
You searched for:"Eduardo Leite Vieira Costa"
We found (9) results for your search.-
Original Article
Clinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
- Bruno Martins Tomazini
 ,
, - Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho , [ … ],
- Luciano César Pontes de Azevedo
Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee moreViews3

Abstract
Original ArticleClinical outcomes and lung mechanics characteristics between COVID-19 and non-COVID-19-associated acute respiratory distress syndrome: a propensity score analysis of two major randomized trials
Rev Bras Ter Intensiva. 2022;34(3):335-341
DOI 10.5935/0103-507X.20220040-en
- Bruno Martins Tomazini ,
- Eduardo Leite Vieira Costa ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fernando Godinho Zampieri ,
- Carlos Roberto Ribeiro de Carvalho ,
- Eliana Bernardete Caser,
- Vicente Cés de Souza-Dantas ,
- Emerson Boschi ,
- Renata Rego Lins Fumis ,
- Meton Soares de Alencar Filho ,
- Israel Silva Maia ,
- Wilson de Oliveira Filho ,
- Viviane Cordeiro Veiga ,
- Alvaro Avezum ,
- Renato Delascio Lopes ,
- Flávia Ribeiro Machado ,
- Otávio Berwanger ,
- Regis Goulart Rosa ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo
Views3ABSTRACT
Objective:
To compare the lung mechanics and outcomes between COVID-19-associated acute respiratory distress syndrome and non-COVID-19-associated acute respiratory distress syndrome.
Methods:
We combined data from two randomized trials in acute respiratory distress syndrome, one including only COVID-19 patients and the other including only patients without COVID-19, to determine whether COVID-19-associated acute respiratory distress syndrome is associated with higher 28-day mortality than non-COVID-19 acute respiratory distress syndrome and to examine the differences in lung mechanics between these two types of acute respiratory distress syndrome.
Results:
A total of 299 patients with COVID-19-associated acute respiratory distress syndrome and 1,010 patients with non-COVID-19-associated acute respiratory distress syndrome were included in the main analysis. The results showed that non-COVID-19 patients used higher positive end-expiratory pressure (12.5cmH2O; SD 3.2 versus 11.7cmH2O SD 2.8; p < 0.001), were ventilated with lower tidal volumes (5.8mL/kg; SD 1.0 versus 6.5mL/kg; SD 1.2; p < 0.001) and had lower static respiratory compliance adjusted for ideal body weight (0.5mL/cmH2O/kg; SD 0.3 versus 0.6mL/cmH2O/kg; SD 0.3; p = 0.01). There was no difference between groups in 28-day mortality (52.3% versus 58.9%; p = 0.52) or mechanical ventilation duration in the first 28 days among survivors (13 [IQR 5 – 22] versus 12 [IQR 6 – 26], p = 0.46).
Conclusion:
This analysis showed that patients with non-COVID-19-associated acute respiratory distress syndrome have different lung mechanics but similar outcomes to COVID-19-associated acute respiratory distress syndrome patients. After propensity score matching, there was no difference in lung mechanics or outcomes between groups.
Keywords:Coronavirus infectionsCOVID-19Critical careCritical care outcomesRespiratory distress syndromeRespiratory mechanicsSee more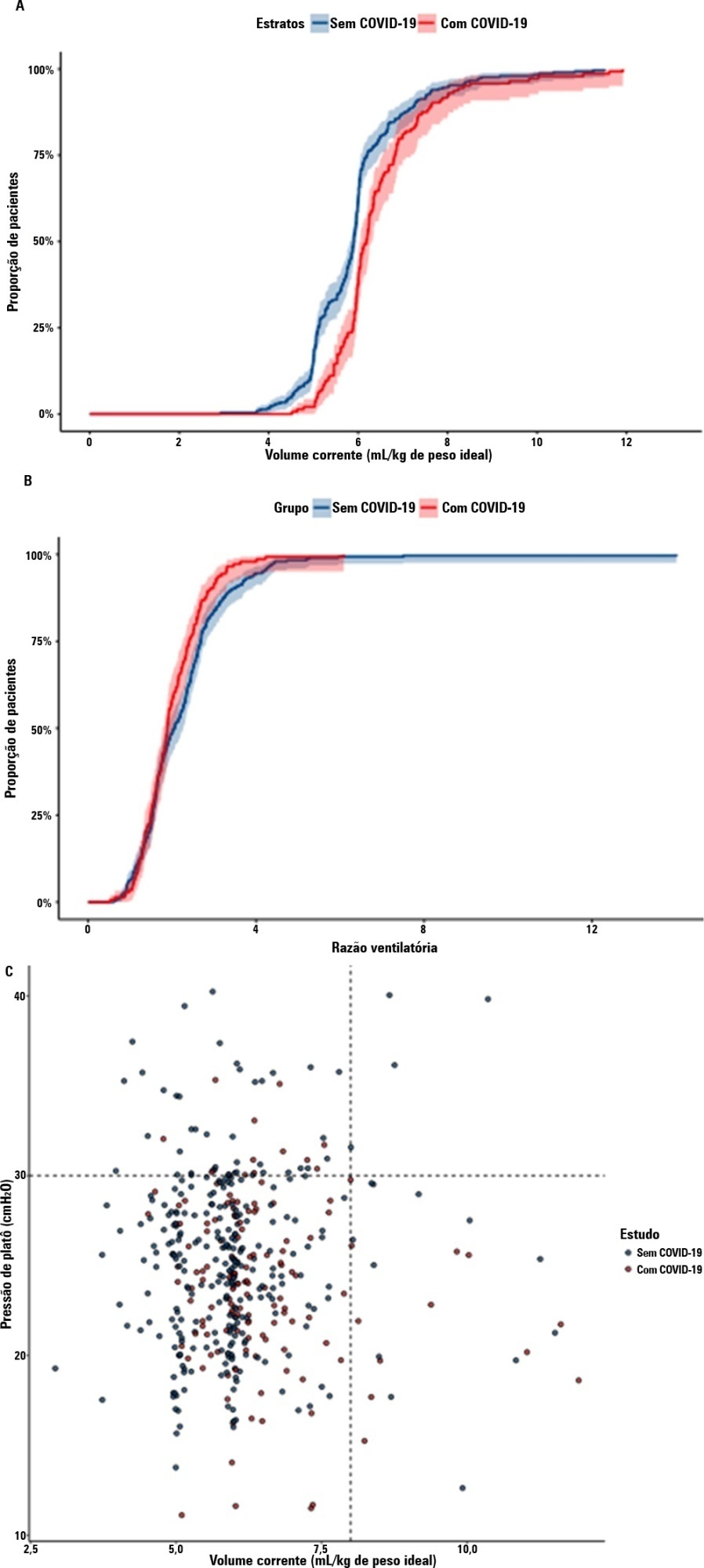
- Bruno Martins Tomazini
-
Original Article
COVID-19-associated ARDS treated with DEXamethasone (CoDEX): study design and rationale for a randomized trial
- Bruno Martins Tomazini ,
- Israel Silva Maia ,
- Flavia Regina Bueno,
- Maria Vitoria Aparecida Oliveira Silva,
- Franca Pellison Baldassare, [ … ],
Abstract
Original ArticleCOVID-19-associated ARDS treated with DEXamethasone (CoDEX): study design and rationale for a randomized trial
Rev Bras Ter Intensiva. 2020;32(3):354-362
DOI 10.5935/0103-507X.20200063
- Bruno Martins Tomazini ,
- Israel Silva Maia ,
- Flavia Regina Bueno,
- Maria Vitoria Aparecida Oliveira Silva,
- Franca Pellison Baldassare,
- Eduardo Leite Vieira Costa ,
- Ricardo Antonio Bonifácio Moura,
- Michele Ouriques Honorato,
- André Nathan Costa,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa,
- Álvaro Avezum,
- Viviane Cordeiro Veiga ,
- Renato Delascio Lopes,
- Lucas Petri Damiani,
- Flávia Ribeiro Machado,
- Otavio Berwanger,
- Luciano César Pontes de Azevedo ,
Views0Abstract
Objective:
The infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spreads worldwide and is considered a pandemic. The most common manifestation of SARS-CoV-2 infection (coronavirus disease 2019 – COVID-19) is viral pneumonia with varying degrees of respiratory compromise and up to 40% of hospitalized patients might develop acute respiratory distress syndrome. Several clinical trials evaluated the role of corticosteroids in non-COVID-19 acute respiratory distress syndrome with conflicting results. We designed a trial to evaluate the effectiveness of early intravenous dexamethasone administration on the number of days alive and free of mechanical ventilation within 28 days after randomization in adult patients with moderate or severe acute respiratory distress syndrome due to confirmed or probable COVID-19.
Methods:
This is a pragmatic, prospective, randomized, stratified, multicenter, open-label, controlled trial including 350 patients with early-onset (less than 48 hours before randomization) moderate or severe acute respiratory distress syndrome, defined by the Berlin criteria, due to COVID-19. Eligible patients will be randomly allocated to either standard treatment plus dexamethasone (Intervention Group) or standard treatment without dexamethasone (Control Group). Patients in the intervention group will receive dexamethasone 20mg intravenous once daily for 5 days, followed by dexamethasone 10mg IV once daily for additional 5 days or until intensive care unit discharge, whichever occurs first. The primary outcome is ventilator-free days within 28 days after randomization, defined as days alive and free from invasive mechanical ventilation. Secondary outcomes are all-cause mortality rates at day 28, evaluation of the clinical status at day 15 assessed with a 6-level ordinal scale, mechanical ventilation duration from randomization to day 28, Sequential Organ Failure Assessment Score evaluation at 48 hours, 72 hours and 7 days and intensive care unit -free days within 28.
Keywords:Adrenal cortex hormonesCoronavirusCOVID-19Critical careDexamethasoneRespiratory distress syndrome, adultSee moreViews0Abstract
Original ArticleCOVID-19-associated ARDS treated with DEXamethasone (CoDEX): study design and rationale for a randomized trial
Rev Bras Ter Intensiva. 2020;32(3):354-362
DOI 10.5935/0103-507X.20200063
- Bruno Martins Tomazini ,
- Israel Silva Maia ,
- Flavia Regina Bueno,
- Maria Vitoria Aparecida Oliveira Silva,
- Franca Pellison Baldassare,
- Eduardo Leite Vieira Costa ,
- Ricardo Antonio Bonifácio Moura,
- Michele Ouriques Honorato,
- André Nathan Costa,
- Alexandre Biasi Cavalcanti ,
- Regis Goulart Rosa,
- Álvaro Avezum,
- Viviane Cordeiro Veiga ,
- Renato Delascio Lopes,
- Lucas Petri Damiani,
- Flávia Ribeiro Machado,
- Otavio Berwanger,
- Luciano César Pontes de Azevedo ,
Views0Abstract
Objective:
The infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spreads worldwide and is considered a pandemic. The most common manifestation of SARS-CoV-2 infection (coronavirus disease 2019 – COVID-19) is viral pneumonia with varying degrees of respiratory compromise and up to 40% of hospitalized patients might develop acute respiratory distress syndrome. Several clinical trials evaluated the role of corticosteroids in non-COVID-19 acute respiratory distress syndrome with conflicting results. We designed a trial to evaluate the effectiveness of early intravenous dexamethasone administration on the number of days alive and free of mechanical ventilation within 28 days after randomization in adult patients with moderate or severe acute respiratory distress syndrome due to confirmed or probable COVID-19.
Methods:
This is a pragmatic, prospective, randomized, stratified, multicenter, open-label, controlled trial including 350 patients with early-onset (less than 48 hours before randomization) moderate or severe acute respiratory distress syndrome, defined by the Berlin criteria, due to COVID-19. Eligible patients will be randomly allocated to either standard treatment plus dexamethasone (Intervention Group) or standard treatment without dexamethasone (Control Group). Patients in the intervention group will receive dexamethasone 20mg intravenous once daily for 5 days, followed by dexamethasone 10mg IV once daily for additional 5 days or until intensive care unit discharge, whichever occurs first. The primary outcome is ventilator-free days within 28 days after randomization, defined as days alive and free from invasive mechanical ventilation. Secondary outcomes are all-cause mortality rates at day 28, evaluation of the clinical status at day 15 assessed with a 6-level ordinal scale, mechanical ventilation duration from randomization to day 28, Sequential Organ Failure Assessment Score evaluation at 48 hours, 72 hours and 7 days and intensive care unit -free days within 28.
Keywords:Adrenal cortex hormonesCoronavirusCOVID-19Critical careDexamethasoneRespiratory distress syndrome, adultSee more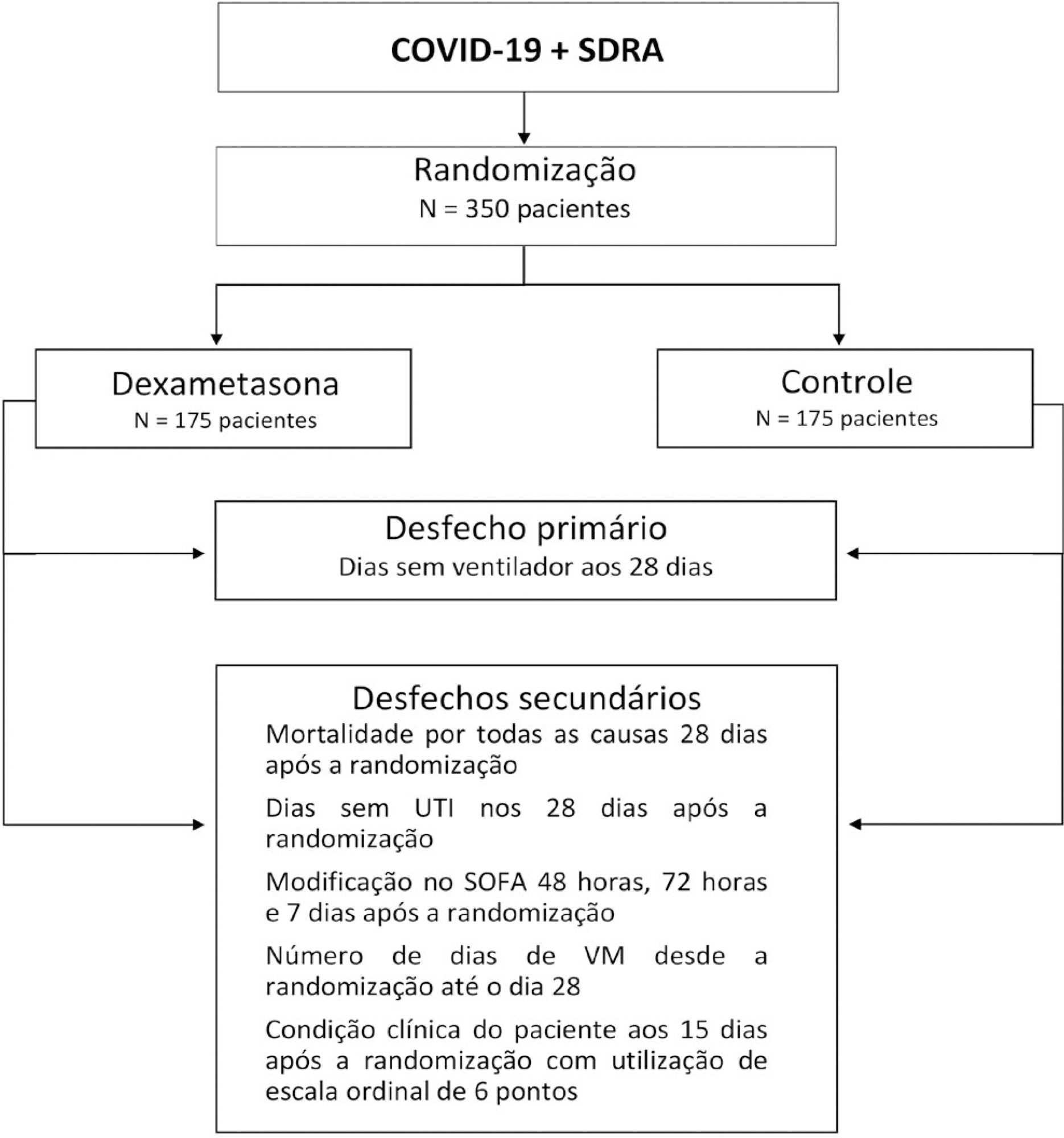
- Bruno Martins Tomazini
-
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
Abstract
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
Views0ABSTRACT
Objective:
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
Methods:
The factors associated with oxygen – and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Results:
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
Conclusion:
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Keywords:Extracorporeal membrane oxygenationRespiration, artificialRespiratory distress syndrome, adultSwineSee moreViews0Abstract
Factors associated with blood oxygen partial pressure and carbon dioxide partial pressure regulation during respiratory extracorporeal membrane oxygenation support: data from a swine model
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
Views0ABSTRACT
Objective:
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
Methods:
The factors associated with oxygen – and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Results:
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
Conclusion:
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Keywords:Extracorporeal membrane oxygenationRespiration, artificialRespiratory distress syndrome, adultSwineSee more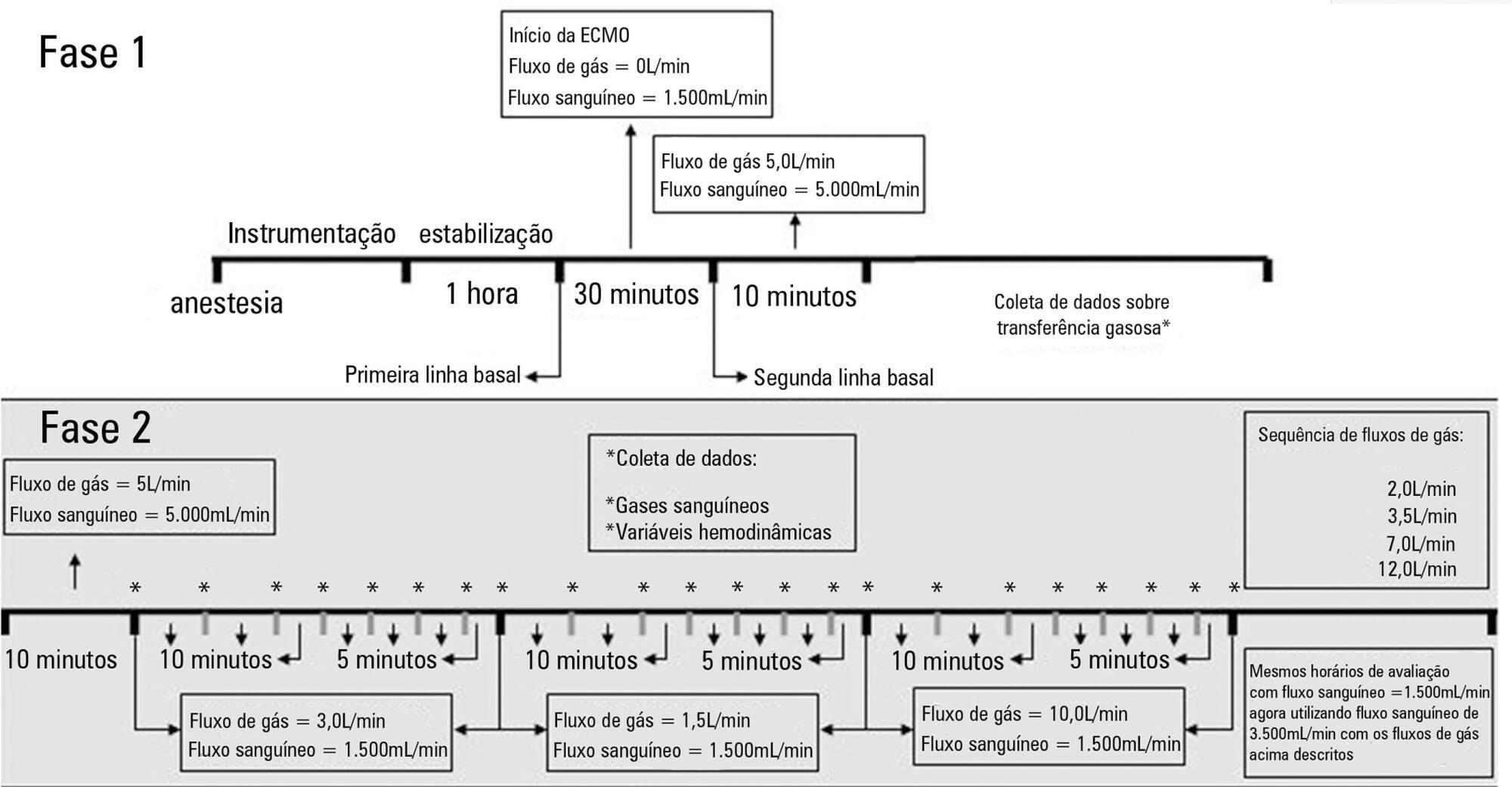
-
Original Articles
Blood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
Abstract
Original ArticlesBlood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
Views0ABSTRACT
Objective:
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Methods:
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
Results:
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = – 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Conclusion:
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee moreViews0Abstract
Original ArticlesBlood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
Views0ABSTRACT
Objective:
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Methods:
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
Results:
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = – 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Conclusion:
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee more
-
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
Abstract
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
DOI 10.5935/0103-507X.20150052
Views0Myocardial dysfunction in sepsis is a complex entity due to the dynamic adaptation of the cardiovascular system to the disease process, the host response, and the effects of resuscitation. The pathophysiology of this entity is multifactorial; systemic, cellular, and extracellular mechanisms have been described, including maldistribution of coronary blood flow, myocardial injury, complement-triggered (C5a) myocyte […]See moreViews0Abstract
A look at the diastolic function in severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):307-308
DOI 10.5935/0103-507X.20150052
Views0Myocardial dysfunction in sepsis is a complex entity due to the dynamic adaptation of the cardiovascular system to the disease process, the host response, and the effects of resuscitation. The pathophysiology of this entity is multifactorial; systemic, cellular, and extracellular mechanisms have been described, including maldistribution of coronary blood flow, myocardial injury, complement-triggered (C5a) myocyte […]See more -
Original Articles
Is the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
Abstract
Original ArticlesIs the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
DOI 10.5935/0103-507X.20140001
Views1Objective:
To evaluate the satisfaction of the intensive care unit staff with a computerized physician order entry and to compare the concept of the computerized physician order entry relevance among intensive care unit healthcare workers.
Methods:
We performed a cross-sectional survey to assess the satisfaction of the intensive care unit staff with the computerized physician order entry in a 30-bed medical/surgical adult intensive care unit using a self-administered questionnaire. The questions used for grading satisfaction levels were answered according to a numerical scale that ranged from 1 point (low satisfaction) to 10 points (high satisfaction).
Results:
The majority of the respondents (n=250) were female (66%) between the ages of 30 and 35 years of age (69%). The overall satisfaction with the computerized physician order entry scored 5.74±2.14 points. The satisfaction was lower among physicians (n=42) than among nurses, nurse technicians, respiratory therapists, clinical pharmacists and diet specialists (4.62±1.79 versus 5.97±2.14, p<0.001); satisfaction decreased with age (p<0.001). Physicians scored lower concerning the potential of the computerized physician order entry for improving patient safety (5.45±2.20 versus 8.09±2.21, p<0.001) and the ease of using the computerized physician order entry (3.83±1.88 versus 6.44±2.31, p<0.001). The characteristics independently associated with satisfaction were the system's user-friendliness, accuracy, capacity to provide clear information, and fast response time.
Conclusion:
Six months after its implementation, healthcare workers were satisfied, albeit not entirely, with the computerized physician order entry. The overall users’ satisfaction with computerized physician order entry was lower among physicians compared to other healthcare professionals. The factors associated with satisfaction included the belief that digitalization decreased the workload and contributed to the intensive care unit quality with a user-friendly and accurate system and that digitalization provided concise information within a reasonable time frame.
Keywords:Attitude of health personnelHealth care surveysJob satisfactionMedical order entry systemPhysician practice patternsSee moreViews1Abstract
Original ArticlesIs the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
DOI 10.5935/0103-507X.20140001
Views1Objective:
To evaluate the satisfaction of the intensive care unit staff with a computerized physician order entry and to compare the concept of the computerized physician order entry relevance among intensive care unit healthcare workers.
Methods:
We performed a cross-sectional survey to assess the satisfaction of the intensive care unit staff with the computerized physician order entry in a 30-bed medical/surgical adult intensive care unit using a self-administered questionnaire. The questions used for grading satisfaction levels were answered according to a numerical scale that ranged from 1 point (low satisfaction) to 10 points (high satisfaction).
Results:
The majority of the respondents (n=250) were female (66%) between the ages of 30 and 35 years of age (69%). The overall satisfaction with the computerized physician order entry scored 5.74±2.14 points. The satisfaction was lower among physicians (n=42) than among nurses, nurse technicians, respiratory therapists, clinical pharmacists and diet specialists (4.62±1.79 versus 5.97±2.14, p<0.001); satisfaction decreased with age (p<0.001). Physicians scored lower concerning the potential of the computerized physician order entry for improving patient safety (5.45±2.20 versus 8.09±2.21, p<0.001) and the ease of using the computerized physician order entry (3.83±1.88 versus 6.44±2.31, p<0.001). The characteristics independently associated with satisfaction were the system's user-friendliness, accuracy, capacity to provide clear information, and fast response time.
Conclusion:
Six months after its implementation, healthcare workers were satisfied, albeit not entirely, with the computerized physician order entry. The overall users’ satisfaction with computerized physician order entry was lower among physicians compared to other healthcare professionals. The factors associated with satisfaction included the belief that digitalization decreased the workload and contributed to the intensive care unit quality with a user-friendly and accurate system and that digitalization provided concise information within a reasonable time frame.
Keywords:Attitude of health personnelHealth care surveysJob satisfactionMedical order entry systemPhysician practice patternsSee more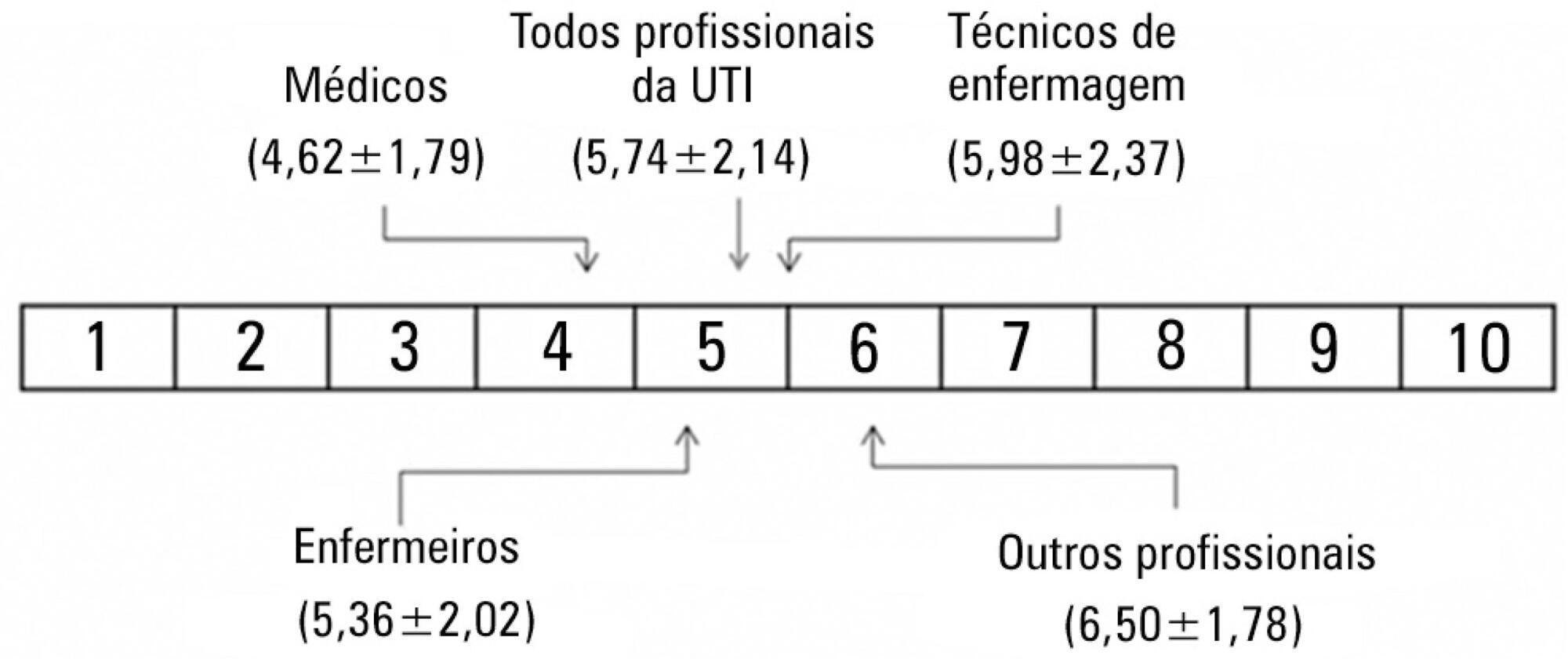
-
Original Article
The economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
Abstract
Original ArticleThe economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
Views0Objective:
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
Methods:
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
Results:
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
Conclusion:
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Keywords:Costs and cost analysisExtracorporeal membrane oxygenation/economyIntensive care unitsRespiration, artificialRespiratory insufficiencySee moreViews0Abstract
Original ArticleThe economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
Views0Objective:
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
Methods:
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
Results:
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
Conclusion:
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Keywords:Costs and cost analysisExtracorporeal membrane oxygenation/economyIntensive care unitsRespiration, artificialRespiratory insufficiencySee more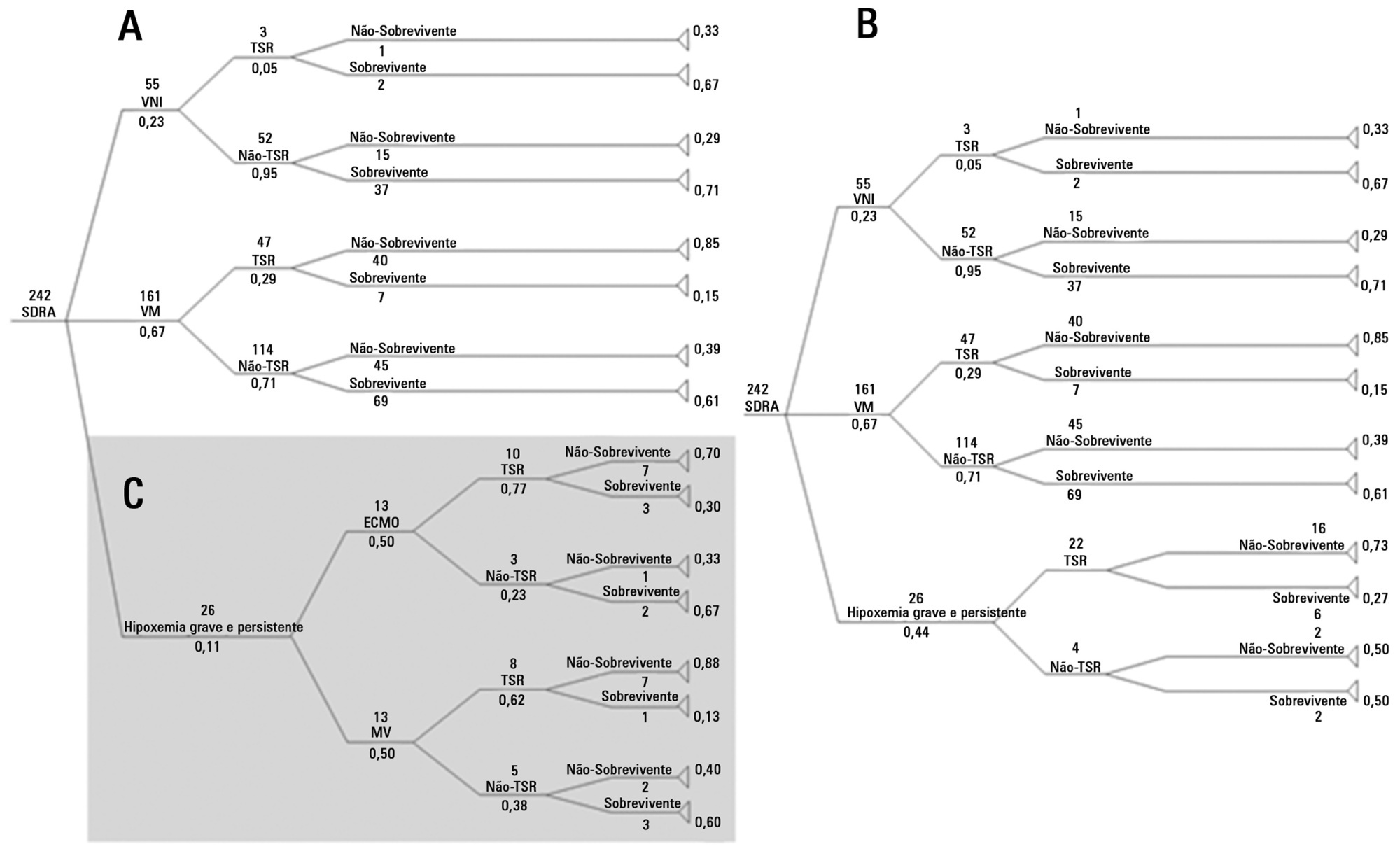
-
Original Articles – Basic Research
Acute hemodynamic, respiratory and metabolic alterations after blood contact with a volume priming and extracorporeal life support circuit: an experimental study
Rev Bras Ter Intensiva. 2012;24(2):137-142
Abstract
Original Articles – Basic ResearchAcute hemodynamic, respiratory and metabolic alterations after blood contact with a volume priming and extracorporeal life support circuit: an experimental study
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
Views0OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee moreViews0Abstract
Original Articles – Basic ResearchAcute hemodynamic, respiratory and metabolic alterations after blood contact with a volume priming and extracorporeal life support circuit: an experimental study
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
Views0OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee more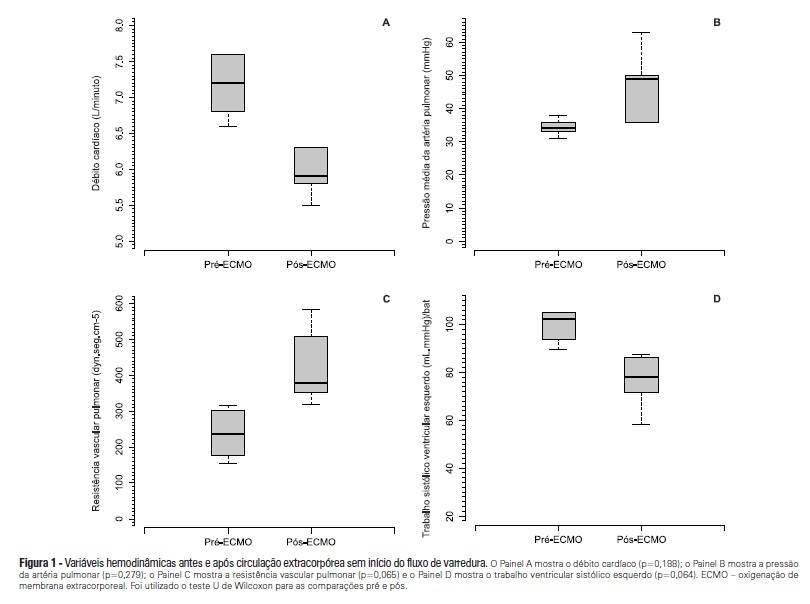
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis