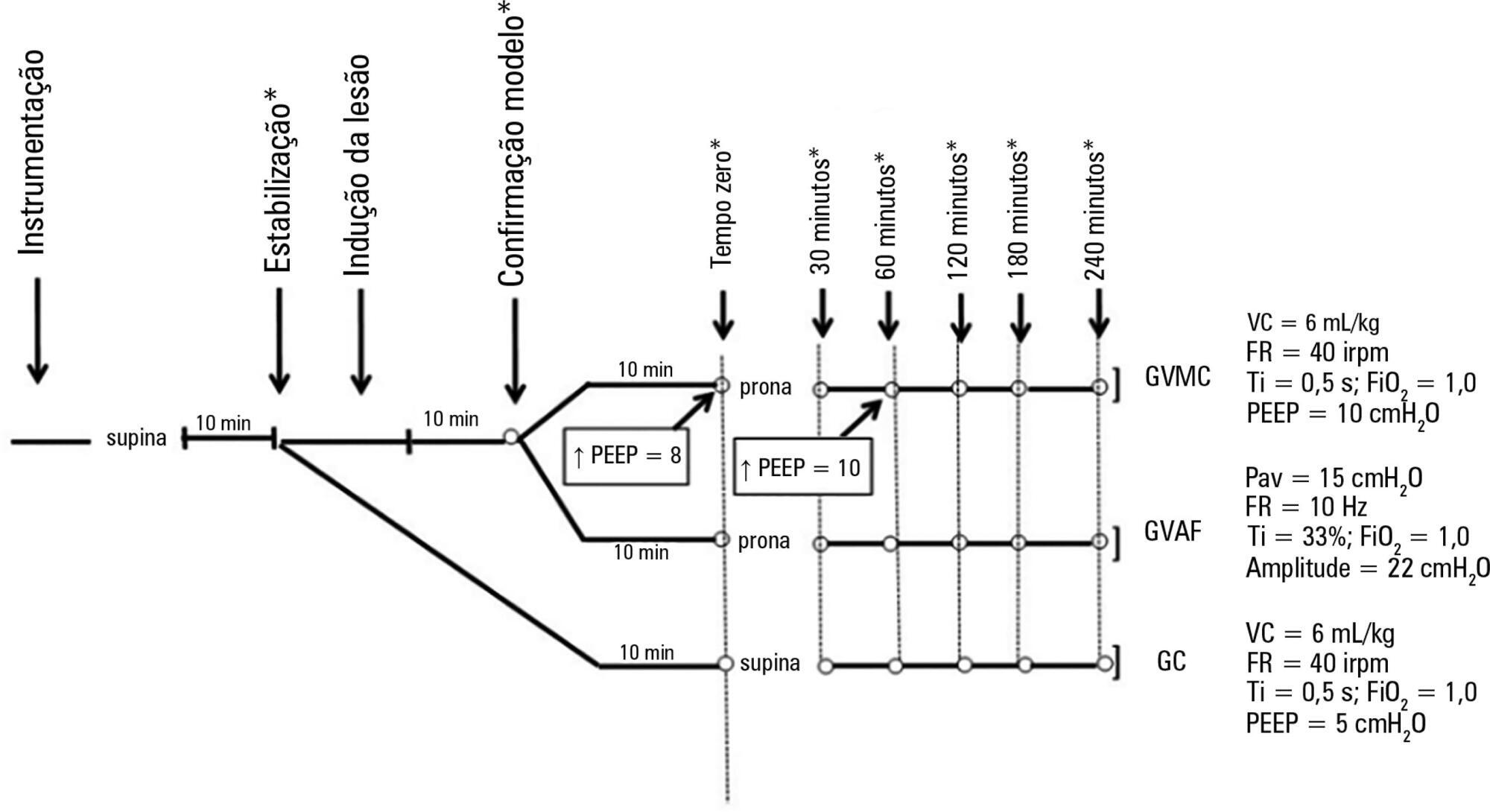
Forty-five rabbits with tracheostomy and vascular access were underwent mechanical ventilation. Acute lung injury was induced by tracheal infusion of warm saline. Three experimental groups were formed: healthy animals + conventional protective mechanical ventilation, supine position (Control Group; n = 15); animals with acute lung injury + conventional protective mechanical ventilation, prone position (CMVG; n = 15); and animals with acute lung injury + high-frequency oscillatory ventilation, prone position (HFOG; n = 15). Ten minutes after the beginning of the specific ventilation of each group, arterial gasometry was collected, with this timepoint being called time zero, after which the animal was placed in prone position and remained in this position for 4 hours. Oxidative stress was evaluated by the total antioxidant performance assay. Pulmonary tissue injury was determined by histopathological score. The level of significance was 5%.
Both groups with acute lung injury showed worsening of oxygenation after induction of injury compared with the Control Group. After 4 hours, there was a significant improvement in oxygenation in the HFOG group compared with CMVG. Analysis of total antioxidant performance in plasma showed greater protection in HFOG. HFOG had a lower histopathological lesion score in lung tissue than CMVG.
High-frequency oscillatory ventilation, associated with prone position, improves oxygenation and attenuates oxidative damage and histopathological lung injury compared with conventional protective mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):427-435
DOI 10.5935/0103-507X.20170067
To compare the effects of high-frequency oscillatory ventilation and conventional protective mechanical ventilation associated with the prone position on oxygenation, histology and pulmonary oxidative damage in an experimental model of acute lung injury.
Forty-five rabbits with tracheostomy and vascular access were underwent mechanical ventilation. Acute lung injury was induced by tracheal infusion of warm saline. Three experimental groups were formed: healthy animals + conventional protective mechanical ventilation, supine position (Control Group; n = 15); animals with acute lung injury + conventional protective mechanical ventilation, prone position (CMVG; n = 15); and animals with acute lung injury + high-frequency oscillatory ventilation, prone position (HFOG; n = 15). Ten minutes after the beginning of the specific ventilation of each group, arterial gasometry was collected, with this timepoint being called time zero, after which the animal was placed in prone position and remained in this position for 4 hours. Oxidative stress was evaluated by the total antioxidant performance assay. Pulmonary tissue injury was determined by histopathological score. The level of significance was 5%.
Both groups with acute lung injury showed worsening of oxygenation after induction of injury compared with the Control Group. After 4 hours, there was a significant improvement in oxygenation in the HFOG group compared with CMVG. Analysis of total antioxidant performance in plasma showed greater protection in HFOG. HFOG had a lower histopathological lesion score in lung tissue than CMVG.
High-frequency oscillatory ventilation, associated with prone position, improves oxygenation and attenuates oxidative damage and histopathological lung injury compared with conventional protective mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
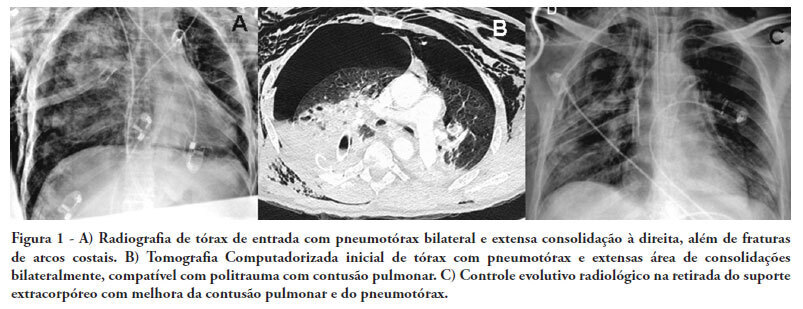
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):164-169
DOI 10.1590/S0103-507X2011000200008
OBJECTIVE: To evaluate the effects of hemodynamic, respiratory and metabolic changes on intracranial pressure in a model of acute lung injury and abdominal compartment syndrome. METHODS: Eight Agroceres pigs were submitted to five different clinical scenarios after instrumentation: 1) a baseline condition with low intra-abdominal pressure and healthy lungs; 2) pneumoperitoneum with 20 mmHg intra-abdominal pressure; 3) acute lung injury induced by pulmonary lavage with surfactant deactivation; 4) pneumoperitoneum with 20 mmHg intra-abdominal pressure with lung pulmonary injury and low positive end-expiratory pressure; and 5) 27 cmH2O positive end-expiratory pressure with pneumoperitoneum and acute lung injury. Respiratory and hemodynamic variables were collected. A multivariate analysis was conducted to search for variables associated with increased intracranial pressure in the five scenarios. RESULTS: Only plateau airway pressure showed a positive correlation with intracranial pressure in the multivariate analysis. In the models with acute lung injury, plateau airway pressure, CO2 arterial pressure, end tidal CO2 and central venous pressure were positively correlated with increased intracranial pressure. CONCLUSION: In a model of multiple organ dysfunction with associated clinical conditions causing increased intra-thoracic and abdominal pressure, increased intracranial pressure triggered by elevated intra-abdominal pressure is apparently caused by worsened respiratory system compliance and a reduced brain venous drainage gradient due to increased central venous pressure.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):41-48
DOI 10.1590/S0103-507X2011000100008
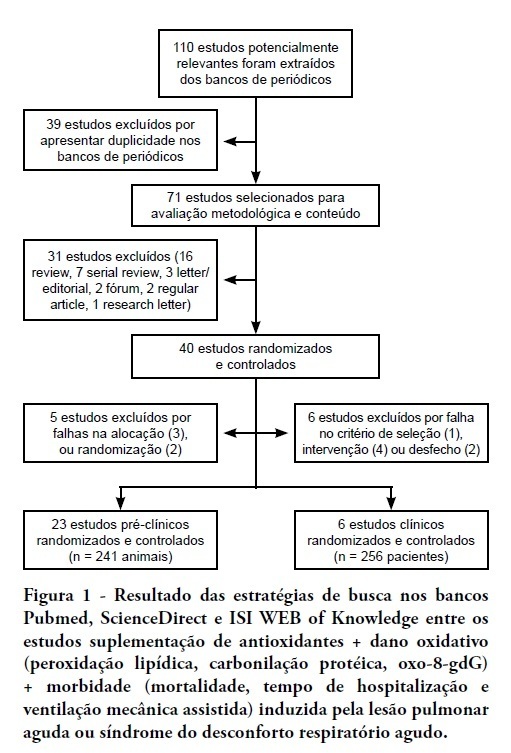
OBJECTIVE: This meta-analysis was performed to evaluate the evidence supporting antioxidant supplementation as an adjunct therapy to prevent oxidative damage and improve the clinical outcomes (mortality, length of hospital stay and duration of mechanical ventilation). METHODS: The search strategy for randomized controlled trials (RCTs) involved the participation of two researchers who independently assessed the methodological quality of each full-text article that was available in the PubMed, ISI WEB of Knowledge and ScienceDirect databases. RESULTS: We extracted 110 studies from the past 10 years, but only 30 articles met the methodological criteria (RCT, blinded and statistically significant results), for a total of 241 animals and 256 patients. This study found an odds ratio (OR) of 0.45 [95% confidence interval (CI): 0.26 to 0.79] for death in the experimental group compared with placebo (six trials, n = 256), an OR of 0.46 [95% CI: 0.26 to 0.87] for hospitalization time and an OR of 0.63 [95% CI: 0.35 to 1.12] for mechanical ventilation time between groups. CONCLUSION: Conflicting evidence makes it impossible to recommend the routine use of antioxidant supplementation in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):41-48
DOI 10.1590/S0103-507X2011000100008
OBJECTIVE: This meta-analysis was performed to evaluate the evidence supporting antioxidant supplementation as an adjunct therapy to prevent oxidative damage and improve the clinical outcomes (mortality, length of hospital stay and duration of mechanical ventilation). METHODS: The search strategy for randomized controlled trials (RCTs) involved the participation of two researchers who independently assessed the methodological quality of each full-text article that was available in the PubMed, ISI WEB of Knowledge and ScienceDirect databases. RESULTS: We extracted 110 studies from the past 10 years, but only 30 articles met the methodological criteria (RCT, blinded and statistically significant results), for a total of 241 animals and 256 patients. This study found an odds ratio (OR) of 0.45 [95% confidence interval (CI): 0.26 to 0.79] for death in the experimental group compared with placebo (six trials, n = 256), an OR of 0.46 [95% CI: 0.26 to 0.87] for hospitalization time and an OR of 0.63 [95% CI: 0.35 to 1.12] for mechanical ventilation time between groups. CONCLUSION: Conflicting evidence makes it impossible to recommend the routine use of antioxidant supplementation in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):384-394
DOI 10.1590/S0103-507X2010000400012
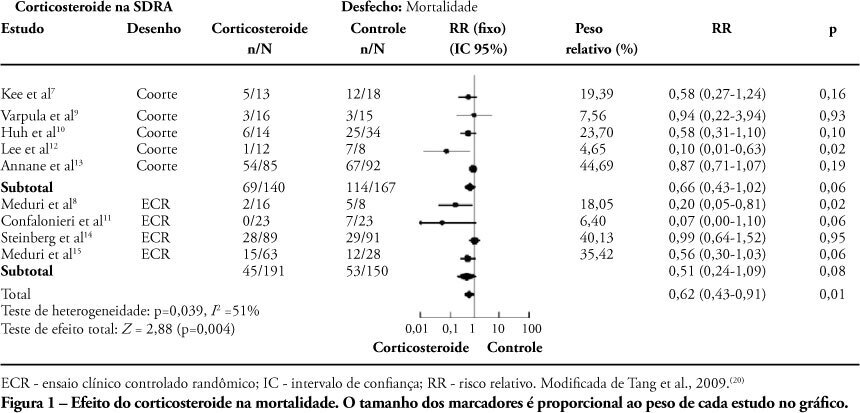
The use of corticosteroids in acute lung injury and acute respiratory distress syndrome is one of the most controversial issues in the literature. However, acute lung injury/acute respiratory distress syndrome studies are restricted to adults, despite the widespread use of corticosteroid for hyper-reactive respiratory airway diseases in children. This review aimed to describe experimental and clinical evidence for corticosteroid therapy in acute lung injury/acute respiratory distress syndrome and to point out the risks and benefits of its use in pediatrics. For this purpose, an extensive review of the literature was performed from 1980 to 2010 including both experimental and clinical papers, as well as reviews and meta-analysis, using Medline, Cochrane Central Register of Controlled Trials, Cochrane database of systematic reviews, SciELO, Lilacs and Bireme databases. The search terms were: acute lung injury, acute respiratory distress syndrome, steroids, child, clinical trials, meta-analyses, reviews, and case reports. Most studies showed that the corticosteroids-induced down-regulation of systemic inflammatory response is associated with oxygenation improvement, reduction of multiple organ dysfunctions, mechanical ventilation time, and intensive care units length of stay. Based on the literature, the authors suggest early and prolonged methylprednisolone administration for acute lung injury/acute respiratory distress syndrome, using continuous 1 mg/kg/day infusion to prevent glycemic variability, associated with strict infection surveillance. In addition, they recommend some diagnostic parameters, interventions and choices of endpoint variables to be adjusted to improve pediatric trials feasibility. Therefore, more research is required to establish the safety and efficacy of methylprednisolone in pediatric patients with acute lung injury/acute respiratory distress syndrome , as well as to determine the best parameters for monitoring steroid side effects and outcomes.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):384-394
DOI 10.1590/S0103-507X2010000400012
The use of corticosteroids in acute lung injury and acute respiratory distress syndrome is one of the most controversial issues in the literature. However, acute lung injury/acute respiratory distress syndrome studies are restricted to adults, despite the widespread use of corticosteroid for hyper-reactive respiratory airway diseases in children. This review aimed to describe experimental and clinical evidence for corticosteroid therapy in acute lung injury/acute respiratory distress syndrome and to point out the risks and benefits of its use in pediatrics. For this purpose, an extensive review of the literature was performed from 1980 to 2010 including both experimental and clinical papers, as well as reviews and meta-analysis, using Medline, Cochrane Central Register of Controlled Trials, Cochrane database of systematic reviews, SciELO, Lilacs and Bireme databases. The search terms were: acute lung injury, acute respiratory distress syndrome, steroids, child, clinical trials, meta-analyses, reviews, and case reports. Most studies showed that the corticosteroids-induced down-regulation of systemic inflammatory response is associated with oxygenation improvement, reduction of multiple organ dysfunctions, mechanical ventilation time, and intensive care units length of stay. Based on the literature, the authors suggest early and prolonged methylprednisolone administration for acute lung injury/acute respiratory distress syndrome, using continuous 1 mg/kg/day infusion to prevent glycemic variability, associated with strict infection surveillance. In addition, they recommend some diagnostic parameters, interventions and choices of endpoint variables to be adjusted to improve pediatric trials feasibility. Therefore, more research is required to establish the safety and efficacy of methylprednisolone in pediatric patients with acute lung injury/acute respiratory distress syndrome , as well as to determine the best parameters for monitoring steroid side effects and outcomes.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):469-474
DOI 10.1590/S0103-507X2007000400011
BACKGROUND AND OBJECTIVES: Mechanical ventilation is considered a basic element of life support in the intensive care unit and is essential for patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Experimental studies have demonstrated that mechanical ventilation with high volumes and/or high pressures can exacerbate (VALI) or induce lung injury (VILI) with histological aspect similar to ALI/ARDS. CONTENTS: This systematic review included the literature on MedLine and SciElo database published in the last 20 years. In this review, we will highlight the most recent data on the mechanisms of VILI. The main mechanisms of VILI are: volutrauma caused by overinflation and uneven expansion of the lungs due to high ventilation pressures or volumes; aletectrauma induced by shear forces generated during cyclic closure and reopening of terminal airways; and biotrauma where the injury resulted from the release inflammatory mediators due to physical stresses associated with mechanical ventilation. CONCLUSIONS: It is fundamental to understand the mechanisms related to volutrauma, atelectrauma, and biotrauma to avoid ventilator-associated lung injury.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):469-474
DOI 10.1590/S0103-507X2007000400011
BACKGROUND AND OBJECTIVES: Mechanical ventilation is considered a basic element of life support in the intensive care unit and is essential for patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Experimental studies have demonstrated that mechanical ventilation with high volumes and/or high pressures can exacerbate (VALI) or induce lung injury (VILI) with histological aspect similar to ALI/ARDS. CONTENTS: This systematic review included the literature on MedLine and SciElo database published in the last 20 years. In this review, we will highlight the most recent data on the mechanisms of VILI. The main mechanisms of VILI are: volutrauma caused by overinflation and uneven expansion of the lungs due to high ventilation pressures or volumes; aletectrauma induced by shear forces generated during cyclic closure and reopening of terminal airways; and biotrauma where the injury resulted from the release inflammatory mediators due to physical stresses associated with mechanical ventilation. CONCLUSIONS: It is fundamental to understand the mechanisms related to volutrauma, atelectrauma, and biotrauma to avoid ventilator-associated lung injury.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)